



Introduction
A plethora of studies provide evidence of family relationships’ key role in individuals’ wellbeing and health across the entire lifecourse and particularly at older ages (Thomas et al., Reference Thomas, Liu and Umberson2017; see also Umberson and Thomeer, Reference Umberson and Thomeer2020). Importantly, health and wellbeing in later life are not only influenced by older adults’ current family relationships (e.g. Milkie et al., Reference Milkie, Bierman and Schieman2008; Arpino et al., Reference Arpino, Bordone and Balbo2018), but also by the ‘long (and cumulative) arm’ of family ties during earlier stages of the lifecourse (e.g. Chen et al., Reference Chen, Brody and Miller2017).
Next to the quality of these relationships (e.g. Merz et al., Reference Merz, Consedine, Schulze and Schuengel2009; Damri and Litwin, Reference Damri, Litwin, Börsch-Supan, Bristle, Andersen-Ranberg, Brugiavini, Jusot, Litwin and Weber2019), even the mere presence or absence of family relations – as a ‘kinship reservoir’ or, more generally, a ‘relational reserve’ – might matter (e.g. McIlvane et al., Reference McIlvane, Ajrouch and Antonucci2007; Cullati et al., Reference Cullati, Kliegel and Widmer2018). Because transitions into or out of kin relationships shape and change individuals’ roles as well as the basic opportunity structure for social interaction and the exchange of support within families (e.g. Umberson et al., Reference Umberson, Crosnoe and Reczek2010; Sauter et al., Reference Sauter, Widmer and Kliegel2023), their occurrence and timing during the lifecourse have been investigated as potential predictors of individuals’ subsequent wellbeing and health (e.g. Williams et al., Reference Williams, Sassler, Addo and Frech2015; Di Gessa et al., Reference Di Gessa, Bordone and Arpino2020).
One important shortcoming in much of the previous literature is its focus on how singular family role transitions, such as losing a parent (e.g. Leopold and Lechner, Reference Leopold and Lechner2015), entering parenthood (e.g. Mirowsky, Reference Mirowsky2005) or becoming a first-time grandparent (e.g. Sheppard and Monden, Reference Sheppard and Monden2019), affect health and wellbeing. However, across the lifecourse, most individuals actually experience multiple such transitions (the loss of parents and the birth of children or even grandchildren). Moreover, each of these transitions constitutes more than just a change in a specific dyadic relationship, but occurs within a family system (e.g. Fingerman and Bermann, Reference Fingerman and Bermann2000). Taking a family systems rather than a dyadic perspective is consequential, because next to merely assessing direct associations between particular role transitions and health outcomes, we are then also able to consider such transitions’ indirect relationship with wellbeing resulting from ‘spillovers’ to other family ties: both the birth and the death of family members affect, for example, individuals’ generational placement and have been shown to impact multigenerational relationship qualities in the family system (e.g. Tanskanen, Reference Tanskanen2017; Kim et al., Reference Kim, Kim, Boerner, Birditt, Zarit and Fingerman2019).
We enhance previous research by addressing the question of whether and how the occurrence, timing and ordering of transitions into and out of multiple kin relations and family roles across the lifecourse relate to individuals’ later-life wellbeing and health. Our study thus primarily takes a lifecourse perspective (e.g. Elder, Reference Elder1994; George, Reference George and Settersten2003; Shuey and Willson, Reference Shuey, Willson and Cockerham2021), but also speaks to – and integrates – role theory and family systems theory. Taken together, these approaches suggest that individuals are embedded in a dynamic family system, in which the individual might take on multiple social roles and which constitutes a ‘kinship reservoir’ that can change over the lifecourse.
[One’s] kinship reservoir refers to a pool of relatives present in the focal individual’s life, whether they are significant family members of the focal individual or not … The family ties that constitute this reserve can be activated, reactivated or deactivated over the lifecourse, depending on the current needs of the focal individual. (Sauter et al., Reference Sauter, Widmer and Kliegel2023: 726)
This does not apply to relationships with intimate partners, though. While acknowledging the importance of partnership histories for individuals’ health (e.g. Kravdal et al., Reference Kravdal, Grundy, Lyngstad and Wiik2012; Williams et al., Reference Williams, Sassler, Addo and Frech2015), the current investigation therefore focuses on intergenerational relations. Moreover, we propose that this ‘bundle’ rather than one specific (dyadic) kin relation or family role transition at a particular point in time should be considered as a driver of later-life health and wellbeing.
Accordingly, our study builds on recent work by Hünteler (Reference Hünteler2022), who empirically identified distinct clusters of ‘generational placement trajectories’. These clusters reflect typical patterns and dynamics of the structural availability of intergenerational family relations – the ‘kinship reservoir’ of parents, children and grandchildren – across individual lifecourses: some experience a trajectory with barely any change in their generational placement (merely losing their role as a child when their parents die, but never entering parenthood or grandparenthood), whereas others find themselves moving up the ‘generational ladder’ – from being a child to being a parent to being a grandparent – at great speed, maintaining several intergenerational family roles at the same time. Generational placement trajectories thus efficiently describe the vertical position of individuals in relation to other living generations in their family over time. This comprehensive and dynamic approach captures simultaneously the occurrence, timing and ordering of transitions into or out of multiple intergenerational family roles, enabling us to explore their joint association with individuals’ later-life wellbeing and health.
Our analysis is based on two cross-sectional rounds of the German Ageing Survey (DEAS; Klaus et al., Reference Klaus, Engstler, Mahne, Wolff, Simonson, Wurm and Tesch-Römer2017), collected in 2008 and 2014, whose data not only provide rich retrospective information on respondents’ family biographies, but also an array of current wellbeing- and health-related measures. These allow us to assess four distinct physical and psychological aspects of the multi-dimensional concepts of health and wellbeing (potentially bearing different associations with the generational placement trajectories), namely life satisfaction (as an indicator of subjective wellbeing), depressiveness (as an indicator of psychological distress), functional limitations (as an indicator of the individual’s inability to perform specific tasks) and physical health problems (such as respiratory problems, cancer or insomnia). Because both the generational placement trajectories as well as wellbeing and health are influenced by an individual’s socio-economic characteristics, such as education and gender, we conduct not only bivariate regression models but subsequently also control for differences in the socio-economic status.
Theoretical and empirical background
The lifecourse perspective
Over their lifecourse, individuals can experience a multitude of family transitions triggering changes in social status and family roles. Individual transitions are considered to be embedded within larger (long-term) trajectories that are shaped by the occurrence, timing and ordering of multiple such events. Differences in these trajectories might result in varying (long-term) consequences of the same social phenomenon across groups of individuals. Thus, life histories rather than singular life events have been considered in studies investigating family transitions’ and positions’ contribution to shaping individuals’ later-life health (see also Gilligan et al., Reference Gilligan, Karraker and Jasper2018; e.g. Kravdal et al., Reference Kravdal, Grundy, Lyngstad and Wiik2012). Speaking to the lifecourse principle of timing (Elder, Reference Elder1994), non-normative or ‘off-time’ transitions (trajectories, respectively) – such as early parenthood or the early death of a parent – are of particular interest because of their potentially negative health implications (e.g. George, Reference George and Settersten2003): (how) does it matter for later-life wellbeing and health, whether, and for how long, one (still) has parents (e.g. Marks et al., Reference Marks, Jun and Song2007; Leopold and Lechner, Reference Leopold and Lechner2015; Kamis et al., Reference Kamis, Stolte and Copeland2022) or whether, and when, one has children (e.g. Mirowsky, Reference Mirowsky2005; Nomaguchi and Milkie, Reference Nomaguchi and Milkie2020) or grandchildren (e.g. Sheppard and Monden, Reference Sheppard and Monden2019; Di Gessa et al., Reference Di Gessa, Bordone and Arpino2020)?
Moreover, the lifecourse principle of linked lives is also fundamental to our study. Arguably, families constitute the most proximate social context within which individual pathways are embedded:
A classic example of the effects that the transition of one family member has on other members can be seen in the transition to parenthood, which creates a counter-transition … to grandparenthood for the older generation … The timing and quality of shared transitions and experiences have ripple effects … on the lives of other members of the family unit beyond just the individual at its epicenter, similar to a pebble … dropped into a pond. (Shuey and Willson, Reference Shuey, Willson and Cockerham2021: 179, italics in the original)
The lifecourse perspective is thus closely related to family systems theory, in which family ties are conceptualised as sets of interdependent, reciprocally influential subsystems (e.g. Fingerman and Bermann, Reference Fingerman and Bermann2000). Along these lines, recent studies have pointed to the importance of accounting for individuals’ ‘embeddedness’ in multiple simultaneous kin relations to advance our understanding of how family functions as a principal determinant of adult health and wellbeing (see Kim et al., Reference Kim, Kim, Boerner, Birditt, Zarit and Fingerman2019; Patterson et al., Reference Patterson, Margolis and Verdery2020a).
Intergenerational family roles and wellbeing: underlying mechanisms
Various mechanisms have been discussed to explain the nexus between intergenerational family positions and wellbeing and health (see e.g. Sheppard and Monden, Reference Sheppard and Monden2019), but role theory is a particularly obvious candidate: it proposes that transitions into new social roles may affect individuals’ health and wellbeing in both positive (role enhancement) or negative (role strain) ways. Because each role is usually associated with both demands and rewards (Nomaguchi and Milkie, Reference Nomaguchi and Milkie2020), its net effect is difficult to determine a priori – and predictions become even more difficult if multiple roles are considered simultaneously (e.g. Reid and Hardy, Reference Reid and Hardy1999). Especially in middle-adulthood, individuals may be placed in an intergenerational ‘sandwich’ position (e.g. Grundy and Henretta, Reference Grundy and Henretta2006; Wiemers and Bianchi, Reference Wiemers and Bianchi2015), whose specific challenges and risks of role strain have been shown to be associated with wellbeing and health (e.g. Do et al., Reference Do, Cohen and Brown2014; Hodgdon and Wong, Reference Hodgdon and Wong2019). Such consideration of multiple simultaneous family roles corresponds to a perspective stressing the importance of accounting for individuals ‘embeddedness’ in the family system and their interconnectedness throughout their lives (linked lives) as a determinant of adult health and wellbeing (see Kim et al., Reference Kim, Kim, Boerner, Birditt, Zarit and Fingerman2019; Patterson et al., Reference Patterson, Margolis and Verdery2020a). Moreover, it might be relevant if transitions into and out of these family roles are experienced ‘on-time’, that is in accordance with the normative expectation (timing).
Next to role theory, the concept of the kinship reservoir, a sub-form of relational reserves that reflects a dimension of social capital, contributes to explaining how the vertical position within the family system might be associated with an individual’s wellbeing and health (Cullati et al., Reference Cullati, Kliegel and Widmer2018). A reserve (in contrast to resources) can be understood as a more indirect source of support to overcome adverse life events. Throughout the lifecourse, the relational reserve can change in density or size. Considering intergenerational biological families, the reserve increases upon the birth of a child or grandchild and decreases when one’s parents die. The larger the reserve, the more potential there is to turn its elements into active ties who support an individual in times of need. Thus, having more family members along vertical lines may enhance later-life health and wellbeing. Conversely, lack of intergenerational family ties constitutes a specific form of vulnerability which may reduce an individual’s wellbeing and health (Cullati et al., Reference Cullati, Kliegel and Widmer2018).
Intergenerational family roles and wellbeing: previous empirical findings
Ample research has investigated associations between transitions into or out of specific family roles (affecting one’s generational placement) and individuals’ health and wellbeing. Parental death, for example, has been shown to be associated with drops in life satisfaction (Leopold and Lechner, Reference Leopold and Lechner2015) as well as declining mental and physical wellbeing (Marks et al., Reference Marks, Jun and Song2007; Kamis et al., Reference Kamis, Stolte and Copeland2022). Importantly, negative effects appear to be stronger if adult children lose a parent ‘off-time’, that is, at younger ages (Leopold and Lechner, Reference Leopold and Lechner2015; Kamis et al., Reference Kamis, Stolte and Copeland2022).
Studies investigating associations between parenthood and wellbeing and health across the lifecourse (e.g. Nomaguchi and Milkie, Reference Nomaguchi and Milkie2020; Quashie et al., Reference Quashie, Arpino, Antczak and Mair2021) cover a broad range of outcomes, ranging from life satisfaction and happiness (e.g. Myrskylä and Margolis, Reference Myrskylä and Margolis2014; Pollmann-Schult, Reference Pollmann-Schult2014) to mortality (e.g. Henretta, Reference Henretta2007; Kravdal et al., Reference Kravdal, Grundy, Lyngstad and Wiik2012). Specifically, having had an ‘early’ first birth has been found to be associated with subsequent lower quality of life and lower (self-rated) general health (e.g. Mirowsky, Reference Mirowsky2005; Read and Grundy, Reference Read and Grundy2011; Grundy and Foverskov, Reference Grundy and Foverskov2016), a higher propensity to report long-standing illness and physical health problems (e.g. Henretta, Reference Henretta2007; Hank, Reference Hank2010; Grundy and Foverskov, Reference Grundy and Foverskov2016), as well as more depressive symptoms (e.g. Mirowsky and Ross, Reference Mirowsky and Ross2002; Henretta et al., Reference Henretta, Grundy, Okell and Wadsworth2008). Some findings indicate, however, that ‘late’ transitions into motherhood might be associated with adverse health outcomes in later life as well (e.g. Mirowsky, Reference Mirowsky2005; Hank, Reference Hank2010). Whether individuals enter parenthood ‘off-time’ – that is, deviating from the ‘normative’ lifecourse – thus appears to have a stronger effect on their subsequent health and wellbeing than the transition as such (see Koropeckyj-Cox et al., Reference Koropeckyj-Cox, Pienta and Brown2007).
This is also reflected in negative associations of being unmarried at the time of the first birth and later-life physical health outcomes (e.g. Henretta, Reference Henretta2007; Hank, Reference Hank2010), as well as in cross-national variation in the extent to which childlessness is associated with lower psychological wellbeing: Huijts et al. (Reference Huijts, Kraaykamp and Subramanian2013) found the disadvantage in psychological wellbeing of childless people to be smaller in countries with tolerant norms towards childlessness. Overall, however, childlessness does not seem to be consistently associated with older adults’ health: in a comprehensive study, Quashie et al. (Reference Quashie, Arpino, Antczak and Mair2021) found a fairly unsystematic pattern of childless older adults’ risk of poor health across various health outcomes and societal contexts.
Finally, whereas Ellwardt et al. (Reference Ellwardt, Hank and Mendes de Leon2021) found that early grandmotherhood increases women’s mortality risk (compared to non-grandmothers), recent studies suggest that the transition to grandparenthood per se does not substantially affect individuals’ life satisfaction or depressive symptoms (Sheppard and Monden, Reference Sheppard and Monden2019; Di Gessa et al., Reference Di Gessa, Bordone and Arpino2020; but see Tanskanen et al., Reference Tanskanen, Danielsbacka, Coall and Jokela2019). Importantly, though, some research indicates a positive association of grandparental status and active grandparenting with, for example, older adults’ subjective wellbeing (Arpino et al., Reference Arpino, Bordone and Balbo2018) and fewer difficulties with activities of daily living (Danielsbacka et al., Reference Danielsbacka, Tanskanen, Coall and Jokela2019).
Intergenerational relationships and generational placement trajectories in Germany
Our study’s focus lies on the structural availability of intergenerational family ties across individual lifecourses (e.g. McIlvane et al., Reference McIlvane, Ajrouch and Antonucci2007; Sauter et al., Reference Sauter, Widmer and Kliegel2023), as reflected in generational placement trajectories (Hünteler, Reference Hünteler2022). The generational placement indicates the vertical position that individuals take within the family system. That is, the presence or absence of preceding (parents) and subsequent (children) generations in the family determines the position of the individual; accordingly, births and deaths lead to shifts in an individual’s generational placement over time. Thus, generational placement trajectories capture the individual’s changing position within the intergenerational family across their lifecourse. When considering biological parents, children and grandchildren, six distinct generational placements are possible, ranging from individuals without any intergenerational kin relations to those being a child, parent and grandparent at the same time.
Hünteler’s (Reference Hünteler2022) analysis of German cohorts born between 1939 and 1953 revealed six typical generational placement trajectories observed from birth to age 60. They differ with regard to (a) the number of simultaneous vertical roles in the family system as well as (b) the timing and ordering of intergenerational role transitions. Table 1 depicts the distribution of the six clusters as well as whether and when individuals in these clusters typically experienced the considered family transitions. The two trajectories with the fewest transitions comprise permanently childless individuals, with a further distinction between clusters of individuals who lost their parents early (6%) and those who lost them later in life (8%). All other trajectories comprise individuals who became parents: the ‘two generations’ cluster (19%) consists of individuals who experienced a trajectory in which the death of both parents occurred prior to the birth of their first child. The two ‘three generations’ clusters, where individuals had children before they lost their own parents and became grandparents around the time their parents died, are further differentiated by a different timing of transitions: for some, the transitions occurred early in the lifecourse (14%), and for others – the quantitatively most prevalent pattern – they occurred later (34%). Finally, the ‘four generations’ cluster (19%) exhibits a similar ordering of transitions, but the timing was such that grandparenthood occurred prior to the death of the second parent (i.e. individuals experienced for some time the family roles of being a child, parent and grandparent simultaneously).
Table 1. Distribution and characteristics of typical generational placement trajectories in German cohorts born 1939–1953 (occurrence and relative timing of transitions)

Notes: Timing refers to the average timing of these transitions in relation to the overall sample. Parentheses indicate that the transition does not occur for all individuals within that cluster until age 60. For more detailed information about the occurrence and timing of transitions, see Hünteler (Reference Hünteler2022) as well as Table S1 in the online supplementary material.
Across cohorts, the prevalence of clusters was shown to be fairly stable. However, a trend towards trajectories with later role transitions – which are thus more ‘stable’ – became evident. Moreover, women, compared to men, and individuals who grew up in the former Eastern parts of Germany were more likely to experience trajectories characterised by early transitions into parenthood and grandparenthood (in the ‘three generations (early)’ and the ‘four generations’ clusters).
Hypotheses
From the theoretical considerations and previous empirical findings described above, we derive the following general hypotheses about how the generational placement trajectories identified by Hünteler (Reference Hünteler2022) might be associated with later-life health and wellbeing:
• Hypothesis 1a: A larger intergenerational kinship reservoir – as observed in the ‘three generations’ and ‘four generations’ clusters – is associated with more favourable outcomes because it provides more opportunities (1) to (re-)activate family ties in order to seek support in times of need and (2) to take on multiple active family roles simultaneously (role enhancement).
• Hypothesis 1b: A larger intergenerational kinship reservoir is associated with less favourable outcomes because (1) it exposes the individual to more potential obligations to support others and (2) forces individuals into multiple active family roles simultaneously (role strain).
• Hypothesis 2: ‘Off-time’ transitions, such as parental loss at younger ages or teenage motherhood, which are characteristic for the ‘childless (early)’ or ‘three generations (early)’ clusters, are associated with less favourable outcomes because they constitute deviations from the ‘normative’ family lifecourse.
Importantly, individuals’ socio-economic status has been shown to impact both the occurrence and timing of family role transitions (e.g. Skopek and Leopold, Reference Skopek and Leopold2017; van Roode et al., Reference van Roode, Sharples, Dickson and Paul2017) as well as health and wellbeing (e.g. Saint Onge and Kueger, Reference Saint Onge, Kueger and Cockerham2021). The expected associations between generational placement trajectories and the later-life outcomes considered in our study might thus be partially affected by their joint association with individuals’ socio-economic characteristics.
• Hypothesis 3: (Bivariate) Associations of generational placement trajectories and later-life health and wellbeing become weaker – or even disappear – if individuals’ socio-economic status is accounted for.
Data and methods
Data
The data for our analysis were derived from two cross-sectional rounds of the German Ageing Survey (DEAS; Klaus et al., Reference Klaus, Engstler, Mahne, Wolff, Simonson, Wurm and Tesch-Römer2017), collected in 2008 and 2014. DEAS is a nationally representative study of non-institutionalised adults aged 40–85, providing rich information on various dimensions of wellbeing as well as demographic data on respondents’ parents, children and – from 2008 onwards – grandchildren. From the initial sample of 12,206 first-time respondents, we excluded (a) 5,381 individuals younger than age 60 to allow considering grandparenthood in our analysis and (b) 1,773 individuals aged 75 or older to avoid potential survivor bias. Thus, only respondents born between 1933 and 1954 were included in the analytic sample. Because respondents provided demographic information only on their two primary care-givers during childhood, those who did not grow up with both of their biological parents (1,102) were excluded, as were observations with item non-response on the birth or death dates of parents (124), children (ten) or grandchildren (100). Respondents were also excluded if the birth of the youngest (grand-)child was reported to have happened prior to the parent’s 12th birthday (11), or if information on any of the four outcome variables (83) or partnership status, education or labour force status (five) was missing. The final analytical sample thus comprises a total of 3,617 observations. Note, however, that two of the dependent variables (see below), namely life satisfaction and physical health problems, were assessed using an additional paper-and-pencil drop-off questionnaire that respondents filled out and returned after the main interview. Analyses including these two variables are thus based on a smaller sample of 2,750 respondents.
Item non-response in the independent variable relative income position (11%) was imputed using multiple chained equations (White et al., Reference White, Royston and Wood2011) which contained the incomplete dependent variables before they were case-wise deleted. Results based on complete case analysis were largely consistent with the analyses based on the imputed data. Finally, weights were applied to the analyses in order to correct for the initial sample’s stratification by age, gender and region, as well as potential selectivity in returning the additional drop-off questionnaire when applicable (see Klaus et al., Reference Klaus, Engstler, Mahne, Wolff, Simonson, Wurm and Tesch-Römer2017).
Dependent variables
We considered four outcome variables, capturing different dimensions of later-life wellbeing and health:
(1) Global life satisfaction, as an indicator of subjective wellbeing, was assessed in DEAS’ drop-off questionnaire and was measured by the average rating of five items, such as ‘In most ways my life is close to my ideal’, using a five-point scale ranging from 1 = strongly agree to 5 = strongly disagree (given at least three of the items had been answered) (Pavot and Diener, Reference Pavot and Diener1993). The scale was recoded so that higher values indicated higher satisfaction with life (Cronbach’s alpha = 0.84).
(2) Depressiveness, as an indicator of psychological distress, was assessed using a German short form of the CES-D scale (Center for Epidemiologic Studies Depression scale). This scale was constructed as the sum of 15 items assessing the frequency of a variety of feelings, thoughts and mental states, such as feeling fearful or sleeping restlessly over the past week, with categories ranging from 0 = rarely or none of the time (less than 1 day) to 3 = most or all of the time (5–7 days). If at least eight items had been answered, the average was calculated and then multiplied by 15. The scale ranged from 0 to 45, with higher scores indicating higher levels of depressiveness (Cronbach’s alpha = 0.85).
(3) Functional limitations, as an indicator of the individual’s inability to perform specific tasks, were measured by respondents’ evaluations using a part of the SF-36 scale (Medical Outcomes Survey 36-item Short Form) on health which included limitations in ten activities of daily living (0 = no, not limited at all to 2 = yes, limited a lot; recoded). Given at least nine of the ten items were answered, the sum of the ratings was calculated so that individuals with no limitations at all scored 0 and those with strong limitations in all activities scored 20 (Cronbach’s alpha = 0.92).
(4) Finally, the number of physical health problems (e.g. respiratory problems, cancer or insomnia) was reported by respondents based on a list provided in the drop-off questionnaire. Ranging from 0 to 12 in our sample, a higher number of problems mentioned reflected worse physical health.
Independent variables
Our main explanatory variable of interest is the respondent’s generational placement trajectory. Applying sequence and cluster analysis using the packages TraMineR (Gabadinho et al., Reference Gabadinho, Ritschard, Müller and Studer2011) and WeightedCluster (Studer, Reference Studer2013) in the program R, we reproduced the six clusters of generational placement trajectories identified by Hünteler (Reference Hünteler2022) as follows: we defined the trajectories according to if and when individuals transitioned into parent and grandparenthood or lost their second parent on an annual basis from birth to age 60. Combining these three transitions, six exclusive states are possible, ranging from having no intergenerational kin alive to being a child, parent and grandparent simultaneously. The big advantage of sequence analysis is that no assumptions about the underlying distribution are necessary, such as in latent class analysis, and that the calculation of the differences between the trajectories can be chosen in accordance with theoretical considerations. Because of its sensitivity to differences in timing, we used the chi-square measure to group the trajectories into clusters of similar trajectories (Studer and Ritschard, Reference Studer and Ritschard2016). As shown in previous research (Hünteler, Reference Hünteler2022) and in contrast to other distance measures, such as optimal matching, the clusters were not only well separated considering the number of simultaneously living intergenerational family members (relevant for Hypotheses 1a and 1b) but also the age at which specific transitions occurred (relevant for Hypothesis 2). Based on the calculated distances, different clusters were identified using the Partitioning Around Medoids algorithm, with the starting point of the algorithm defined through the hierarchical clustering ‘Ward’, as is recommended (Studer, Reference Studer2013). This method strives towards maximising a global criterion and it performed better on several quality measures and different numbers of clusters than the ‘Ward’ algorithm.
In line with Hünteler’s (Reference Hünteler2022) findings, the analyses suggested a six- and an eight-cluster solution. Six clusters already allowed for a substantively clear differentiation between the groups, whereas the eight-cluster solution further separated the two childless (by timing of parental death) and the third cluster (the ‘four generations’ pattern) (also by timing of parental death). Additionally, six clusters performed comparatively better and overall well on the measures of the quality of partition, such as the weighted average silhouette width (0.46) and Hubert’s C (0.05) (Studer, Reference Studer2013). Therefore, the six-cluster solution – which virtually produced the same clusters as described above (Table 1) – was preferred above the eight-cluster solution. For the regression analyses, depending on which cluster respondents belonged to, they were assigned a value of 1 in one of the following binary indicators (0 otherwise): ‘childless (early)’, ‘childless (late)’, ‘two generations’, ‘three generations (early)’, ‘three generations (late)’ (reference category), ‘four generations’. For descriptive statistics of the cluster characteristics, see Table S1 in the online supplementary material.
Finally, we account for a broad set of control variables: next to basic demographic characteristics, namely age (and its square; 66.9 years on average), gender (52% female), partnership status (81% having a partner) and migration background (8%), we pay particular attention to indicators of individuals’ socio-economic status (as proposed in Hypothesis 3): education (based on the International Standard Classification of Education: low (0–2; 11%), medium (3–4; 54%) or high (5–6; 35%)), employment status (working (15%) versus retired (73%) versus not employed (12%)), relative income position (operationalised as percentage points of the mean of the equivalent net income of the German population; 117 on average (missing values were imputed)), social class (up to middle class (48%) versus upper (middle) class (52%), operationalised by respondents’ and their partners’ (last) occupational position). Moreover, we control for respondents’ current region of residence: East Germany (18%) versus West Germany (82%). This seems important because the cohorts in our sample were born prior to unification and despite considerable convergence after unification, both regions still tend to differ with regard to, for example, transitions to parenthood (Hank and Huinink, Reference Hank, Huinink, Hank and Kreyenfeld2015) and grandparenthood (Leopold and Skopek, Reference Leopold and Skopek2015), their prevalence of typical generational placement patterns (Hünteler, Reference Hünteler2022), as well as health (Lampert et al., Reference Lampert, Müters, Kuntz, Dahm and Nowossadeck2019). For descriptive statistics of these variables by clusters of generational placement trajectories, see Table S1 in the online supplementary material.
Analytical approach
We ran two linear regression models for each outcome variable that included the generational placement patterns as the main independent variable. This is a well-established procedure to test for the associations between family trajectories and individual later-life outcomes (Jalovaara and Fasang, Reference Jalovaara and Fasang2020; Comolli et al., Reference Comolli, Bernardi and Voorpostel2021; Kapelle and Vidal, Reference Kapelle and Vidal2022). The first model tested the bivariate relationship between generational placement clusters and the later-life outcomes, whereas the second model additionally included the control variables. The second model thus estimated the association of the generational placement trajectory with the wellbeing indicators independent of socio-demographic differences. To facilitate interpretation, we calculated the overall sample mean of each wellbeing indicator and the deviations from it for each family pattern. This allows for an assessment of cluster differences that is independent from any reference category (like in the original regression models). These deviations from the sample mean were calculated using the Stata-ado mimrgns (Klein, Reference Klein2014). Additionally, we calculated pairwise contrasts for each of the typical patterns in order to investigate differences between specific pairs of clusters more in depth. Replication files are available at https://osf.io/e4ncd/?view_only=30d538687dab484f95e4c78ec03d48d6.
Results
Linear regression models were estimated for each later-life outcome in order to assess their bivariate and multivariate associations with the previously identified six clusters of generational placement trajectories. Table 2 exhibits deviations of the predicted cluster means from the overall sample mean (full regression results are displayed in Table S2 in the online supplementary material).
Table 2. Deviations of predicted cluster means from overall sample mean based on linear regressions
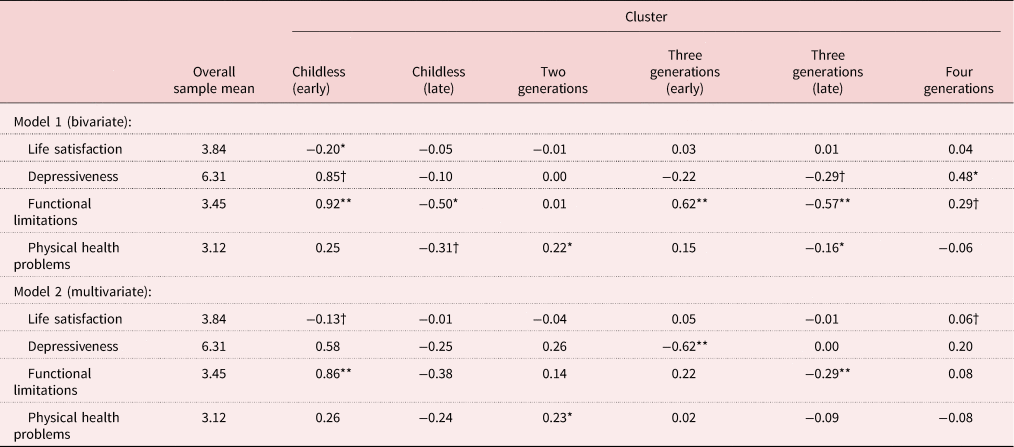
Notes: Weighted data; N = 3,617 for depressiveness and functional limitations; N = 2,750 for life satisfaction and physical health problems; own calculations, based on the German Ageing Survey (DEAS 2008, version 3.2 and DEAS 2014, version 4.0). For the full display of the regression results, see Table S2 in the online supplementary material.
Significance levels: † p < 0.10, * p < 0.05, ** p < 0.01.
Considering the bivariate models (Table 2, Model 1), two clusters stood out: individuals in the ‘childless (early)’ cluster were worst off in three out of the four dimensions of health and wellbeing considered in the analysis. That is, compared to the overall sample mean, they reported significantly lower life satisfaction as well as higher levels of functional limitations and (marginally significant) depressiveness. In contrast, those in the ‘three generations (late)’ cluster scored best, that is, they reported the lowest levels of functional limitations and (marginally significant) depressiveness as well as the fewest physical health problems. Similarly, individuals in the ‘childless (late)’ cluster exhibited lower levels of functional limitations and (marginally significant) depressiveness than the sample mean. Whereas these bivariate findings indicate that the timing of changes in one’s generational placement might indeed matter, and that trajectories vary particularly in regard to their association with functional limitations (which we also observe in the ‘three generations (early)’ and – marginally significant – ‘four generations’ clusters), a consistent overall pattern did not emerge. Being in the ‘two generations’ cluster, for example, was merely associated with being more likely to have a higher number of physical health problems, and individuals in the ‘four generations’ cluster were the only ones clearly exhibiting above-average levels of depressiveness.
The multivariate models (Table 2, Model 2) accounted for differences in clusters’ socio-demographic composition and, importantly, for socio-economic status (see Table S1 in the online supplementary material and Hypothesis 3). Some of the previously significant relationships were no longer statistically significant. All remaining relations suggest that the generational placement patterns are directly associated with later-life wellbeing to some degree. Individuals in the ‘childless (early)’ cluster continued to exhibit worse health and wellbeing outcomes than individuals in other clusters: compared to the overall sample mean, they reported (marginally significant) lower life satisfaction and the highest level of functional limitations (versus all clusters characterised by late parental death; see pairwise comparisons in Table S3 in the online supplementary material). The initially suggested health advantage of individuals in the ‘three generations (late)’ cluster partially disappeared and now merely pertained to a lower level of functional limitations (versus those characterised by early parental loss; Table S3 in the online supplementary material). Individuals’ levels of functional limitations, thus, seem to depend on the combination of (a) the timing of one’s parents’ death and (b) the occurrence and timing of one’s own transition to parenthood: only individuals who experienced parental loss and entry into parenthood ‘late’ enjoyed a health advantage (that is, a below-average level of functional limitations), whereas only those who experienced an ‘early’ parental loss and did not become a parent themselves exhibited a significant health disadvantage.
Life satisfaction turned out to be significantly below average in the ‘childless (early)’ cluster (versus those characterised by early parenthood; Table S3 in the online supplementary material) and above average in the ‘four generations’ cluster (versus ‘childless (early)’ and ‘two generations’; Table S3 in the online supplementary material). That is, individuals in the cluster with the fewest living generations for the longest period of time (due to early loss of the parents and no transition into parenthood) seemed to be least satisfied with life, whereas those with the largest kinship reservoir were most satisfied. These differences in life satisfaction might point to processes of compensation (when one’s new role as a parent replaces the loss of one’s role as a child, especially if both transitions occur early in the lifecourse) and an additive advantage (if the benefits associated with ‘late’ parental death were supplemented by having own children).
Once socio-demographic characteristics and socio-economic status were controlled for, depressiveness was found to be significantly below the sample mean in the ‘three generations (early)’ cluster (versus all but the ‘childless (late)’ cluster; Table S3 in the online supplementary material) – and only here – which was not the case in the bivariate model. The significantly higher number of physical health problems reported by individuals exhibiting a ‘two generations’ generational placement trajectory (versus clusters characterised by ‘late’ parental death; Table S3 in the online supplementary material) was, however, consistently found in models with and without controls. Finally, none of our health and wellbeing measures exhibited a statistically significant association with the ‘childless (late)’ cluster in the multivariate analysis, indicating that socio-demographic and socio-economic characteristics rather than the generational placement trajectory itself were the drivers of the seemingly better health outcomes observed among individuals in this cluster in the bivariate model.
Such compositional effects also seem to explain the overall weak pattern of associations between generational placement trajectories and later-life wellbeing and health: for life satisfaction, gender, partnership status, migration background, class membership and residence in East Germany seemed to be influential, whereas, for depressiveness and functional limitations, age (U-shaped), education and labour force status appeared to matter as well. For physical health problems, only age, education and labour force status were relevant. Relative income was significantly associated with all outcomes, but the size of the estimator was zero.
Discussion
Against the background of ample research indicating a key role of family relationships in individuals’ wellbeing and health across the lifecourse (e.g. Umberson and Thomeer, Reference Umberson and Thomeer2020), the present study set out to provide a more comprehensive exploration of the nexus between the structural availability of intergenerational family ties and wellbeing and health in a nationally representative sample of older Germans aged 60–74. Building primarily on a lifecourse perspective (complemented by family systems and role theorical considerations), we investigated associations between the occurrence, timing and ordering of transitions into or out of multiple intergenerational family positions over time (i.e. ‘generational placement trajectories’; Hünteler, Reference Hünteler2022) and four distinct dimensions of health and wellbeing in later life.
Two main findings emerged from our study. First, our analysis did not reveal a systematic pattern of associations between specific clusters of generational placement trajectories and the various indicators of wellbeing and health considered here. Importantly, several of the initially observed bivariate correlations between individuals’ generational placement trajectories and later-life health and wellbeing disappeared once we controlled for individuals’ socio-economic characteristics. Consistent with Hypothesis 3, these associations, where we observed them at all, were thus not independently driven by specific sets of lifecourse vertical positions in the family system, but rather by their interplay with socio-economic positions typically associated with generational placement trajectories as well as health and wellbeing. Along similar lines, Comolli et al. (Reference Comolli, Bernardi and Voorpostel2021), for example, found work and family (i.e. partnership and childbearing) trajectories to be jointly associated with (subjective, relational and financial) wellbeing at older ages (see also Tosi and Grundy, Reference Tosi and Grundy2021).
Second, some statistically significant associations remained even in our fully controlled models. Whereas these correlations are difficult to interpret – statistically as well as theoretically – in terms of their underlying causal mechanisms, they still provide two important insights: to begin with, the structural availability of intergenerational family ties and the number of simultaneous intergenerational family roles seems to matter. Those with two or fewer ties (i.e. a small kinship reservoir) are more likely than the average to suffer from higher levels of functional limitations (‘childless (early)’) or more physical health problems (‘two generations’), whereas those in the ‘three generations’ clusters, for example, report lower levels of depressiveness (‘early’) or functional limitations (‘late’). Rather than supporting Hypothesis 1b, this result supports Hypothesis 1a and the notion of salutary effects of a larger demographic reserve (‘kinship reservoir’) and multiple social roles (‘role enhancement’) in the family (see e.g. McIlvane et al., Reference McIlvane, Ajrouch and Antonucci2007). While role strain might play a role for some individuals, role enhancement might outweigh potential negative consequences, on average.
At the same time, and in line with Hypothesis 2, the timing of intergenerational family role transitions appears to be relevant as well. Those in the ‘early’ and ‘late’ three generations clusters seem to enjoy different ‘health benefits’, and those in the ‘early’ childless cluster tend to experience health disadvantages, whereas their ‘late’ counterparts do not. This finding points to the key tenet of lifecourse theory that it matters whether a transition occurs ‘on-time’ or ‘off-time’. Negative life events occurring ‘off-time’, such as an early parental death, have been proposed to exhibit particularly strong negative effects on individuals’ wellbeing, for example (Leopold and Lechner, Reference Leopold and Lechner2015). Importantly, the effect of such deviations from the ‘normative’ family lifecourse need not be a direct one, but it might also be mediated through effects on the individual’s educational attainment or socio-economic status (e.g. Patterson et al., Reference Patterson, Verdery and Daw2020b).
Overall, our analysis has demonstrated that individuals’ later-life wellbeing seems to depend, in part, on the interplay between the occurrence, timing and ordering of transitions into and out of multiple vertical family roles, underlining the importance of the two lifecourse principles of ‘timing’ and ‘linked lives’. Our findings highlight the complexity of their interaction, considering their direct and indirect relationships with health and wellbeing. Still, the present study is not without limitations. First, we exclusively focused on intergenerational relationships with biological parents, children and grandchildren. Obviously, though, meaningful social roles in families may also result from step-relations (e.g. Ganong and Coleman, Reference Ganong and Coleman2017) as well as intragenerational relationships with siblings (Hank and Steinbach, Reference Hank and Steinbach2018), for example, and might thus also be relevant for later-life health and wellbeing. Second, whereas DEAS provides detailed information on respondents’ family biographies (allowing us to assess individuals’ lifecourse generational placement trajectories), comprehensive measures of respondents’ health and socio-economic status are not available retrospectively and the analyses were restricted to individuals who grew up with both of their biological parents. Moreover, DEAS’ potential for longitudinal analyses is very limited (the longitudinal sample is rather small, both in terms of the number of follow-up interviews after 2014 and the number of panel participants). We are thus neither able to identify health trajectories, nor can we properly assess the issue of reversed causality (i.e. health limitations earlier in life might affect individuals’ generational placement trajectories, whose causal effect on later-life wellbeing we would ideally like to identify). The same applies to individuals’ lifecourse socio-economic position, which is – to some extent – endogenous to both family (e.g. Aisenbrey and Fasang, Reference Aisenbrey and Fasang2017) and health (e.g. Niedzwiedz et al., Reference Niedzwiedz, Katikireddi, Pell and Mitchell2012) trajectories.
Despite these limitations, our study contributes in several ways to advancing research investigating the role of family ties in individuals’ (later-life) health and wellbeing: by taking a more comprehensive perspective which, conceptually, integrates lifecourse, family systems and role theories and, empirically, considers transitions into and out of multiple kin relations over time, as reflected in individuals’ generational placement trajectories, the current analysis demonstrates that even in the absence of one coherent pattern the number and timing of intergenerational family role transitions bear statistically significant associations with a variety of health outcomes at older ages. Further investigation of these relationships, particularly explorations of the causal mechanisms underlying them, appear to be important and promising tasks for future research.
The immediate practical implications of our study seem somewhat more limited. However, our findings indicate that older adults with a smaller intergenerational relational reserve and fewer family roles across their lifecourse might experience disadvantages in health and wellbeing (partially affected by socio-economic inequalities). This contributes to recent debates about the consequences of ‘kinlessness’ in later life for individuals’ health (e.g. Margolis et al., Reference Margolis, Chai, Verdery and Newmyer2022), the alternatives to ‘ageing alone’ in the absence of close kin (e.g. Mair, Reference Mair2019) and, relatedly, if and how interventions aiming to support adults ‘ageing solo’ can actually compensate lacking family ties (e.g. Lowers et al., Reference Lowers, Zhao, Bollens-Lund, Kavalieratos and Ornstein2023).
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0144686X2300034X.
Acknowledgements
We thank Heribert Engstler from the DZA for generating and providing the necessary demographic data on children and grandchildren, and Daniel Klein for his advice on handling multiple imputation data. Our thanks also go to Martin Wetzel and Thomas Leopold for their thoughts on earlier versions.
Financial support
This work was supported by the Cologne Graduate School in Management, Economics and Social Sciences of the University of Cologne (BH).
Competing interests
The authors declare no competing interests.
Ethical standards
Ethical approval was not required.





 Open access
Open access