

The first reported case of developmental dyslexia appeared in the British Medical Journal in 1896. Dr Pringle Morgan, a general practitioner, described a 14-year-old boy named Percy, who, despite being ‘bright and of average intelligence in conversation’, had been unable to learn to read. Specimens of Percy's writing show many spelling errors characteristic of dyslexia (such as ‘carlfuly’ for ‘carefully’, ‘pag’ for ‘peg’ and ‘Precy’ for ‘Percy’). Morgan pointed out that Percy could read numbers but had difficulties with written words. For example, he could discern the numeral 7 but not the word seven (Reference MorganMorgan 1896). Reference HinshelwoodHinshelwood (1907) later called the condition ‘congenital word blindness’
The word dyslexia comes from the Greek dys-, broadly denoting difficultly or inadequacy, and lexis, meaning word. A number of terms have been used to describe dyslexia. In the psychiatric classifications ICD–10 (World Health Organization 1992) and DSM–IV (American Psychiatric Association 1994) it is called ‘reading disorder’. In ICD–10, this is classified under ‘Specific developmental disorders of scholastic skills’; in DSM–IV, it comes under ‘Learning disorders’. In the UK, the word dyslexia has not been popular in educational services (where it is most commonly encountered), and the term ‘specific learning difficulties’ is used in preference. Psychologists, who have carried out most research in this area, also tend to use the latter term. Other descriptions include ‘specific reading disability’, ‘reading disability’ and ‘reading retardation’. I use the word dyslexia as it has become etched in the minds of the public and professionals and provides a familiar shorthand for describing the condition.
Over the past 40 years there has been a vast amount of research into reading acquisition and reading difficulties. In fact, dyslexia has been one of the most intensely studied subjects in developmental psychology. As a result, a massive amount of literature has accumulated that has helped us better understand the nature of the core deficits seen in dyslexia, their aetiology and clinical features.
Relevance for child and adolescent psychiatry
Given that dyslexia is primarily a scholastic problem and the responsibility for any intervention lies with educational services, what is the role of the child psychiatrist? First, dyslexia is common: it is the most common of all specific developmental disorders, accounting for almost three-quarters of all specific learning difficulties (Reference Shaywitz and ShaywitzShaywitz 2003a). Its estimated minimum prevalence is around 5%. This is considerably higher than the best estimates of prevalence of autism-spectrum disorders, which is in the region of 1% (Reference Baird, Simonoff and PicklesBaird 2006; Reference Baron-Cohen, Scott and AllisonBaron-Cohen 2009). Second, comorbidity with child mental health problems is considerable (as high as 50% or more, as discussed below). Hence, dyslexia is bound to be overrepresented in child mental health clinical populations and the consequences of the disorder to the child have to be factored into any case formulation and management plan. If one takes the view that the purpose of any psychiatric intervention with children and adolescents is not symptom removal alone, but facilitating navigation through their normal developmental tasks, it becomes important to consider the impact dyslexia may have on the child.
Defining dyslexia
There are a number of definitions of dyslexia. ICD–10 and DSM–IV adopt a broadly similar approach. In describing specific reading disorder, ICD–10 says that ‘The main feature … is a specific and significant impairment in the development of reading skills, which is not solely accounted for by mental age, visual acuity problems, or inadequate schooling’ (World Health Organization 1992: p. 245). The ICD–10 Diagnostic Criteria for Research (DCR–10) for specific reading disorder (which provide a more succinct definition) are shown in Box 1. The diagnostic criteria for reading disorder in DSM–IV essentially require both that reading ability assessed using standardised tests of accuracy or comprehension is substantially below that expected given the person's age, IQ and age-appropriate education, and that this significantly interferes with academic achievement or activities that require reading normal developmental tasks (American Psychiatric Association 1994). In the ICD–10 multiaxial classification (World Health Organization 1996) it is placed under Axis II (specific disorders of psychological development), whereas in DSM–IV it is classified under Axis I (clinical disorders).
BOX 1 ICD–10 Diagnostic Criteria for Research (DCR–10) for specific reading disorder (F81.0)
-
A. Either of the following must be present:
-
(1) a score on reading accuracy and/or comprehension that is at least 2 standard errors of prediction below the level expected on the basis of the child's chronological age and general intelligence, with both reading skills and IQ assessed on an individually administered test standardized for the child's culture and educational system;
-
(2) a history of serious reading difficulties, or test scores that met criterion A(1) at an earlier age, plus a score on a spelling test that is at least 2 standard errors of prediction below the level expected on the basis of the child's chronological age and IQ.
-
-
B. The disturbance described in criterion A significantly interferes with academic achievement or with activities of daily living that require reading skills.
-
C. The disorder is not the direct result of a defect in visual or hearing acuity, or of a neurological disorder.
-
D. School experiences within the average expectable range (i.e. there have been no extreme inadequacies in educational experiences).
-
E. Most commonly used exclusion clause. IQ is below 70 on an individually administered standardized test.
(World Health Organization 1993: p. 144. Reproduced with permission)
The discrepancy definition
Both ICD–10 and DSM–IV provide a ‘discrepancy definition’ of dyslexia. According to the discrepancy criterion, individuals are classified as having dyslexia if their reading skills are significantly below what would be expected from their IQ scores. This is a purely psychometric definition that does not take into account the putative underlying cognitive processes. Research in the area has produced a number of compelling reasons for questioning the discrepancy definition. These objections may be summarised as follows (Reference Vellutino, Scanlon and LyonVellutino 2000):
-
• psychological research shows that the correlation between IQ and reading skills is low
-
• the core cognitive variables relevant to reading (discussed below in ‘The cognitive basis of dyslexia’) are the same between poor readers of high and low IQ
-
• intervention studies show that IQ makes no difference to response to remediation
-
• there is no reason to believe that children with low IQ cannot have dyslexia.
There is now abundant evidence for redefining all specific developmental disorders in ways that are consistent with how intellectual disability (known as ‘learning disability’ in UK mental health services and as ‘mental retardation’ in DSM–IV) is defined, i.e. on the basis of the child's ability in the particular domain relative to age peers (Reference Dyck, Hay and AndersonDyck 2004). Note that the ICD–10/DCR–10 and DSM–IV definitions make no distinction between reading accuracy and reading comprehension. It has now been shown that dyslexia (in which reading accuracy is the main problem) is distinct from reading comprehension disorder (Reference Hulme and SnowlingHulme 2009: pp. 90–128).
An alternative definition
Accumulating research in the field has led to an emerging consensus regarding a universally acceptable definition of dyslexia. The following definition, formally adopted by the International Dyslexia Association, draws on the most recent results:
Dyslexia is a specific learning disability that is neurobiological in origin. It is characterised by difficulties with accurate and/or fluent word recognition and by poor spelling and decoding abilities. These difficulties typically result from a deficit in the phonological component of language that is often unexpected in relation to other cognitive abilities and the provision of effective classroom instruction. Secondary consequences may include problems in reading comprehension and reduced reading experience that can impede growth of vocabulary and background knowledge (Reference Lyon, Shaywitz and ShaywitzLyon 2003: p 2).
This definition, summarised in Box 2, succinctly captures the most important aspects of dyslexia as it is currently understood. It is worth noting that the definition does not say how severe the reading difficulties should be for a diagnosis of dyslexia to be made. The lack of universally accepted criteria to fix a threshold has been a common source of disparities in prevalence and outcome studies.
BOX 2 A recent, research-based definition of developmental dyslexia
-
• It is a specific learning disability
-
• It is characterised by poor word reading, spelling and reading fluency
-
• These difficulties result from specific cognitive deficits in the phonological component of language
-
• These difficulties are ‘unexpected’ in the context of individual's other cognitive abilities
-
• The difficulties occur despite adequate classroom instruction
The cognitive basis of dyslexia
In dyslexia, the essential difficulties in reading occur at word level. The central problem involves recognition of words in isolation and this leads to poor accuracy of reading and spelling and to impaired reading fluency. Higher-level language skills in syntax (grammar), semantics (meaning) and pragmatics (social use of language) are unimpaired.
One of the robust findings of research into developmental psychology over the past 40 years is that poor word reading abilities arise from a specific defect in phonological (speech) processing. This processing deficit encompasses at least two elements: deficits in phonological skills and impairment in acquisition of print-to-sound decoding skills. These phonological deficits have been shown to be present before children learn to read (Reference Gallagher, Frith and SnowlingGallagher 2000) and may be assessed by tests of readiness to read (e.g. rhyming, naming).
Deficits in phonological skills
Acquisition of reading is thought to involve two steps (Reference ShaywitzShaywitz 2003b: pp 45–58). First, the child has to develop the ability to break down the spoken word into its sound units or phonemes. For example, the child has to learn that the word ‘cat’ should be fragmented into the phonemes /k/-/a/-/t/, and the word ‘ship’ into the phonemes /sh/-/i/-/p/. Difficulty in segmenting spoken words into phonemes is the hallmark of dyslexia. Consequently, children with dyslexia show poor phonemic awareness. Phonemic awareness is the ability to notice, think about and manipulate the phonemes in spoken words, and it is usually assessed through rhyming and phoneme manipulation tasks (as discussed below).
Impaired decoding skills
The second step in learning to read involves understanding how printed letters (graphemes) map onto sound units of language (phonemes). Breaking the code of sound–letter association, i.e, learning the grapheme-to-phoneme conversion rules, is a prerequisite for accurate word identification. For example, knowing that the written word ‘cat’ has the same number and sequence of sounds as the spoken word /k/-/a/-/t/ is an indication that the child has understood that the letters represent these sounds. Children with dyslexia show a marked impairment in decoding skills. Decoding skills may be assessed by non-word reading tests (discussed in Reference ThambirajahThambirajah 2010).
The association of letters with phonemes is known as the alphabetic principle or phonics. Mastering the alphabetic principle is considered to be part of reading acquisition. But the task for the child learning to read English is not an easy one. English has a non-phonemic spelling system. That is, the relationship between letters and sounds is not straightforward, i.e. there is no one-to-one correspondence between letters and phonemes. For example, the letter i represents one sound in in ‘pin’ and another sound in ‘pint’. There are about 44 phonemes in the English language (depending on regional accent) but these can be spelled in more than 1000 ways. Italian, Spanish, Greek and most Indian languages have a very close letter-to-phoneme correspondence and are described as having transparent orthographies or spelling systems.
Theories of dyslexia
The core phonological deficit theory
Given the available research, most researchers consider phonological deficits as the core neuro-psychological deficit of dyslexia. This theory posits that poor phonemic awareness and poor mastery of the alphabetic principle are the key underlying deficits seen in most individuals with dyslexia. These cognitive deficits are considered to be both necessary and sufficient conditions for the reading difficulties seen in developmental dyslexia (Reference SnowlingSnowling 2000; Reference Vellutino, Fletcher and SnowlingVellutino 2004). Most individuals with dyslexia also show impairments outside the phonological domain, the two most common being poor verbal working memory (visual short-term memory is unimpaired) and impaired verbal processing speed (rapid automatic naming or RAN) as shown by poor performance in rapid naming tasks. Others show poor sequencing (e.g. difficulties in telling the days of the week in order). Dyslexia is a heterogeneous condition and the cognitive developmental profile of children with dyslexia shows considerable variation depending on the severity of the condition and associated deficits. Box 3 summarises the main cognitive deficits seen in dyslexia.
BOX 3 Core cognitive deficits in dyslexia
-
• The primary skill deficit in dyslexia is difficulty at the level of single-word reading
-
• The word reading problems arise from core cognitive deficits in phonological processing that consist of:
poor phonological awareness (sensitivity to or explicit awareness of the phonological structure of words in one's language), and
difficulties in mastering the alphabetic principle, i.e. connecting written letters (graphemes) with speech sounds (phonemes)
-
• Other prominent impairments seen in most, if not all, people with dyslexia are poor phonological working memory and impaired rapid automatic naming (RAN)
-
• Higher linguistic skills such as syntactic and semantic processing skills are largely intact
Alternative theories
The best known of the several alternative theories of dyslexia are the various visual processing theories and the cerebellar theory and the magnocelluar theory. The first were popular two decades ago but have now largely been discredited and the evidence for the last two is limited. For a review of current theories of dyslexia see Reference Ramus, Rosen and DakinRamus et al (2003).
Aetiology
There is clear evidence that both environmental and genetic factors contribute to reading ability and disability. Moreover, genetic and environmental factors interact in several ways to produce various degrees of reading skill.
The environment
Evidence for an environmental contribution to dyslexia comes from several sources. Cross-linguistic studies (Reference Landerl, Wimmer and FrithLanderl 1997) show that the prevalence of dyslexia depends on the writing system adopted by the community. Its manifestations are less common in populations that use languages which have direct and transparent correspondence between graphemes and phonemes (for example, Italian and Spanish) (Reference Ziegler and GoswamiZiegler 2005).
Socioeconomic status has a considerable influence on reading development. Many studies document the high prevalence of dyslexia in children of low socioeconomic status. As early as 1975, Berger and colleagues, in their Isle of Wight study, reported a 3.1% prevalence of discrepancy-defined reading disability among 10-year-olds living on the Isle of Wight but a 6.3% prevalence among those living in an inner London borough (Reference Berger, Yule and RutterBerger 1975). Subsequent studies have confirmed this relationship between poor reading in dyslexia and low socioeconomic class. A number of environmental factors, including the mother's educational level, time spent reading at home (‘lap-time’ reading) and the availability of reading material at home, have been considered important for development of reading (Reference Raz and BryantRaz 1990). However, no specific environmental factors have been identified.
Summarising across studies, it has been estimated that two-thirds of individual differences in reading are attributable to genetic factors and about one-fifth to shared environmental factors (Reference Pennington and OlsonPennington 2005: pp. 453–472). But, as pointed out by Reference RutterRutter (2005), genes may also act through environmental factors. The period between 4 and 7 years of age appears to be crucial for development of reading and probably represents a sensitive period for acquisition of reading skills (Reference PinkerPinker, 1994).
Biological factors
Developmental dyslexia is both familial and hereditary. Dyslexia runs in families and dyslexia in a parent is one of the strongest predictors of dyslexia in the child. Across studies, about 40% of parents who have offspring with dyslexia have dyslexia themselves. The association is greater for fathers than for mothers, with aggregated figures of 46% and 33% respectively (Reference GrigorenkoGrigorenko 2001).
Twin studies
A number of carefully conducted twin studies show that concordance rates for dyslexia in monozygotic twins are usually more than 70%, whereas in dizygotic twins the rates are below 50%. The most reliable estimate of concordance is probably provided by the Colorado Twin Project, which examined 636 twin pairs of whom at least one had dyslexia. This study found that the concordance rate for pairs of monozygotic twins was around 70%, whereas the corresponding concordance rate for reading disability in same-sex dizygotic twins was 48%, a highly significant difference (Reference DeFries, Fulker and LaBudaDeFries 1987).
In the Twins Early Development Study (TEDS) in the UK, nearly 4000 pairs of 7-year-old twins were studied for word reading ability and decoding skills (Reference Harlaar, Spinath and DaleHarlaar 2005). The main findings of the study were that:
-
• genetic influences accounted for two-thirds (72%) of the individual difference on measures of word reading and decoding
-
• heritability was greater for boys
-
• the genetic contribution was the same for severe and less severe reading difficulties.
Across studies, heritability estimates around 0.6 have been a robust finding for reading disability (and ability). Another interesting finding from twin studies is that heritability of dyslexia is substantially higher for those with a high IQ than for those with a low IQ (Reference Friend, DeFries and WadsworthFriend 2007).
Chromosomes
Genetic studies have proposed several genes as susceptibility candidates at some of the quantitative trait loci linked to dyslexia. Up to now, linkage analysis has identified nine chromosome regions (Reference Schumacher, Hoffmann and SchmälSchumacher 2007). Of these, the loci found on chromosomes 1, 2, 3, 6, 11, 15 and 18 have received the most support, with the loci on chromosome 6 being the most replicated. Altogether, four candidate genes have been identified: DCD2, KIAA0319 (both on chromosome 6p), DYX1C1 (on chromosome 15) and ROBO1 (on chromosome 3). It should be noted that these are not ‘dyslexia genes’, but genes whose variation influences reading. KIAA0319 has been shown to be necessary for neuronal migration during the development of the neocortex (Reference Paracchini, Thomas and CastroParacchini 2006). For a useful summary of the genetics of dyslexia see Reference Demonet and TaylorDemonet & Taylor (2004).
A significant finding from genetic studies of dyslexia is that both normal variations and extremes of reading ability are substantially heritable. That is, the genes that account for dyslexia are the same genes that are responsible for normal variation in reading abilities. The genetic influence on dyslexia is best conceptualised in terms of multiple quantitative trait loci (QTL) that modify the distribution of reading abilities in the population at large and create a continuum of genetic risk for reading difficulties (Reference Plomin and KovasPlomin 2005). Further support for this assertion comes from a genetic study that reports that 15% of the general population carries the candidate gene KIAA0319 (Reference Paracchini, Steer and BuckinghamParacchini 2008).
Brain studies
Post-mortem studies have reported two significant structural changes in the brains of individuals who had dyslexia (Reference GalaburdaGalaburda 1992). A region of the superior temporal gyrus known as the planum temporale has been shown to lack asymmetry in such individuals. In individuals with no history of dyslexia it is normally larger in the left hemisphere than in the right. In those with dyslexia the volumes of the planum temporale are the same on both sides. Since this region of the brain is implicated in auditory and language processing, this finding is thought to be significant. The second finding concerns histological changes in the left-hemisphere perisylvian region and parts of the thalamus in individuals with dyslexia, specifically the presence of abnormally large cells, ectopias (‘brain warts’) and dysplasia. These cellular abnormalities in the brain are thought to result from failure of neural migration.
Functional brain imaging
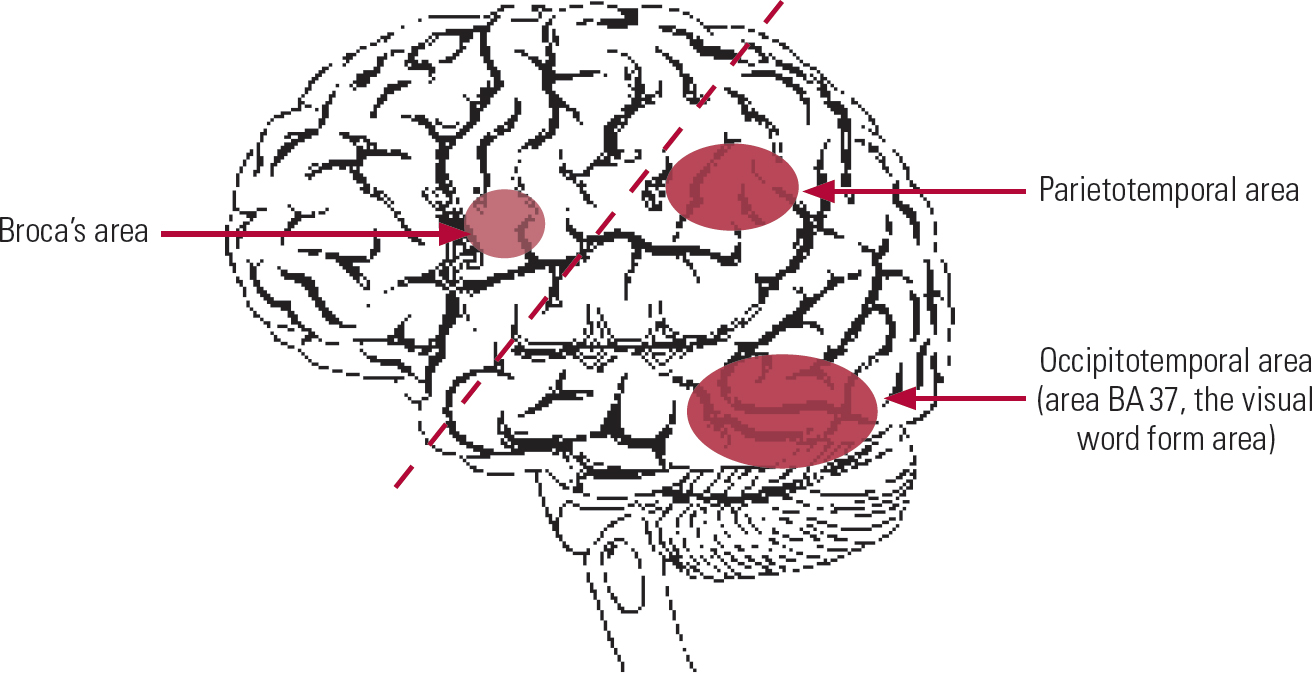
Before considering the findings from functional brain imaging in dyslexia, it is worth reminding ourselves of the various brain areas and neural networks involved in language and reading. The left hemisphere is thought to dominate all language functions, including reading. Three main areas of the left hemisphere are important (Fig. 1).
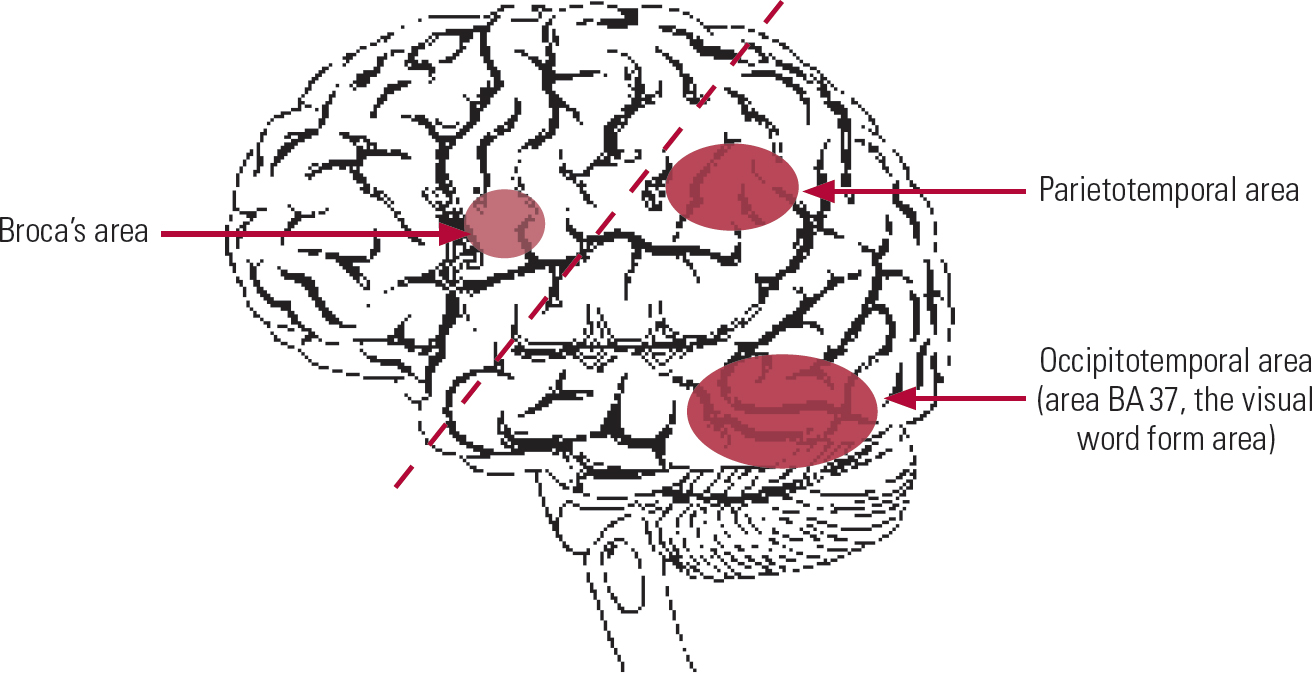
FIG 1 Activation of left-hemispheric brain circuits during phonological tasks in typically developing children. In normal readers the posterior language areas show most activation and there is minimal activity in the anterior language area. The broken line roughly demarcates the anterior and posterior language areas.
The first is an anterior area, including Broca's area located in the left inferior frontal gyrus, responsible for production of speech. This anterior reading system is assumed to be related to phonemic word analysis and articulation during reading and naming.
The second and third are posterior areas:
-
• a parietotemporal area that encompasses Wernicke's area and surrounding areas (the superior temporal gyrus and the angular gyrus); these areas are considered to be responsible for phonological processing and in mapping letters to sounds (decoding);
-
• an occipitotemporal area corresponding to Brodmann's area 37 (BA 37), which provides access to the mental dictionary of words; this area is thought to be crucial for word recognition and has been termed the visual word form area (VWFA).
Several research groups have studied brain functioning in normal and dyslexic readers using technologies such as positron emission tomography (PET), functional magnetic resonance imaging (fMRI) and magnetoencephalography (MEG) (Reference GrigorenkoGrigorenko 2001). Typically, these studies have involved brain imaging to identify activation (or lack of activation) of brain areas during phonological processing tasks that are known to be impaired in dyslexia. Patterns of activation of cerebral areas can be studied during various reading tasks that place increasing demands on phonological analysis (e.g. from simple rhyming tasks to non-word reading).
We now have the benefit of findings from brain imaging studies of children with dyslexia from a number of centres. In general these have produced consistent results (for a review see Reference Shaywitz and ShaywitzShaywitz 2005). The main conclusions from these studies, illustrated in Fig. 2, may be summarised as follows:
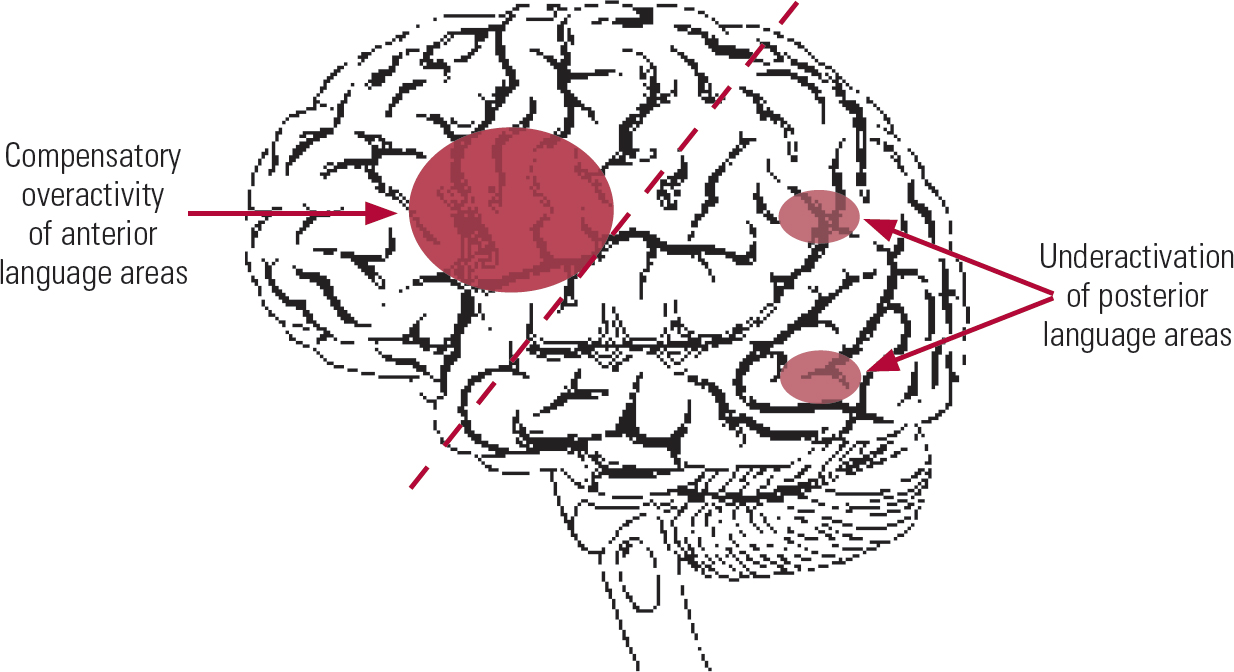
FIG 2 Left hemisphere brain activation pattern in dyslexia showing underactivation of posterior reading circuits during performance of phonological tasks together with compensatory overactivation in anterior language areas (based on results from Reference Shaywitz and ShaywitzShaywitz 2005). The broken line roughly demarcates the anterior and posterior language areas.
-
• during phonological tasks readers with dyslexia exhibit underactivation of the left posterior language areas, especially the occipitotemporal region, and pronounced bilateral activation of the anterior areas;
-
• during tests of phonological awareness children with dyslexia show activation in the language areas in the right hemisphere rather than the left, indicating differences in brain lateralisation;
-
• in children with dyslexia there is poor activation of the cerebellum and other non-specific areas, the significance of which is unclear.
Importantly, evidence-based remedial teaching leads to considerable normalisation in brain activation patterns, especially in the occipito-temporal region.
Categorical v. dimensional view of dyslexia
Given the research findings outlined above, how is developmental dyslexia best conceptualised and understood? In the Isle of Wight study, Reference Rutter and YuleRutter & Yule (1975) had concluded that reading disability represents a ‘hump’ at the lower end of the distribution of reading abilities. Recent epidemiological and genetic research have demonstrated that this is not the case. To date, the evidence is that the difference between dyslexia and normal reading is quantitative and not qualitative. Even severe dyslexia constitutes no more than the extreme of reading distribution. Unlike the case of general intellectual disability, there is no ‘hump’ at the bottom of the normal distribution curve of reading ability, nor is there a bimodal distribution. It is now clear that a categorical approach to the understanding of dyslexia can no longer be justified. Rather, a dimensional approach, where dyslexia is seen as the ‘lower tail’ in the normal distribution of reading abilities in the general population, appears to be more valid (Fig. 3).
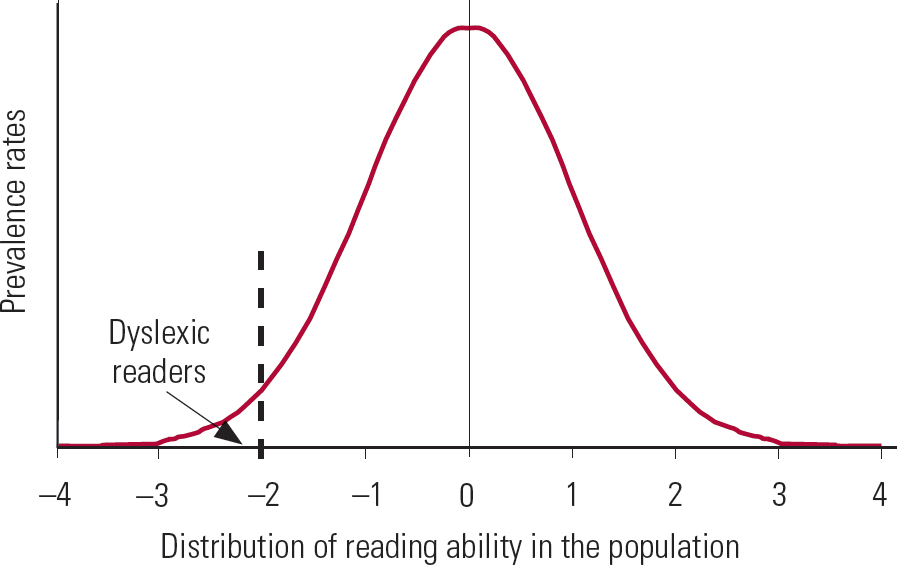
FIG 3 Developmental dyslexia represents the lower tail of the normal variation in reading ability seen in the population. A cut-off score of − 1.5 to − 2 s.d. is usually used. Note that, unlike in general intellectual ability, there is no ‘hump’ at the lower end of the curve.
In one of the best known longitudinal studies in dyslexia, the Connecticut Longitudinal Study, 445 children were followed up from kindergarten to grade 6 (11 years of age). The authors clearly demonstrated that dyslexia is not an all-or-nothing phenomenon, concluding that ‘Epidemiological data indicate that like hypertension and obesity, dyslexia occurs in gradations and fits the dimensional model. Within populations, reading ability and reading disability occur along a continuum, with reading disability representing the lower tail of normal distribution of reading ability’ (Reference Shaywitz, Escobar and ShaywitzShaywitz 1992). Thus, dyslexia is best understood and conceptualised not as a discrete diagnostic category that is distinctly separate from the normal population distribution, but as an extreme variation of reading abilities in the population. Of course, this does not diminish the seriousness of the reading difficulties seen in dyslexia, nor does it exclude the possibility that the lower extreme of the distribution may be aetiologically distinct.
Current research strongly supports an interactional model of dyslexia in which genetic risk factors interact reciprocally with environmental risk factors (G · E) to produce a spectrum of reading disorder of various degrees of severity. The main finding from recent studies suggests that reading difficulties (especially poor phonological skills) interact with other cognitive skills and environmental factors to produce a continuously increasing risk of dyslexia. When the level of risk reaches a certain threshold, the classic dyslexia picture emerges, but the evidence suggests that there are varying degrees of subclinical impairment, particularly in ‘dyslexic families’ (Reference Vellutino, Fletcher and SnowlingVellutino 2004). Longitudinal studies of children of parents with dyslexia show that even the ‘reading-unimpaired’ children exhibit subtle impairments in reading fluency and word knowledge but do not reach the threshold for ‘diagnosis’ of dyslexia. This supports the ‘broader phenotype’ concept of dyslexia and militates against diagnosis of dyslexia as a categorical disorder (Reference SnowlingSnowling 2008). Moreover, dyslexia is primarily a language-based disorder and, as would be expected, it falls on a continuum with specific language impairment. The term dyslexia-spectrum disorders, which include dyslexia and specific language impairment, has been suggested (Reference Bishop and SnowlingBishop 2004).
Key findings from the past 40 years of research are summarised in Box 4.
BOX 4 Key research findings in developmental dyslexia
-
• The discrepancy definition based on comparison with IQ can no longer be justified: dyslexia occurs across the range of intellectual abilities
-
• Dyslexia represents the lower tail of the normal distribution of reading abilities; there is no additional ‘hump’ at the lower tail of distribution
-
• There is a strong genetic contribution to both reading ability and reading disability (dyslexia); environmental factors are as important
-
• Brain imaging studies have demonstrated impaired functioning in the left posterior reading systems (occipitotemporal and parietotemporal areas)
Epidemiology
Estimations of the prevalence of dyslexia vary according to the definition used and the age and language of the population. Although there is now agreement on the ‘lower tail’ hypothesis of dyslexia, the field continues to be bedevilled by the lack of a universally agreed cut-off point for its diagnosis. A number of well-conducted epidemiological studies report the prevalence of dyslexia to vary between 4% and 12%. A major UK epidemiological study of over 1000 children aged 9 to 10 years found 6.2% to have specific reading difficulties. This study used a standard score of 85 (− 1 s.d.; mean = 100) as the cut-off to define dyslexia (Reference Lewis, Hitch and WalkerLewis 1994). Other researchers have used a more pragmatic threshold and adopted a standard score of 80 (− 1.3 s.d.) as the cut-off, which identifies 9% of the population (Reference PenningtonPennington 2009: p 47). Summarising across studies, estimation of the prevalence of dyslexia produces a rate of about 3–6%. Using a conservative estimate of 5% prevalence, a class of 30 children will have at least one or two children with dyslexia. This works out to about 100 children with dyslexia in a secondary school with 2000 pupils.
Dyslexia shows marked male preponderance. An analysis of results from four epidemiological studies showed a male:female ratio in the region of 1.5–2 to 1 (Reference Rutter, Capsi and FergussonRutter, 2004). However, in referred populations boys tend to outnumber girls in a ratio of about 3:1, probably because of the high incidence of conduct problems in males (Reference Shaywitz, Shaywitz and FletcherShaywitz 1990).
Dyslexia has been shown to occur in all linguistic systems. However, its prevalence is said to be significantly lower in linguistic populations in which the written language is more phonetically consistent, such as Spanish, Italian, Greek and Czech (Reference Paulesu, Demonet and FazioPaulesu 2001). In these groups it manifests mainly as poor reading fluency. Detailed study of these children show that the core phonological deficits such as phoneme manipulation are as impaired as in their English counterparts (Reference Caravolas, Snowling and HulmeCaravolas 2005). In logographic languages such as Chinese (where a character represents a word or meaningful part of a word) the difficulties manifest as poor rapid naming.
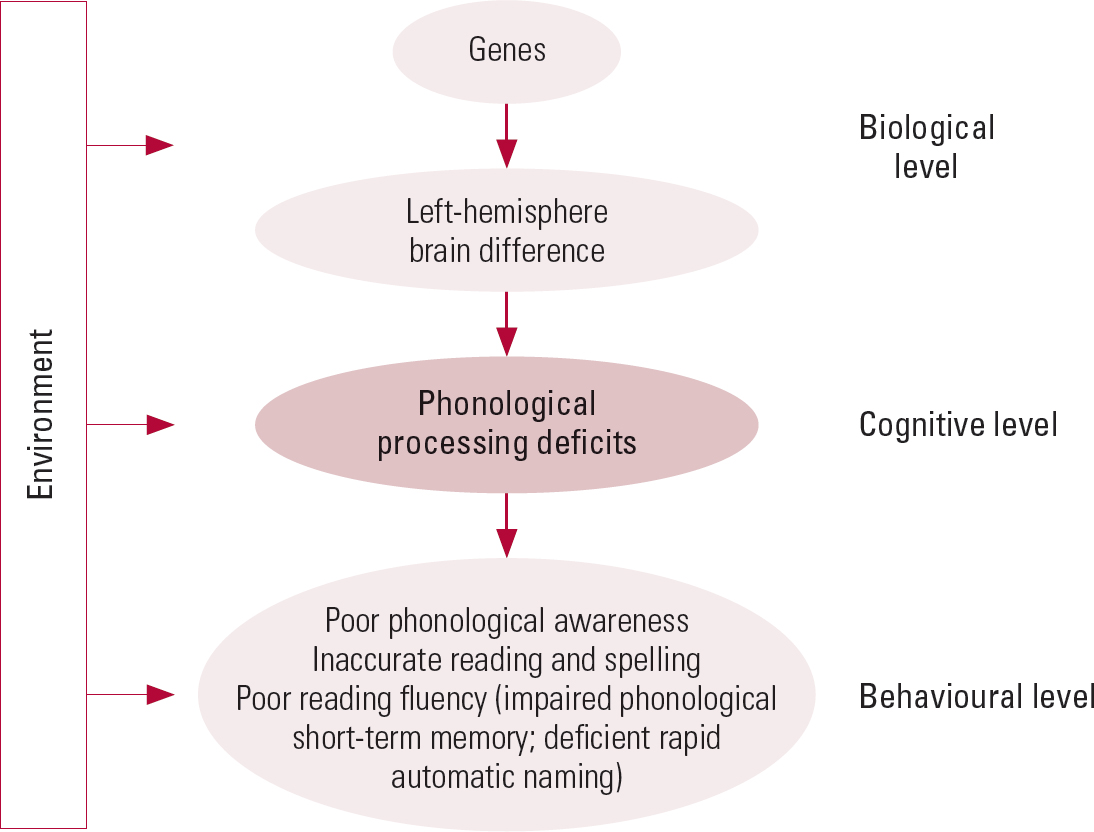
A causal model of dyslexia
A causal model of dyslexia that integrates various theories within a common framework has been put forward by Reference MortonMorton (2004: p 169). The framework indicates three levels of an individual's functioning – biological, cognitive and behavioural – together with a consideration of relevant environmental factors. The behavioural level deals with the manifestations or symptoms of dyslexia, the cognitive level is concerned with the processes underlying the observed deficits in processing, and the biological level seeks to identify the processes within the brain. This allows consideration of underlying genetic mechanisms that lead to the abnormalities in cerebral structure and functioning. Note that environment contributes to the development of reading disability at each level. A simplified diagram of this causal model is shown in Fig. 4.
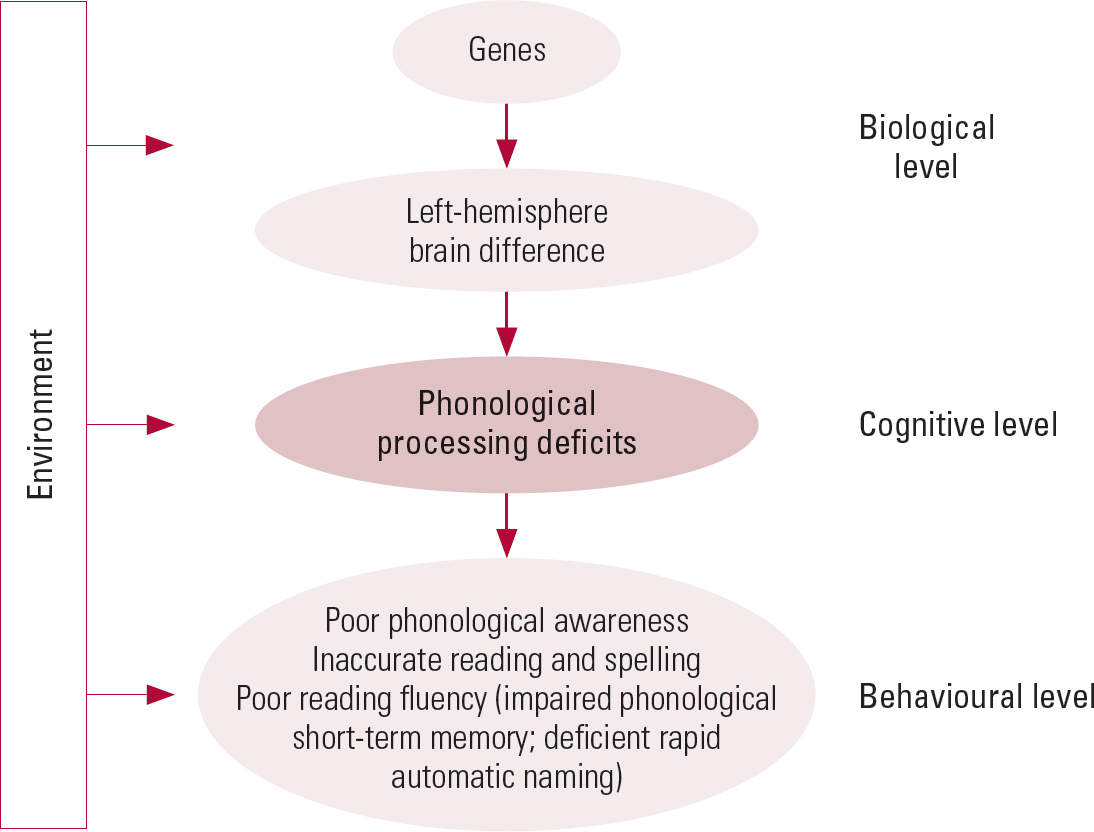
FIG 4 A simplified causal model of developmental dyslexia (based on Reference MortonMorton 2004).
Although dyslexia is the best researched of all specific developmental disorders and there has been vast improvement in our understanding of its cognitive basis, several questions remain unanswered. In spite of the evidence against the IQ discrepancy definition, most descriptions and definitions, including that of the International Dyslexia Association given above, continue to use it under the umbrella of ‘unexpected in relation to other cognitive abilities’. Even though there is general agreement that dyslexia occurs in children across the full range of IQ, there is little literature on dyslexia in populations with intellectual disability. The difference between IQ-discrepant and IQ-consistent reading disability has received little attention. The literature on developmental dyslexia in adulthood and its relationship, if any, to adult mental health is very limited. There is also the question of whether the term dyslexia should be retained or discarded in favour of the general phrase reading disability. No doubt ICD–11 and DSM–V will reflect some of the advances made in the past four decades.
In my next article in Advances (Reference ThambirajahThambirajah 2010) I discuss clinical aspects of dyslexia.
MCQs
Select the single best option for each question stem
-
1 In developmental dyslexia (specific reading disability) the reading difficulties occur at the level of:
-
a reading comprehension
-
b syntax
-
c semantics
-
d single-word recognition
-
e sentence reading.
-
-
2 According to the current view, the primary deficit in developmental dyslexia is:
-
a poor short-term memory
-
b phonological processing deficits
-
c visual perceptual dysfunction
-
d cerebellar dysfunction
-
e impaired temporal sequencing abilities.
-
-
3 Research in developmental dyslexia shows that:
-
a genes that cause dyslexia have been identified
-
b specific brain areas underperform during reading tasks
-
c environmental factors are of little importance in its aetiology
-
d the reading difficulties improve over time
-
e it is invariably associated with high IQ.
-
-
4 Epidemiological studies show that developmental dyslexia is a
-
a discrete condition
-
b equally prevalent in girls as in boys
-
c normally distributed in the population
-
d best classified categorically
-
e best conceptualised as the lower extreme in the distribution of reading skills in the population.
-
-
5 Cross-linguistic studies in developmental dyslexia show that:
-
a it is as common in Germany as in the USA
-
b it does not occur in linguistic groups that use a logographic writing system such as Japanese and Chinese
-
c it is more common in English-speaking countries
-
d the manifestations of dyslexia are the same in all languages
-
e there is no language barrier.
-
MCQ answers
| 1 | d | 2 | b | 3 | b | 4 | e | 5 | c |



eLetters
No eLetters have been published for this article.