



No CrossRef data available.
Published online by Cambridge University Press: 20 November 2024
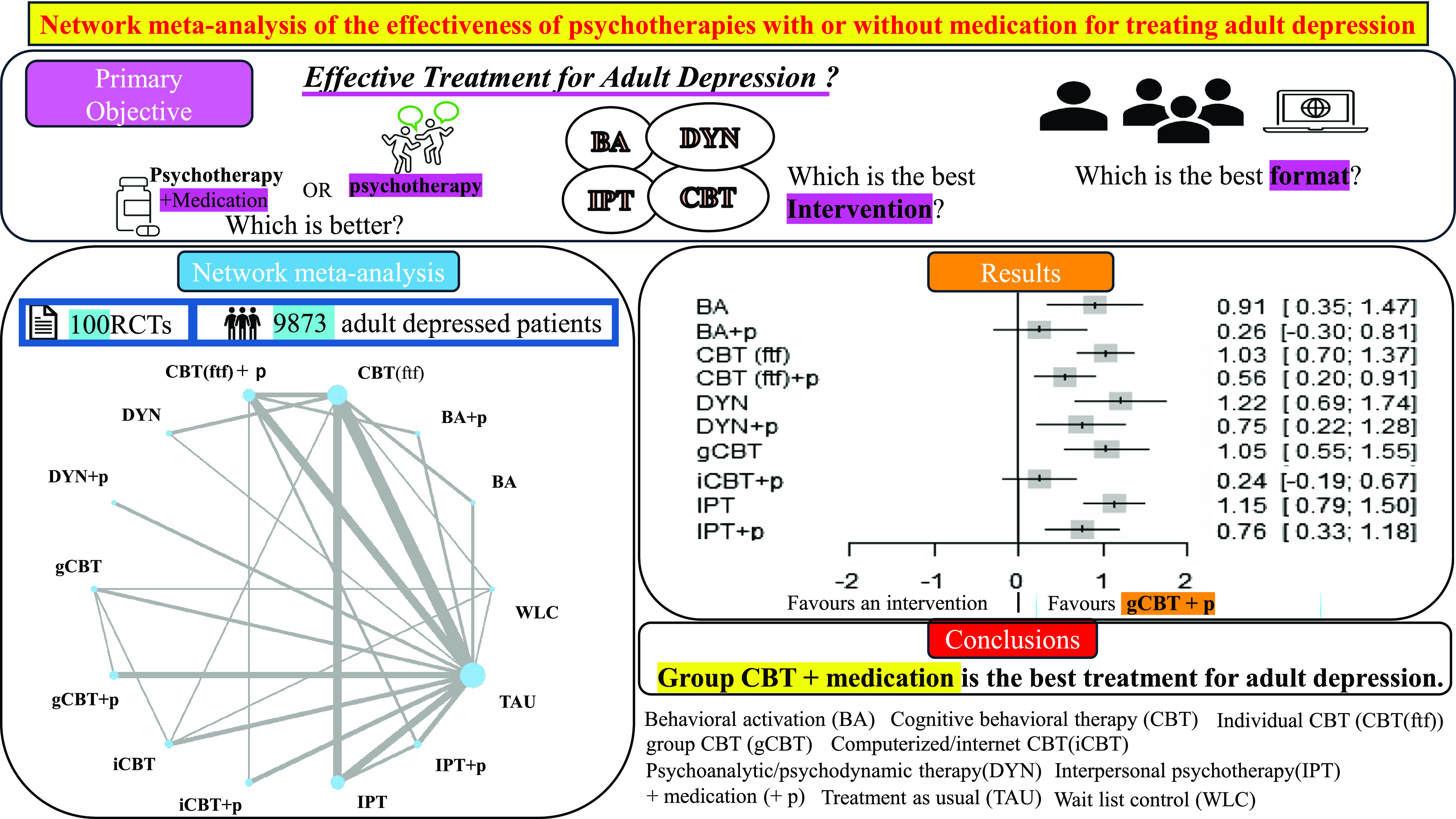
To ascertain whether psychotherapies combined with medication are more efficacious than those without medication and determine which combinations yield the best results.
We conducted a network meta-analysis of randomised controlled trials (RCTs) comparing behavioural activation (BA), psychoanalytic/psychodynamic psychotherapy (DYN), interpersonal psychotherapy (IPT), individual face-to-face cognitive behavioural therapy (CBT (ftf)), group cognitive behavioural therapy (gCBT), and computerised or internet cognitive behavioural therapy (iCBT) with each other, or with treatment-as-usual (TAU) and wait list control (WLC) among adults formally diagnosed with depression. The psychotherapy arms were categorised as either psychotherapy alone or psychotherapy combined with medication (+ p). Treatment efficacy was assessed based on depression severity. We used a random-effects model to conduct a pairwise meta-analysis.
A total of 100 RCTs with 9,873 participants were included. The most common treatment was CBT (ftf) alone. All treatment arms were compared with TAU. Most psychotherapies combined with medication were superior to psychotherapy alone. In the subgroup analyses according to the baseline severity of depression, most psychotherapies combined with medication were more effective than psychotherapy alone in moderate-to-severe depression, whereas in mild depression, such differences were not observed. Among psychotherapies with medication, gCBT + p was significantly more effective than TAU and other psychotherapies in both the main and subgroup analyses.
The efficacy of depression treatment varied depending on the severity of the depressive condition. Notably, gCBT + p was identified as the most effective approach for treating adult depression.

