This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/eurpsy/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.

Intensive home treatment (IHT) for people experiencing a mental health crisis has been progressively established in many western countries as an alternative to in-ward admission. But is this a real alternative? We previously reported that patients treated in our IHT unit only differ from those voluntarily admitted to hospital in suicidal risk and severe behaviour disorders (not in other factors such as clinical severity) (Martín-Blanco et al., Rev Psiquiatr Salud Ment 2022;15:213-5). Now we are interested in disentangle if those patients who used to require inward management can be successfully treated at home.
To describe subsequent treatment trajectories of the first 1000 admissions to our IHT unit and to compare clinical characteristics among the different groups of trajectories.
Retrospective cohort study. Subsequent treatment trajectories were collected from December 2016 to October 2022 and classified: absence, hospital, IHT, and mixed (hospital and IHT). Statistical significance was tested by means of ANOVA or Kruskal-Wallis test for quantitative variables (corrected for multiple comparisons) and chi-square tests for qualitative variables.
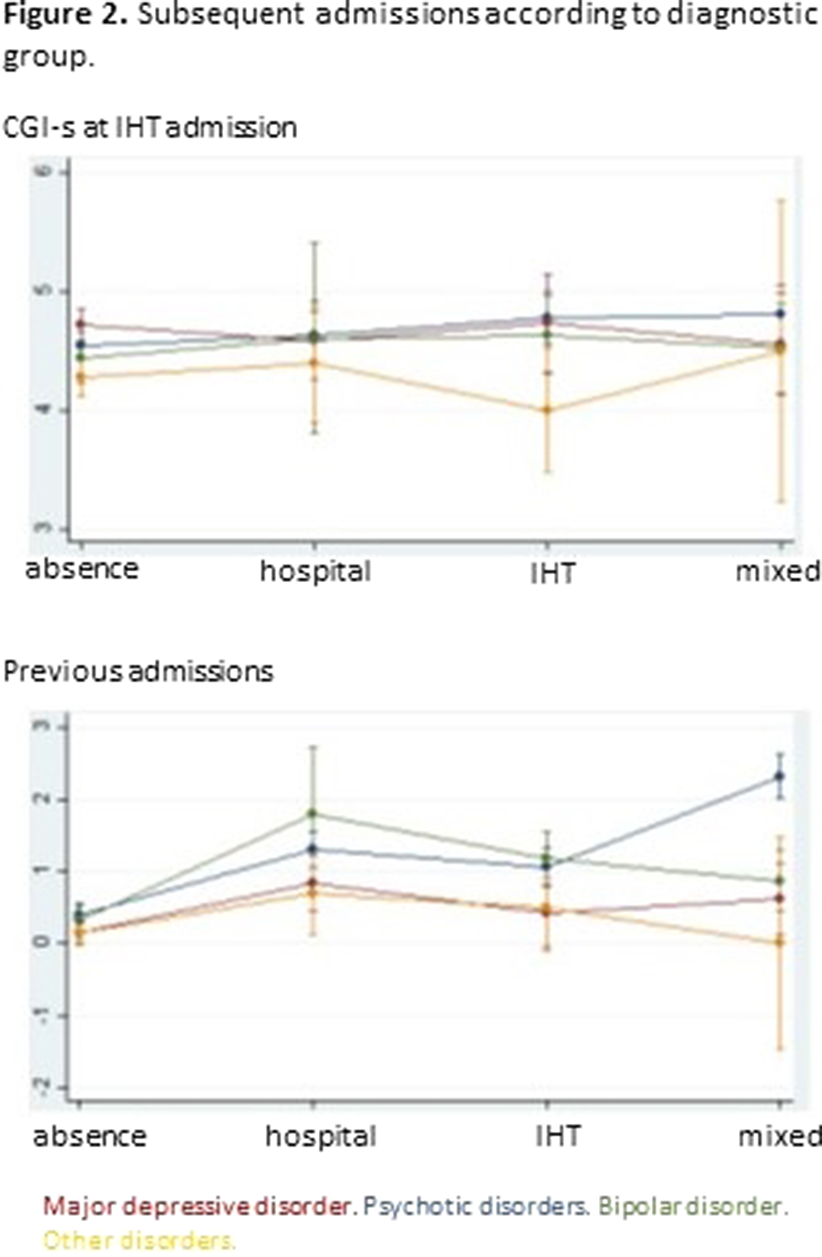
Tables 1 shows the characteristics of the whole sample. Of the 1000 IHT admissions, 12.1% needed subsequent hospital admission(s), 12.7% IHT admission(s), and 9.3% mixed admission(s). There were no differences among these groups in median severity at IHT admission, but there were differences in the number of previous admissions (p=0.0001): the group with no subsequent admissions had less previous admissions than the other groups (pBonf<0.0001), and the group with subsequent IHT admissions had less than the group with mixed admissions (pBonf=0.0123). There were differences between groups regarding distribution of diagnoses (p<0.0001) (Fig. 1). When considering subsequent admissions by diagnosis, there were differences in severity at IHT admission (p=0.0068) and in number of previous hospitalizations (p<0.0001) (Fig. 2). CGI-s: clinical global impression - severity. * median and IQRmean SD Age (years) 47.07 17.02 CGI-s at admission * 5 4-5 N % Sex (female) 548 54.8% Psychotic disorders 463 46.3% Affective disorder 257 25.7% Bipolar disorder 128 12.8% Other disorders 152 15.2% Hospital admission in the previous 5 years 313 31.3%
Image:
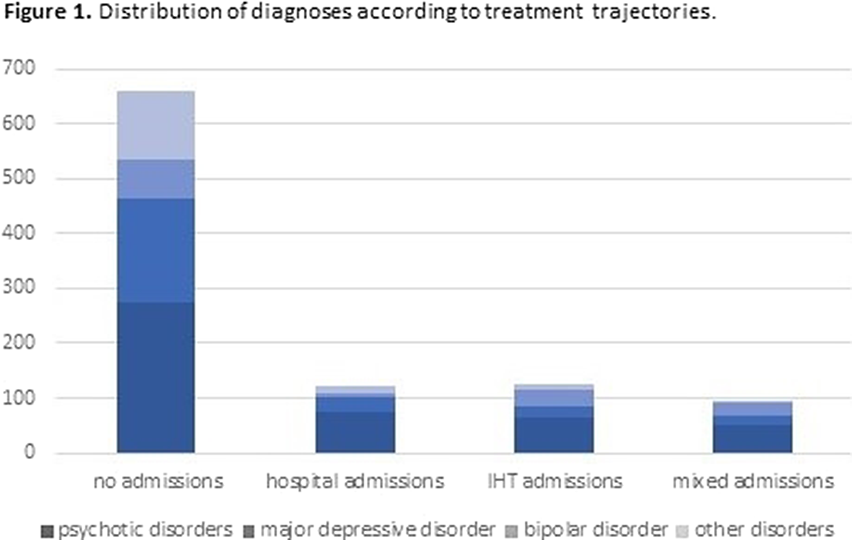
Image 2:
Patients that used to require inward management can now be treated at home when suffering an acute episode. Therefore, IHT has changed treatment trajectories for some patients with psychiatric disorders.
None Declared
The threat and preservation of the territorial integrity of Ukraine are not new issues. During the last decade, peacetime (Peace, until 2013) was disrupted by active hostility (AH, 2014–2015) and trench warfare (TW, 2016–2021). War exert acute and chronic impacts on mental health, may be a substrate for mental health disorders, especially worrisome since, today, the large-scale conflict has demanded the recruitment of adult civilians to defend and fight alongside armed forces troops.
The analysis aimed to unveil the impact of those conflicts on the mental health of the army and help us to anticipate risk factors (ranks, time period) and need for resources (admissions and days of hospitalization per time period, rank and disease).
A retrospective cross-sectional analysis of an anonymized part of the internal database included 3995 anonymized records.Data are expressed as the frequency (%), fold-increase, or mean ± SEM. Chi-square analysis and ANOVA with Bonferroni post hoc correction were performed with Jamovi.
The temporal distribution of admissions (Figure 1) showed a 6.97 (AH) and 3.62 (TW) [5.02 (TW1, 2016–2017), 3.91 (TW2, 2018–2019), and 1.95 (TW3, 2020–2021)] fold increase per year compared to peacetime. The most frequent mental health problems, accounting for 76.1% of cases, were ‘anxiety, dissociative, stress-related, somatoform and other nonpsychotic disorders’ (F40-F48, ANXd, 40.1%) and ‘mental and behavioral disorders due to psychoactive substance use’ (F10–F19, PSUd, 36.0%). ‘Reaction to severe stress and adjustment disorders (F43, 76.5%) and ‘Alcohol-related disorders (F10, 89.3%) were the predominant mental health disorders, respectively.
The ICD-10 category depended on the war period (Figure 2), with peacetime to TW2 accounting for 90% of cases. ‘ANXd’ were the main mental health problem in any period, with 61.8% of cases occurring in peacetime. PSUd, residual in peacetime 6.1%, reached their peak in active hostility (47.4%), with 97.9% of ‘Alcohol-related disorders’ as the cause of these admissions, which could agree with the use of alcohol serving as a coping mechanism in front traumatic events. In trench warfare, PSUd decreased (TW1, 39.2%; TW2, 25.1%).
Hospital stays for people with ANXd or PSUd lasted at least one month in peacetime but significantly decreased in war periods (Figure 3). This could be explained by a ‘need for free beds effect’ and the distribution of admissions by ranks.
Image:

Image 2:
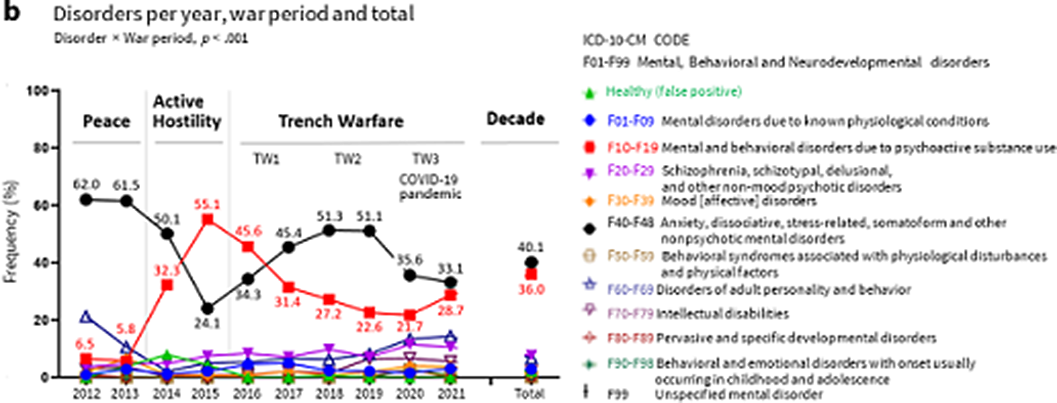
Image 3:

-
The dominance of ANXd, mainly among professional soldiers and high ranks, points to the need for rank-tailored psychological training in skills to reduce the ANXd burden.
-
The large number of PSUd in nonprofessional soldiers during wartime dictates the need to strengthen the selection of military personnel.
-
Hospitalizations in military operations are heterogeneous and depend on the military rank.
None Declared
