This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/eurpsy/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.

Repetitive Transcranial Magnetic Stimulation (rTMS) is a new emerging neuromodulation treatment that has been tried for multiple psychiatric conditions [1, 2]. Its major approved application is treatment-resistant depression (TRD) [1]. At the same time there is a perceived potential for its use for other clinical conditions, primarily other mood and anxiety disorders [2]. At Homewood Health Centre we have been using rTMS as an adjunct treatment for patients with TRD and multiple comorbidities.
To evaluate the effectiveness and feasibility of rTMS in complex clinical populations.
Observational study. Quick Inventory of Depressive Symptomatology (QIDS). Generalized Anxiety Disorder Questionnaire (GAD-7). Descriptive statistics.
We have treated 30 patients, 12 women (40%) and 18 men (60%), with average age of 42.0±15.6 years. All patients had a primary diagnosis of major depressive disorder. The standard questionnaires were used to quantify the severity of depressive symptoms (QIDS) and anxiety (GAD-7). The average baseline scores for depression and anxiety were 16.1±4.9 and 15.0±4.4, respectively. The patients received an average of 28.1±5.1 treatments. All patients but one received the full course of treatment as planned. The average end-of-treatment (EoT) scores for severity of depressive symptoms and anxiety were 9.6±6.5 and 7.3±5.3, respectively. The rates of improvement and remission for depressive symptoms were 66.7% and 36.7%, respectively. The rates of improvement and remission for anxiety symptoms were 76.9% and 30.8%, respectively.
Image:
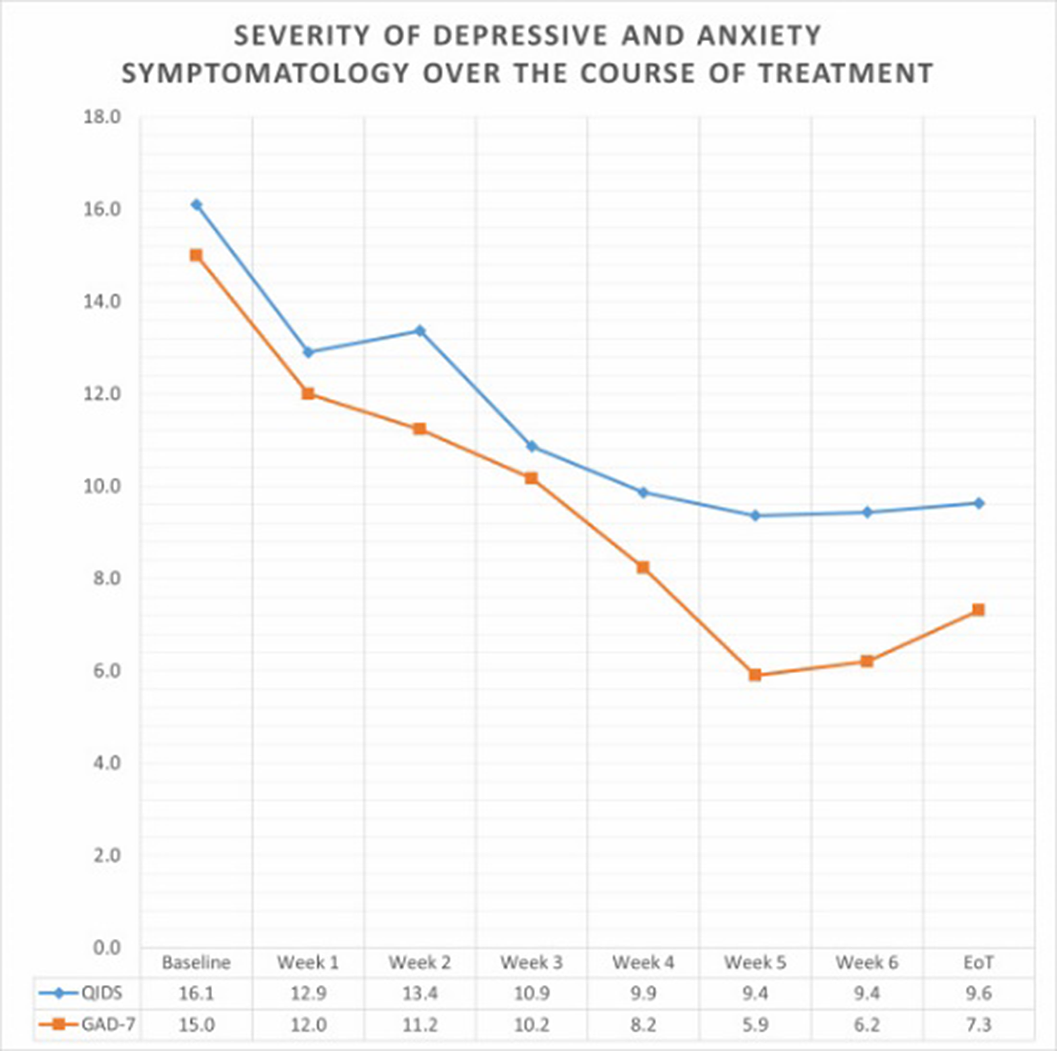
Our data indicate that rTMS provides significant improvement and recovery rates in complex clinical populations and is well-tolerated. While further research is required, we recommend wider implementation of rTMS for treatment of mood and anxiety disorders.
1. Brunoni AR, Chaimani A, Moffa AH, Razza LB, Gattaz WF, Daskalakis ZJ, Carvalho AF: Repetitive Transcranial Magnetic Stimulation for the Acute Treatment of Major Depressive Episodes. JAMA Psychiatry 2017, 74(2):143.
2. Somani A, Kar SK: Efficacy of repetitive transcranial magnetic stimulation in treatment-resistant depression: the evidence thus far. Gen Psychiatr 2019, 32(4):e100074.
None Declared
The fact that nurses do not have a voice in the treatment decision of patients and that there is no framework about futile treatments can cause some psychological problems such as depression, burnout and moral distress (Yildirim et al., 2018). If not managed properly, moral distress leads to decreased job satisfaction, increased nurse turnover rates and intent to change the working area or leave the profession (Vieira & Doedato & Mendes, 2021).
This study aimed to explore the nurses’ attitudes towards futile treatments and its relationship with the moral distress, intention to leave the job and the other personal factors.
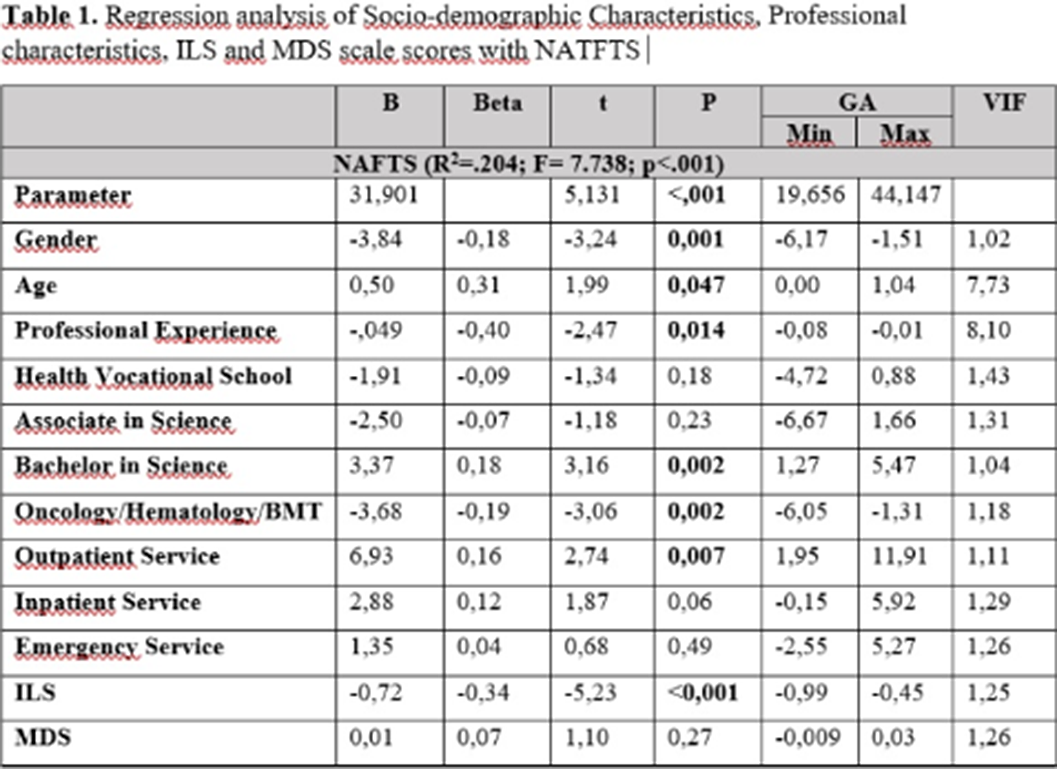
This study has a descriptive and correlational design, carried out with 425 nurses, between April-May 2021 in Istanbul. The data were collected using a Personal Information Form, The Nurses’ Attitudes Towards Futile Treatment Scale(NATFTS), Moral Distress Scale(MDS) and Intention to Leave Scale (ILS). Personal Information Form: The form consists of 22 questions including the socio-demographics and professional characteristics. The Nurses’ Attitudes Towards Futile Treatment Scale (NATFTS): The scale was developed by Yildirim et al. in 2019, consisting of 18 items and uses a 5-point likert type scale.Moral Distress Scale(MDS):The scale, developed by Hamric (2012), adapted to Turkish by Karagözoğlu et al. (2017), consisting of 21 expressions, was designed to measure the level of moral distress in nurses. Intention to Leave Scale (ILS):The scale was developed by Wayne et al. (1997), and adapted to Turkish by Avcı ve Küçükusta(2008) in the form of 5 items. The data were analyzed by using descriptives, Kruskal Wallis test, Independent Samples t- test and ANOVA, Pearson Correlation analysis on SPSS 25.0 for Windows. For significance, p < .05 and 95% CI were assumed in the data analysis.
A moderate negative correlation was found between NATFTS score and the ILS score (r=-0.356, p<0.001). Nurses who think that futile treatments should be applied under the strict rules have less tendency to leave their jobs. On the other hand, there was a lower positive level of correlation between NATFTS score and the MDS score (r=0.295, p<0.001). That is, nurses who think that futile treatments should be applied under the strict rules have a higher level of moral distress. A low-level negative of relationship was found between the MDS score and the ILS score (r=-0,260, p<0,001). As the level of moral distress increases, the tendency to leave work decreases.
Image 2:
It is believed that educating nurses and strengthening them psychologically will prevent them from experiencing moral distress, increase job satisfaction and reduce intention to leave (Cicolini et al., 2014). Considering the negative effects of ethical dilemmas about futile treatments on health professionals, it is recommended that legal regulations be made on the subject and institutions determine their own protocol.
None Declared
Coercion is a general term used to refer to a series of actions, ranging from involuntary treatments to forced interventions, which can be ethically, legally and clinically challenging for both professionals and service-users. Perception of healthcare professionals on restraint practices is in important factor determining the clinical outcomes.
The aim of this study was to determine i) the differences between the estimates of healthcare professionals working in the Emergency Unit of Erenköy Psychiatric and Neurological Training and Research Hospital (Erenköy RSHEAH) regarding physical restraint practices and the real use and outcome values ii) the knowledge, attitudes and opinions of healthcare professionals on such procedures.
The study was designed as a descriptive cross-sectional online survey. All healthcare professionals working in the Emergency Unit of Erenköy RSHEAH (with a catchment area of 5 million people) who agreed to participate in the study and who were not part of the research team were included. Sociodemographic information, information about working experience, and estimates of physical restraint practices in the last month were questioned. Attitudes and opinions towards these practices were evaluated with 5-point Likert-type questions. Ethical approval was obtained from Erenköy RSHEAH Clinical Ethics Committee (Decision No: 40, 18.07.2022).
A total of 55 healthcare workers (31 trainees, 10 specialist psychiatrists, 6 nurses, 8 security personnel) participated in the study. The mean age of the participants was 32±6.4 years (24-50, min-max) and 52.7% were female. The mean duration of employment in the health sector and current institution were 6.6±5.7 (1-22, min-max), and 4.1±4.1 (1-17, min-max) years, respectively. The estimated mean rate of physical restriction was 13.5±13% (2-60, min-max). However, the actual median rate was 4% (0 - 8.8% min-max) in the same month. The estimated mean duration of physical restraint was reported as 87.8±54.1 (20-300, min-max) minutes, whereas the median actual duration of physical restraint was 60 minutes. No significant relationship was found between the estimates of duration, rates and complication rates of of physical restraint and the duration of professional experience (p>0.05). A significant difference was found between professional groups in terms of restraint duration and complication rate (p<0.05), as well as their opinions regarding the appropriateness of restraint practices with the legal framework (Table 1).
Image:
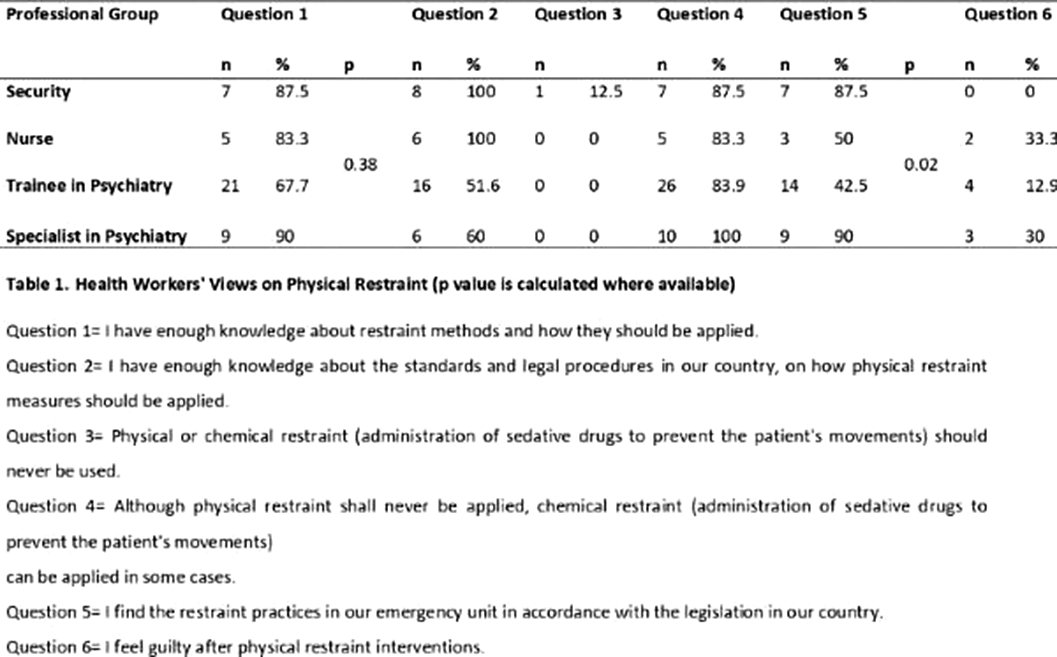
It was observed that healthcare workers had a misperception regarding the rate and duration of physical restraints, which were perceived as higher than the actual values. Thus, the restraint interventions were perceived to be more negative than they actually are. Correction of such misperceptions should become part of the continous educational processes of all professional groups.
None Declared
