This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/eurpsy/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.

Since the beginning of the modern psychiatry the acute units have established a “locked door” policy. Some studies show that this condition may increase patient’s discomfort and affect the perception of health quality of care (Boyer L, 2009, Eur Psychiatry Dec;24(8):540-9). Lately, several European countries such as Germany, Switzerland and Spain are starting to implement the “open-door” policy but its impact on patient’s satisfaction is still unknown (Hochstrasser, L, Frontiers in Psychiatry, 9(57). https://doi.org/10.3389/fpsyt.2018.00057) .
To help characterize the advantages of the “open-door” policy implemented in an acute inpatient psychiatric unit in order to assess the patient’s view of it.
This is a descriptive observational study carried out at an inpatient psychiatric unit. Data were collected after the implementation of the open door policy on June 2019, assessing the patient satisfaction of 31 subjects who completed the SATISPSY-22 scale at the time of discharge. Results are described using the average and its standard deviation.
Results show scores in all items above 50 points, being the care team and the quality of care the most valued ones with 82 and 79 points respectively. The overall score is above 65 points (Fig. 1).
Image:
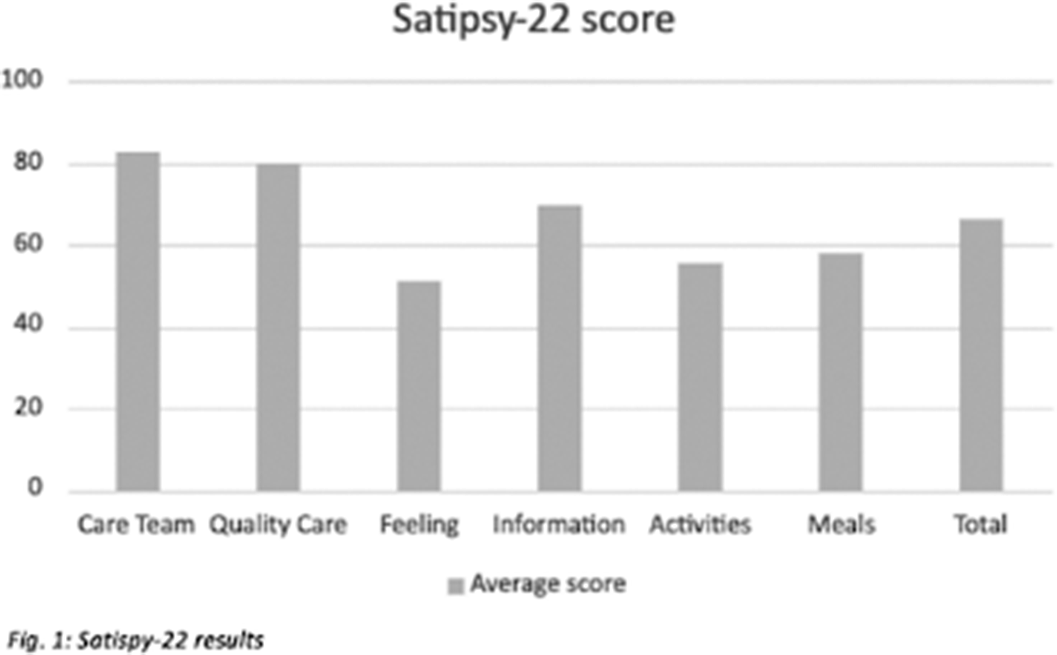
In line with previous studies, our data suggests that the main impact of the “open-door” policy implementation is on patients’ perception of the care, being Quality of care and satisfaction with the Staff the items with highest scores. This could be explained by patients trusting more in the Care team, which would help enhance the therapeutic relationship improving therapeutic adherence, treatment adequacy and the outcome. Nevertheless, the Feeling related to hospitalisation was found to be the item with the lowest score. This could mean strategies should focus on improving patient’s insight regarding their clinical state and their need to be admitted. Our study supports the hypothesis that open-door policy in acute psychiatric units is seen positively by patients and that further research should be carried.
None Declared
Schizotypy refers to a continuum of symptoms from subclinical manifestations in the general population to severe symptoms in schizophrenia spectrum disorders. Neuroimaging studies revealed significant relationships between schizotypy and cortical anatomy in the general population. However, it remains unclear whether these structural associations has a gender specificity.
The present study used structural MRI data to investigate the relationship between subclinical schizotypy symptoms and cortical and subcortical morphometric measures in male and female samples of healthy individuals.
164 right-handed healthy unmedicated individuals (18.0-34.9 years, 57% females) underwent structural MRI at 3T Philips scanner. T1-weighted images were processed via FreeSurfer 6.0 to quantify cortical thickness for 34 regions-of-interest (ROIs) according to Desikan atlas and volumes for 7 subcortical structures at each hemisphere. Schizotypy levels were assessed using self-report Schizotypal Personality Questionnaire, total schizotypy score and 4 factors scores (Cognitive-perceptual, negative, disorganized and paranoid factors as per Stefanis et al. Schizophr Bull. 2004; 30 335-350) were calculated. Partial correlation analysis (ppcor version 1.1, R version 4.2.1) was used to assess the associations between ROIs cortical thickness and total schizotypy or 4 factors scores including age and sex as covariates. The same analysis was performed for subcortical volumes including intracranial volume as additional covariate.
In male group we revealed a positive correlation between greater thickness of the left caudal middle frontal gyrus and higher total schizotypy (r=0.42, punc=0.0003, 95% CI [0.21–0.60]) and negative factor of schizotypy (r=0.49, punc<0.0001, 95% CI [0.28–0.65]) (Image). No correlations survived correction for multiple comparisons in female sample. There were no differences in age, caudal middle frontal gyrus thickness, total schizotypy or negative factor of schizotypy scores between male and female subgroups.
Image:
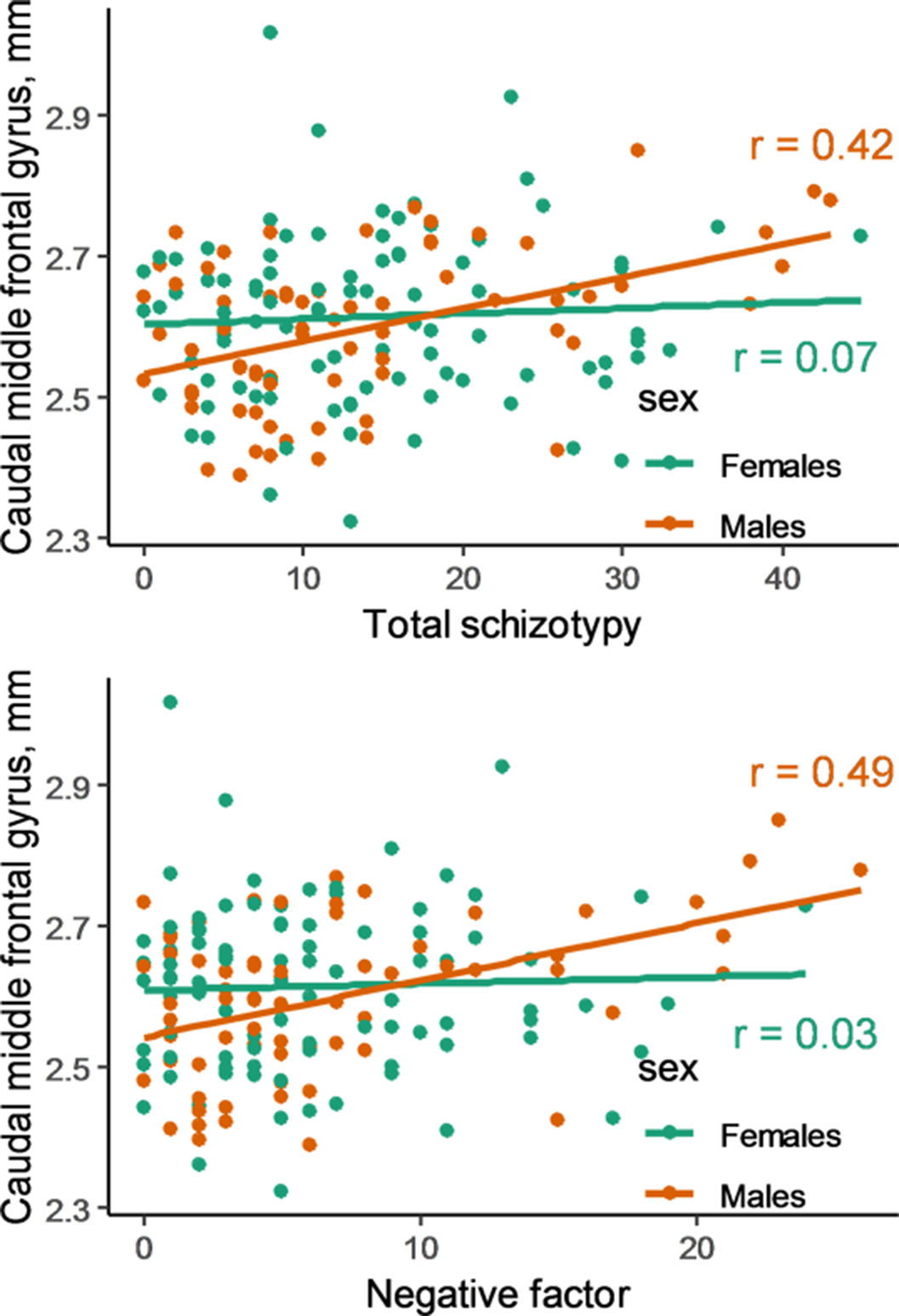
The results suggest that the association of dorsolateral prefrontal cortex (DLPFC) and levels of schizotypy is gender specific. We showed that total and negative schizotypy positively correlated with thicker DLPFC in male but not in female sample. The present data are inverse to findings of prefrontal cortical thinning observed in schizophrenia. Such correlations suggest that thicker cortex could be a potential compensatory mechanism or could reflect alterations in trajectory of cortical thickness reductions across the lifespan.
The work was supported by RFBR grant 20-013-00748
None Declared
There is growing evidence to suggest that delusions in schizophrenia-spectrum disorders are associated with altered brain connectivity. Disruptions in long association fibers, such as the superior longitudinal fasciculus, are among the most consistent findings in psychosis. However, functional connectivity (FC) correlates of such structural alterations and their implications in delusional symptoms remains unclear.
The study used a hypothesis-driven approach and aimed at exploring structural connectivity (SC) disruptions of the left superior longitudinal fasciculus (part with parietal terminations, SLFP) and their FC correlates in a group of psychotic patients with persistent delusions across diagnostic categories within the schizophrenia-spectrum.
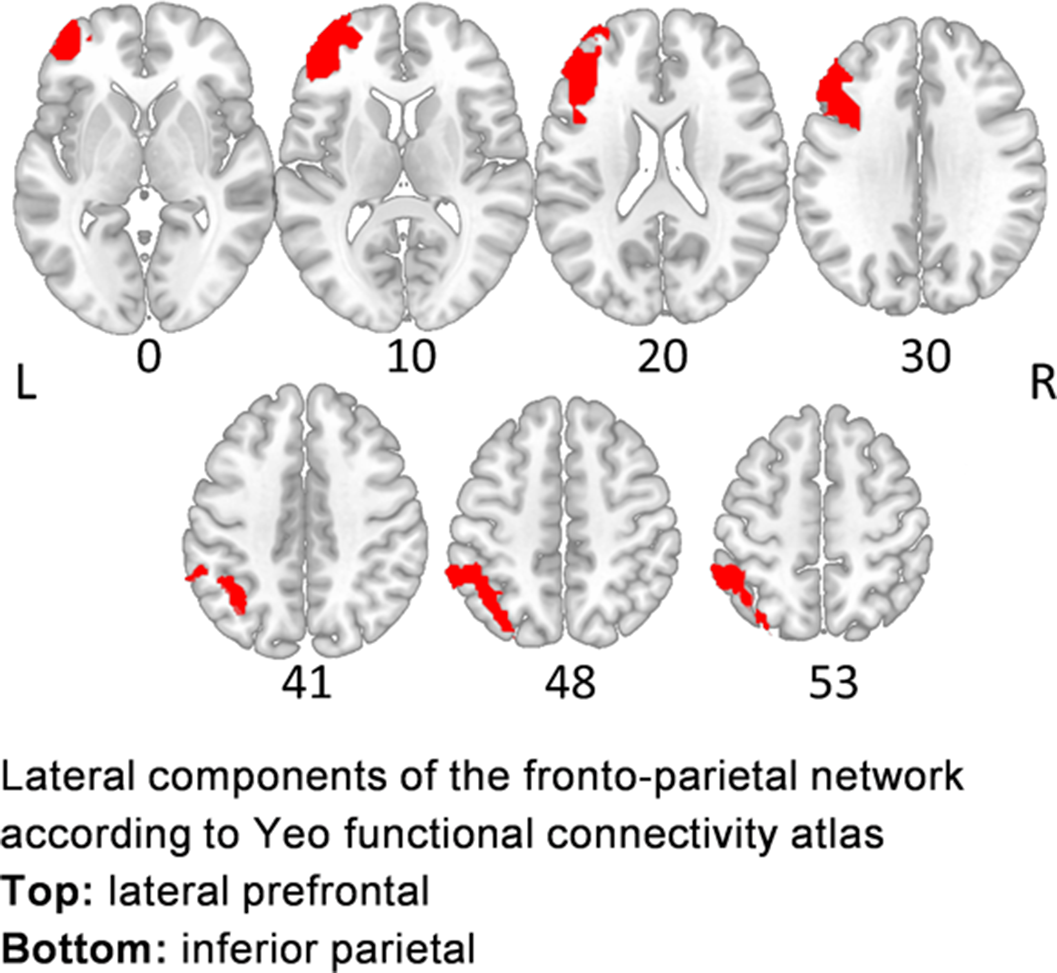
Sixteen right-handed patients (23.1-53.8 years, mean age 39.6±8.5, 44% females) with delusional disorder (DD, n=10) and schizophrenia (SCZ, n=6), presenting with persistent delusions, and 16 matched healthy controls (23.0-56.4 years, mean age 38.9±11.1, 44%females) underwent diffusion-weighted 3T MRI (DW-MRI), while patients additionally underwent resting-state 3T fMRI (rsfMRI). DW-MRI data were processed via FreeSurfer6.0 and TRACULA to derive axial (AD), radial (RD) diffusivities and fractional anisotropy (FA) for left SLFP. rsfMRI data were processed with SPM12 and Conn v19c to calculate ROI-to-ROI FC between lateral prefrontal and inferior parietal components of the frontoparietal network (FPCN) according to Yeo atlas (Yeo et al. J Neurophysiol. 2011; 106(3) 1125-65), which is sought to represent cortical projections of the SLFP (Image). Partial rank-based correlation analysis (with age and sex as covariates, ppcor v1.1, R v4.2.1) was used to explore the associations between SC and FC measures involving the SLFP, PANSS and BABS scores.
Compared to healthy controls, patients showed decreased AD in left SLFP [F(1, 28)=14.9, p=0.0006; Cohen’s d = −1.3, 95% CI: −2.1 to −0.5]. No RD or FA alterations were found. We revealed a correlation between AD in left SLFP and fronto-parietal FC within the FPN (r = 0.58, p = 0.031) in patients. Correlation between FC and PANSS total score (r = −0.54, p = 0.045) did not survived correction for multiple comparisons. No other correlations between SC or FC, chlorpromazine equivalents and clinical scores were revealed.
Image:
The findings suggest that the structural connectivity disruptions of the SLFP may mediate FC strength within the FPN in patients with persistent delusions. However the limited sample size and the lack of correlations between connectivity measures and clinical scores do not allow to conclude definitely whether the revealed structural-functional connectivity pattern underlies delusional symptoms, which should be elucidated via further research.
This study was supported by RFBR grant 21-515-12007
None Declared
Frontotemporal dementia (FTD) is the second most common type of dementia seen between 45-65 years of age and affects the frontal and/or temporal lobes. FTD is clinically characterized by progressively the change in behavior, personality, and language dysfunctions.
Clinical features of FTD include restlessness, disinhibition, apathy, blunted affect, avolition, social withdrawal, impulsiveness, and loss of executive function. Most patients with FTD act as socially inappropriate behaviors, not talking much, compulsive-like acts, poor insight, and psychiatric features including hallucinations and paranoid delusions. According to symptoms, the diagnosis of FTD may be confused with depression, mania, or schizophrenia.
In this case report, we wanted to draw attention that FTD should be considered in the differential diagnosis of late-onset psychosis.
A 53-year-old female, married, uneducated, and not having children patient has applied to our clinic with complaints, that started a year ago, about social withdrawal, activity, decreased sense of purpose, neglecting personal hygiene, not eating well, and acting inappropriately and impulsively.
The patient reported that she was walking out of the house for hours, having profanity speeches, and forgetfulness.
She was admitted to the psychiatry hospital a year ago and discharged with a diagnosis of bipolar disorder.
Brain MRI showed atrophy of frontal and anterior temporal structures bilaterally. PET scan demonstrated left frontal, parietal, and temporal hypo perfusion of the brain.
In our clinical observation, she had apathy, inappropriate jokes, lack of eye contact, flat affect, lack of gesturing when communicating, unable to respond to questions, and visual hallucinations.
Due to the similarity of the clinical resemblance of BPAD and FTD, the diagnosis of FTD can be confusing. In this case, amnesia and sudden onset of the symptoms with rapid destruction may help the diagnosis of FTD.
Psychosis symptoms in our clinical observation also suggested the diagnosis of psychosis. However, its atypical course and early-onset psychosis symptoms brought us closer to organic pathology. Investigations of structural and functional brain imaging may help support the diagnosis.
Image:
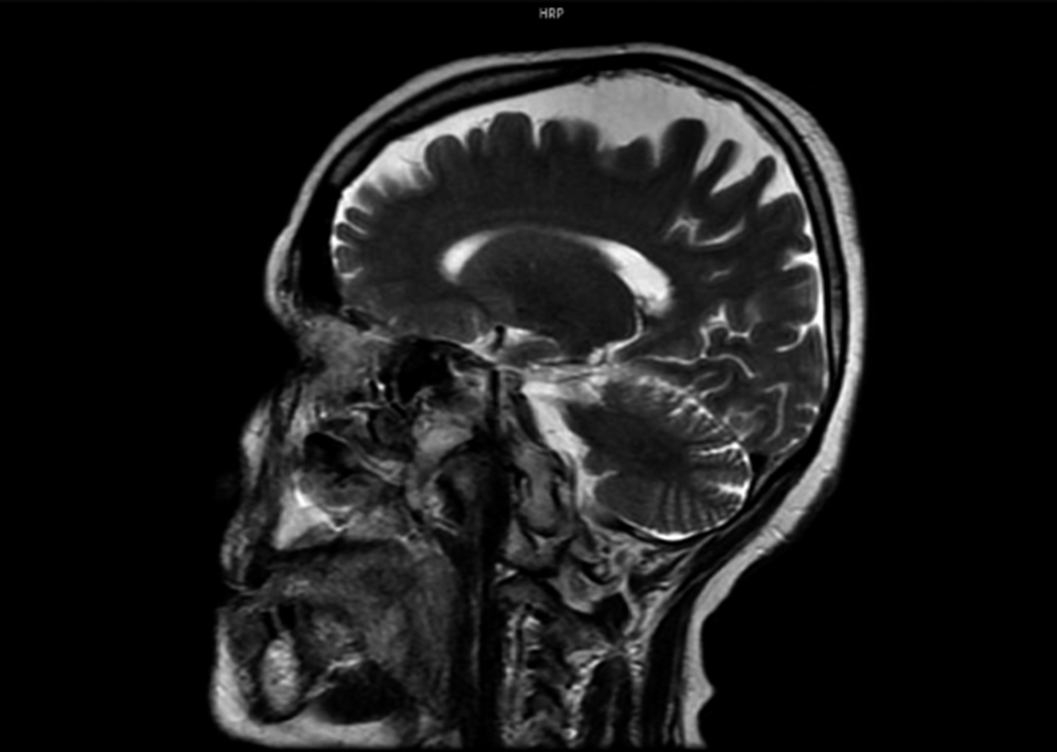
Image 2:
Psychiatric symptoms in FTD may cause misdiagnosis. Organic pathologies should be kept in mind, especially in late and sudden onset symptoms.
None Declared
