This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/eurpsy/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.

The physiopathology of patients with treatment-resistant obsessive-compulsive disorder (OCD) may differ from that of treatment-responsive patients. Cognitive evoked potentials may be one of the ways to detect these differences. The error-related negativity (ERN) is an electrophysiological correlate of error detection during the execution of a motor task, which is larger in patients with OCD than in typical people. According to the literature, the ERN could vary according the patients’ treatment-resistance.
The main goal of this study was to assess whether the ERN, which begins 20 ms before the motor response and reaches its maximum 80 ms later, was different between non-resistant and highly resistant OCD patients.
Forty-seven OCD patients and their age- and gender-matched controls were asked to perform a flanker task while the potentials evoked by their motor responses were recorded. For each participant, the difficulty of the task was adjusted to get an error rate of about 20%. Treatment-resistance was evaluated using Pallanti and Quercioli’s (Prog Neuropsychopharmacol Biol Psychiatry 2006; 30 400-412) resistance scales.
In all participants, response errors evoked an ERN at fronto-central electrodes [Fz, FCz, red and green lines on the figure], whereas the negativity was absent or smaller for correct responses (black and blue lines on the figure, both ps < .01). As expected, the ERN of OCD patients was consistently larger and of longer duration than that of control participants (compare the green and blue lines with the red and black ones, respectively). Interestingly, the amplitude of the potentials evoked by correct responses at central and centro-parietal electrodes on the left side of the brain [C5, C3, CP5] was significantly less negative in treatment-resistant patients (all ps < .05). In control participants, the ERN recorded at fronto-central electrodes were followed by a positive wave which reached its maximum between 170 and 270 ms after the response, and was larger after errors than after correct response. In OCD patients in contrast, this positive wave was absent whether the response was correct or not.
Image:
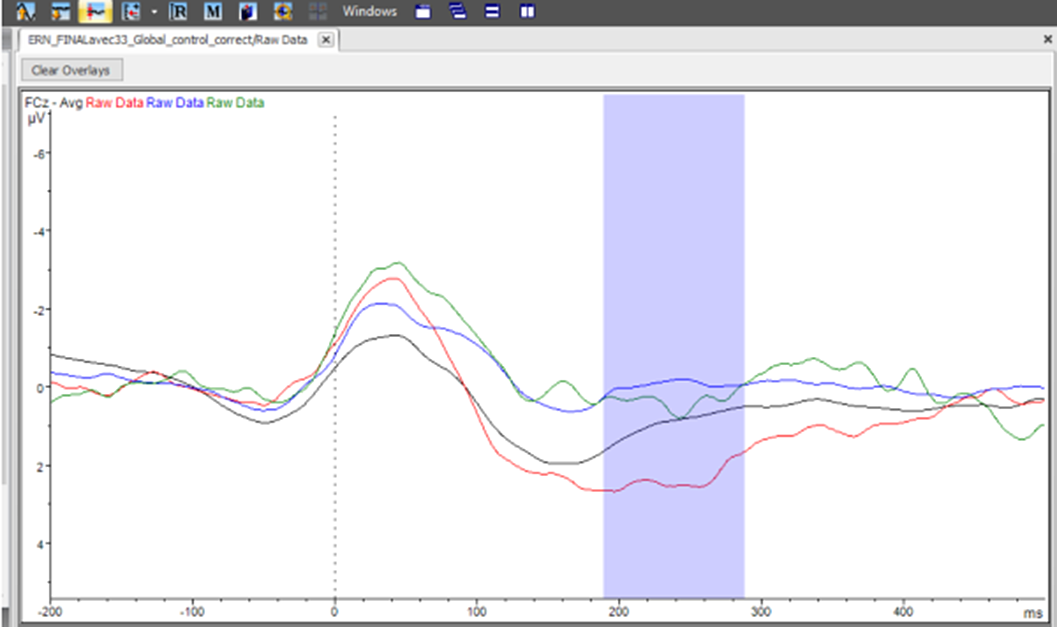
The significant correlation observed between OCD patients’ treatment resistance and the potential evoked by correct responses on the left side of the brain suggest that this potential could be used as a marker of treatment-resistance. The absence in OCD patients of the positive wave that follows the ERN in control participants suggests that OCD patients were not fully aware of whether or not their response was correct.
None Declared
During the second wave of Russia-Ukraine war, around 8 million were internally displaced. Negative mental health impact of the war cannot be underestimate. Among internally displaced persons (IDPs), particularly vulnerable category is people with neurocognitive deficits. Stress associated with displacement may cause a change not only in cognitive functions, but also affect the onset or evaluation of behavioral and psychological symptoms.
to study the prevalence of neuropsychiatric disorders in hospitalized patients with dementia, who were internally displaced and to compare with general population frequency.
64 IDPs with dementia (moderate and severe neurocognitive deficits) who were examined during March-September 2022. Cases of newly arrived persons were taken into account, after 1 to 30 days had passed since their relocation. The diagnosis was verified based on the ICD-10 criteria (F00-F01). The degree of neurocognitive deficit was determined using the MMSE and MoCA tests. Affective pathology was studied using the HAM-D, HAM-A, PHQ-9, AES scales. Psychotic symptoms and behavioral disorders were studied based on clinical examination and medical records. The study was conducted in Lviv Regional Psychiatric Hospital.
among the examined patients, 60 (94% of all examined) had neuropsychiatric disorders. Among this sample, neuropsychiatric symptoms (an isolated symptom or a combination of two or more symptoms) occurred with the following frequency: apathy 16 (26.7%), anxiety49 (81.7%), depressive symptoms 32 (53.3%), agitation and aggression 41 (68.3%), hallucinatory symptoms 8 (13.3%), delusional disorders 34 (56.7%), wandering and disorientation 18 (30%), refusal of food and medicine 12 (20%)
Image:

In this study the frequency of occurrence of certain neuropsychiatric syndromes among IDPs with dementia differed from the studied average frequency of occurrence of the same symptomatology among the general population. In particular, anxiety symptoms among IDPs with dementia occurred 42% more often than on average among patients with dementia in the general population (with a frequency of 81% vs 39%), agitation and aggression - 28% more often (68% vs 40%), and delusions - 16% more often (57% vs 31%). At the same time, symptoms such as apathy (by 19%) and refusal to eat (by 14%) were observed less often among IDPs with dementia than among dementia patients from the general population
None Declared
