Background
Coronavirus Disease 2019 in India
India is 1 of the largest and most populated countries in the world, accounting for approximately 1.3 billion inhabitants distributed over 3,287,263 km2 in both urban and rural areas, with a wide variability in access to medical care. Since the start of the coronavirus disease 2019 (COVID-19) pandemic last year, fears have been raised about the possibility of an uncontrolled spread of the virus in the country, in view of its social, demographic, and urban features. Contrary to predictions, India registered a relatively low incidence of COVID-19 cases in 2020, approximating 10,266,674 cases. Both public health measures and the national health system proved their effectiveness in containing the virus by means of lockdowns in May 2020 together with coordinated clinical management. The vaccination campaign started in January 2021, carrying with it big hopes of health and economic benefits; India being 1 of the largest manufacturers of vaccines in the world. Reference Changoiwala1–Reference Rubin, Baden and Udwadia3
The COVID-19 pandemic has progressed in India, particularly in western and northern areas, secondary to multi-factorial reasons, both virological and social, such as population density and economic migration. This has led to an incidence of approximately 350,000 cases per day in the weeks between May 1, and May 14, 2021 and a daily death toll of approximately 4000 during the same period. Reference Changoiwala1–4 Moreover, rises in cases have been registered in other areas of the country, and there is also a high likelihood of under-reporting of cases and deaths. The Delta (B.1.617.2) variant, also known as the Indian variant, has recently been updated to a Variant of Concern (VOC) by the World Health Organization (WHO). 4
Oxygen Shortage
The current pandemic is testing the adaptability of the oxygen distribution and consumption of many countries of all sizes and economies, including India. Oxygen distribution in India, as in other countries, is mostly assured by the constant refilling of liquid O2 systems by means of tanks and cylinders. Capacity and availability of those systems is highly variable and dependent upon market, local and national policies, as well as supply chain issues, hospital facilities, transport, and logistics. Due to exceptional COVID-19-related circumstances, by mid-April 2021, many reports of oxygen shortages from different health-care facilities started to highlight the unfolding humanitarian crisis that, in a few days, would lead to an international call for help from the Indian government. The overwhelming number of new cases disrupted the health-care system and highlighted the frailty of the oxygen distribution and refilling chain. Many hospitals in the major cities of India had no more capacity to hospitalize patients and clashes and robberies targeting oxygen provisional transports and reserves were being reported. Rural areas suffered from their isolation. The price of oxygen cylinders jumped by around 9-fold, and the national government of India coordinated 1 of the biggest efforts in its history to distribute oxygen all over the country by all means, diverting the industrial oxygen supply chain toward the medical supply of oxygen. 5–Reference Madaan, Paul and Guleria10 Still, the situation was escalating drastically. Following the country’s request for support, the EU Civil Protection Mechanism coordinated the response agreed by EU Member States providing the shipment of oxygen, medicine, and equipment to India. It was in this context that our Emergency Medical Team (EMT)-2, based in and coordinated from Saluzzo, Piedmont Region, Italy, immediately answered the call, bearing in mind the crisis which occurred in northern Italy during the first wave of the COVID-19 pandemic in March 2020. Reference Sacchetto, Raviolo and Beltrando11
The Mission
The team was activated on April 25, 2021, with the main goal of the intervention being set and communicated by the Indian government. In a few hours, a 12-member team was formed, comprised of 1 team leader, 1 deputy team leader, 1 public health medical doctor (MD), 1 infectious diseases specialist MD, 1 emergency medicine MD, 1 intensivist MD, 2 emergency nurses, 2 technicians specialized in logistics and electricity, and 2 experts in oxygen systems. Transport on a C-130 cargo flight was organized thanks to the Italian Civil Protection Department and the Italian Air Force. The mission lasted 12 d, from May 2 to 14, 2021.
Target: the ITBP Referral Hospital
Indo-Tibetan Border Police (ITBP) is a police department with frontier duties. Among other roles, it is involved in health care and enrolls physicians from all specialties to serve the corps and communities. ITBP also has at its disposal the Referral Hospital in Greater Noida, Uttar Pradesh, India, 1 of the most affected areas of the country. Reference Kumar, Vimal and Dimri12 It is a secondary care hospital with 200 beds and around 21 well-trained doctors and around 42 staff nurses. During the pandemic all hospital beds were dedicated to patients with COVID-19, with the number of medical staff increased to around 30 doctors and 64 staff nurses. At the time of our arrival, approximately 80 beds were occupied in 8 wards, located in a dedicated area of the structure, without any particular differentiation for intensity of care and/or severity of disease, due to the sudden overwhelming demand for oxygen beds. The emergency department had been closed, and patients were mainly hospitalized by referral by means of a network comprising the ITBP headquarters, Greater Noida hospitals, as well as police and hospital staff’s families and relatives. All other ordinary surgical and medical services had been suspended, as all staff (including specialists) were reallocated to care for patients with COVID-19. The radiology department was also wholly assigned to the care of patients with COVID-19, with the provision of X-ray imaging and an ultrasound system. No CT scanner was available. Intensive care unit (ICU) beds, normally located near the operating theater, were available but not active due to the lack of staff and shortages of oxygen. The hospital was running with a limited capacity of approximately 300 L/min of oxygen (18,000 L/h) and relying on a bulk cylinder system. Every hour, approximately four 46.7-L capacity cylinders were substituted by an officer assigned to that sole task. That translates to the need to substitute a cylinder weighing around 60 kg every 20 min, day and night, to ensure that a pressure of around 2 bar was reaching all patients. It was calculated that every patient would have a maximum 3 L/min at their disposal. Discussing the situation within mixed medical teams, it was highlighted that the devices providing oxygen to patients were mainly non–rebreathable-masks (NRM), oxygen delivery masks, and domiciliary B-PAP devices (ResMed™; n = 25 units). According to manufacturing standards, NRMs need between 10 and 12 L/min to maintain efficacy and reliability. On the other hand, for domiciliary B-PAP, with which an accurate FiO2 cannot be set, resulting performance can be unpredictable. Oxygen concentrators (approximately n = 10 units), to which it was possible to connect masks, were available in the wards, each providing a maximum of around 10 L/min. Oxygen provisions were scarce and cylinders were increasingly costly and hard to obtain.
Intervention
Step 1: Introduction of the Oxygen Generator to Improve the Oxygen Delivery Capacity
The main goal of our mission was to increase the total availability of oxygen from the oxygen source at the ITBP Referral Hospital. In light of previous experiences, Reference Sacchetto, Raviolo and Beltrando11 the decision was made to install a Pressure Swing Adsorption (PSA) oxygen plant system (Oxygen 93 % European Pharmacopoeia 04/2011:2455) instead of relying on a cylinder or tank system. The PSA system provides a central source of oxygen generation using PSA technology (similar to concentrators) allowing the provision of 61.8 m3/h of oxygen 95% ± 1% with a pressure of 5 bar. Its main parts are shown in Figure 1 and Figure 2, and include:

Figure 1. The PSA Oxygen Plant.

Figure 2. Pictures from the field. The PSA Oxygen plant installed.
Compressor GA75 VSD+ (3-phase 400V 50 Hz); Dryer 1175 m3/h and filtration system (0.1 and 0.01 micron); Coal tower 150 and micofine filter (0.01 micron); Air tank 2000 liters; Oxygen tank 2000 liters, filter 0.01 micron and bactericidal filter; and Line reducer.
The system needs a continuous power supply of 80 kW with a starting power of approximately 200 kW. Transportation of the disassembled system (total weight, 6052 kg) was coordinated by the Italian Civil Protection Department along with the EMT-2 and was achieved thanks to the Italian Air Force C-130. After identification of an adequate site at ITBP referral hospital, the system was mounted in 36 h into a space of around 25 m2. Technical and back-up tests were performed, a protective wall built, and an air conditioning system provided to maintain a steady temperature state below 25°C, as heat and humidity can affect the engine’s performance. A backup generator was also installed to assure the continuity of the system in case of electrical black-outs. The PSA oxygen plant was then connected to both the existing oxygen pipeline and the control unit at the hospital. The previous cylinder system (24 units) remained connected to the control unit as an automated pressure-regulated back-up solution in case of overflow. The pressure in the system was measured and noted (Table 1). After installation, flow meters were checked 1 by 1 to assess reliability and current usage. The pressure in the pipelines was measured on each of the wards to determine if there were any intervening leakages. Technical training about alarms and actions to put in place in case of overflow, as well as maintenance and proper use was provided both to local engineers and to dedicated staff.
Table 1. Hospital oxygen system characteristics before and after intervention

Step 2: On-Site Needs Assessment
Due to the short time available, a “go & see” approach was used. Medical and nursing teams were deployed to clinical ward rounds accompanied by local staff. Areas of interest in which interventions could potentially provide improvement in management were identified. The main areas that were targeted were clinical management (ventilation, diagnostic support, nursing, medical therapy) and organization. During ward rounds, it was noticed that early treatment was avoided due to the lack of resources (mainly oxygen delivery). Patients with SaO2 < 90-92% were admitted and ventilation was provided with a 2-step approach. When SaO2 levels were below 90%, NRM was the first line of treatment. With worsening respiratory distress, B-PAP was escalated. B-PAP machines were set with an inspiratory pressure of approximately 10-12 cmH2O (IPAP) and expiratory pressure of 5 cmH2O (EPAP). All B-PAP machines were home-treatment ventilators. To ensure high flow oxygen was given to critically ill patients, the only solution was to use a second oxygen source in a very unconventional way. We also noticed that no particular differentiation in device use was applied according to the level of respiratory failure: NRMs were being used mostly for mild and moderate cases, and nasal cannula was not used. Reference Graham, Bagayana and Bakare13 There was no targeted strategy of nutrition for patients with moderate and severe respiratory failure, and most of them were on peripheral parenteral nutrition. One aspect of standard treatment, remdesivir prescription, was observed for most of the admitted patients, with no differentiation made between early and late COVID-19 disease. Chest X-rays were the most used examination for diagnosis and monitoring, while no lung ultrasound (US) or ABG (arterial blood gas) exams were performed. As for the organizational side, due to scarcity of staff, there was only 1 medical doctor for nearly 90 patients in each of the 3 shifts per day. There were 5 nurses on each shift, 1 in each ward aided by 3 paramedical staff. As far as we noticed, nurses were mainly on duty for administering therapy and for patient care. No intensity of care model was used to allocate patients to different areas of the hospital, so patients on B-PAP were scattered around different wards. In the following days, a further “go & see” was required as the PSA oxygen plant was subject to several overflows due to its threshold of 1000 L/min being exceeded, mainly during night-shifts.
Step 3: Further On-Site Actions
Following the needs assessment, the following actions were implemented:
-
Brief medical training with a plenary session accessible to all medical staff, attended by the vast majority, apart from those on duty.
-
Ultrasound Session: a focused lung US (L-US) session was provided by 1 certified instructor. The main objectives of the session were the identification of the general characteristics of artifacts in L-US, as well as patterns, classification, progression, prognostic factors, concordance with other imaging and differentials in COVID-19-related pneumonia. Reference Smargiassi, Soldati and Borghetti14 On-site practical training was available. Following on from these sessions, bed-side exams were performed during clinical rounds.
-
Respiratory Failure Session: a focused respiratory failure session was provided by 2 MD specialists. The main subjects of the session were general principles, respiratory support (introducing the role of Helmet-CPAP or other devices able to provide PEEP such as Boussignac and Easyvent), devices for oxygen delivery, the role of pronation, and the rational use of oxygen flow. An on-site practical training and demonstration session was available. In line with our experience, the importance of early C-PAP treatment in moderate to severe hypoxemia was stressed. Reference Bellani, Grasselli and Cecconi15,Reference Coppadoro, Benini and Fruscio16
-
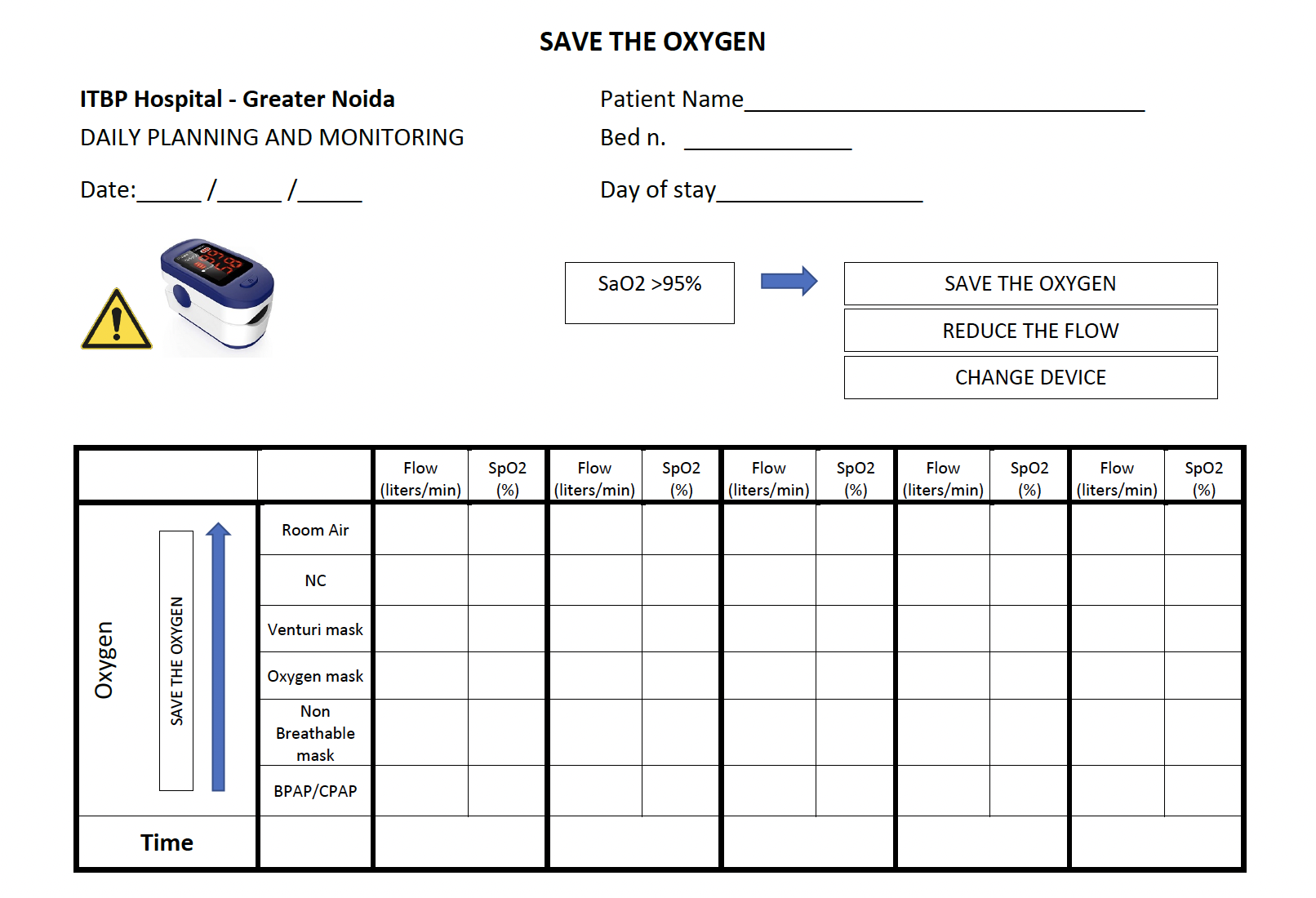
Proposal for organizational changes: a diagram to better allocate patients to dedicated areas providing varying intensity of care was proposed (Figure 3). A color code was also suggested to easily define patients’ clinical profile to improve the proper use of devices and rational use of oxygen. Nasal cannulae and Venturi masks were also introduced. As per our experience, we proposed that the role of the nurses should be broadened, giving them the task of monitoring O2 saturation and O2 flow at least once per shift using a specific form. Another main point was on how to assist for awake pronation. To prevent oxygen plant overflow above its maximum capacity, we proposed that the hospital management and medical doctors calculate the exact number of patients treatable with different types of respiratory support according to the maximum capacity of the system (Figure 4).
-
Medical Treatment Session: a focused medical treatment session was provided by 2 MD specialists. The main focuses of the session were the role of antivirals, antibiotics, immuno-modulants (especially corticosteroids) and anticoagulants and their timing during the course of the disease according to international protocols and guidelines. 17 The absence of evidence in the use of remdesivir in this setting was also discussed (Figure 5).

Figure 3. Patients’ stratification proposal according to respiratory failure during COVID-19 pandemic.

Figure 4. Different devices combination according to oxygen delivering capacity.

Figure 5. Pictures from the field. Medical therapy open session.
Short-Term Achievements
As well as achieving the main objective of our mission by increasing the oxygen availability from the hospital oxygen pipeline system from 300 L/min at 2 bar to 1000 L/min at 5 bar, the following short-term achievements were reported before the end of the mission:
-
Implementation of daily morning monitoring of the number of patients on O2 treatment, categorized by type of respiratory support;
-
The opening of an 8-bed High Dependency Unit (HDU) with a dedicated nurse and 2 paramedical staff in an already existing area with ICU ventilators and monitors, made possible due to improved oxygen supply;
-
The introduction of targeted oxygen therapy to achieve SaO2 ≤ 95%, to conserve the precious oxygen resource;
-
The introduction of the use of double flow fluxmeters adapting the European-manufactured connection and coupling pipes to the Indian wall entry junction, to ensure the high flow needed for Helmet-C-PAP and Easyvent mask with Ventukit. The switch from B-PAP to C-PAP, starting with Helmet and Easyvent was advised for selected patients. Optimizing oxygen use by adapting levels of assistance to changes in demand avoided the risk of overflow and hence the risk of being left with only the support of the back-up system and the breakdown of the machines. Working at nursing and ventilation support level led to the result that no more overflow was noticed in the following weeks;
-
The introduction of enteral nutritional support by means of a straw through C-PAP helmets and B-PAP masks was established;
-
The importance of pronation and consequent ventilation-perfusion mismatch was emphasized.
Additional Equipment Provided
The first cargo transported 20 ventilators, 1 stretcher for high-level (IV) biohazard containment, and a large amount of personal protective equipment (PPE), as well as the PSA machine along with the team. A second cargo added 2 more ultrasound machines (GE-Healthcare™), 2 ventilators (Siare Engineering™), 30 oxygen concentrators, and additional PPE.
Discussion
The main target of our mission, especially in the above-mentioned situation involving oxygen supply and delivery in India, was to guarantee a larger gas reserve in the ITBP Hospital and to free the structure from the inflated oxygen market using an autonomous oxygen source, as well as to promote the conservation and rationalization of its use. Reference Changoiwala1–5
Oxygen availability from the hospital oxygen pipeline system increased from 300 L/min at 2 bar to 1000 L/min at 5 bar. The previous cylinder system remained as a back-up solution as it was not possible to add the corresponding oxygen capacity to that of the PSA oxygen plant. Moreover, adding the cylinder system in parallel would have required a temporary but complete interruption of the total oxygen provision, a situation that was not feasible while all the inpatients were admitted. Time is an essential factor during an emergency, so 1 of the main successes of our intervention was in the extremely fast installation of the machine (around 36 h), which reduced delay in the treatment of patients. This was also made possible thanks to the incredible cooperation of the local staff. Of interest, overflow was noticed in the first days after installation of the new oxygen system, especially during night-shifts, maybe reflecting the stressful situations to which health-care workers were exposed at these times. Reference Watson, Saggar and MacDowell18 Intriguing technical issues included the differences in fluxmeter junctions (fixed by a lathe turner), the education of technicians and, occasionally, the language barrier. Also, the practical and factual approach to the ground situation, deploying both the medical and nursing staff with the “go & see” approach, contributed substantially to the subsequent steps. Very frequent briefings were scheduled with managers and engineers to assure the sustainability and maintenance of the donated equipment.
Equally, medical meetings gave everyone the opportunity to discuss the pathophysiology of COVID-19 to better tailor therapies. 17 These moments were a unique double opportunity to share medical knowledge and approaches to this much-debated disease and to provide additional tools such as US scans and oxygenation devices in the harsh fight against death. Reference Smargiassi, Soldati and Borghetti14–Reference Mantena, Rogo and Burke19 Additionally, sharing feelings and emotions in this hard time certainly enhanced empathy and team-building. Contact is maintained with the hospital officers and medics in India so that additional medical and maintenance issues can be addressed. In particular, ensuring that the provided equipment is still working at high capacity and no technical issues or system’s upkeep problems have emerged. Moreover, thanks to the opening of the HDU, patients are being treated according to the medical principles we shared during our briefings and that we continue to discuss by distance.
Short-term achievements were reached thanks to this strategy and should be considered as relevant. In fact, from a clinical point of view and especially in the management of COVID-19, adapting the nursing role to include supportive interventions and revising therapies are some of the main low-cost and high-output measures to put in place to reach a more systematic approach to patients. Also, assessing different levels of dependency and support can be crucial in improving the overall management of patients and arranging wards and areas accordingly to maximize resources and avoid misidentification of alarming symptoms.
The stability of the oxygen system and the adaptability of different devices to different levels of oxygen demand can also be key in the ever-changing picture of complex COVID-19 disease. Finally, feeding and fluid balance remain essential in the management of patients for both preserving physiological functions and metabolism Reference Lippi, South and Henry20 ; in conditions where heat, humidity, and ventilation may vary dramatically, accompanied with hard-to-manage stressors, this proved to be of great importance.
Our achievements prove the feasibility of a targeted intervention focusing on oxygen demand during a human disaster through collaboration and coordination with an integrated approach that considers logistics, materials, and assistance at all levels. In the literature, despite ongoing projects, Reference Murthy and Adhikari21–Reference Duke, Hwaihwanje and Kaupa23 there are no examples of such a successful intervention, and this is the first action of its kind that has been attempted and successfully carried out by an EMT WHO classified team.
The limitations of our intervention include the lack of a large dataset providing quantitative data on the intervention, both in the assessment of the baseline situation and in monitoring the outcomes. This can also be considered inherent in the EMT WHO approach to human catastrophe when a required action is extremely time-critical, preparedness crucial, and statistical data analysts could not be recruited. Also, despite our main goal being reached in a short period of time, the mission was too short to allow deeper and long-lasting cooperation and training, something telemedicine and online meetings can only partially remedy. In particular, nurses’ engagement was difficult, maybe due to their work overload and their different professional profile compared with the Italian model. Employment of easy-to-use and informative parameter records was attempted (Supplementary Material 1). Another important factor to consider is the limitation due to the continuous task shifting at a time of extreme resource shortage, which did not allow for a continuous, round-table, open discussion framework, apart from the few open sessions provided and largely attended in the first days.
Perspectives, Take Home Messages, and Conclusions
The installation of a PSA oxygen plant provided the ITBP Referral Hospital with a sustainable solution to oxygen shortage. In particular, thanks to the constant on-site generation of oxygen, patients were no longer the victims of possible disruption in the supply chain. For the future and in other settings, we should keep in mind this kind of system in the planning process when addressing oxygen shortage. The biggest challenge was the transportation of the disassembled oxygen plant, although the installation did proceed smoothly and proved feasible in less than 2 d, thanks to the presence of experienced technical staff and the huge effort from local workers following a coordinated plan. Freeing the oxygen source from an ever-changing political, economic, and social situation and relieving staff from taking decisions about the best supportive treatment during an almost unmanageable COVID-19 wave really changed the picture of the intervention site and gave not only confidence about the possibility of wider access to care but also hope to admitted patients. Reference Changoiwala1–Reference Madaan, Paul and Guleria10
The supply of oxygen could not be deemed a successful intervention without proper organization behind it to guarantee the rational use of the source. An innovative technological solution should not be a stand-alone intervention, but has to be integrated into a wider organizational approach. Reference Sacchetto, Raviolo and Beltrando11,Reference Graham, Bagayana and Bakare13–17 Having shared a similar scarcity of resources during different waves of this pandemic, an empathic atmosphere and receptive attitude from the medical staff and hospital managers was established that enabled us to share experiences, protocols and potential solutions to common problems that we also suffered in Italy during the first COVID-19 wave. In a scenario of disparity between needs and resources, international cooperation and solidarity can play a huge role. Reference Shadmi, Chen and Dourado24 The introduction of technological innovations could help in finding simple, sustainable, and feasible solutions in limited-resource settings. More traditional medical and public health principles are complementary to these solutions and should always be kept in mind when approaching human disasters. Last, mankind should thank the COVID-19 disaster in having emphasized the importance of team camaraderie, pro-activeness, and resource conservation. It would be pertinent to mention that all organizations and governments across the world will be forced to strengthen their delivery of health care and their administration in tackling any pandemic. Reference Padma7,Reference Murthy and Adhikari21–Reference Shadmi, Chen and Dourado24
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/dmp.2021.372
Acknowledgment
We thank the local medical, nursing, engineering, and technical staff. We also thank Michael Flinders and Roma Virhia for their valuable help.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by S.G., M.C., and C.F. The first draft of the manuscript was written by G.S. and all authors commented on previous versions of the manuscript. The table and figures were prepared by M.C., C.F. and G.S. All authors read, reviewed, and approved the final manuscript. All listed authors have approved the manuscript before submission, including the names and order of authors.
Conflict(s) of interest
The authors declare that they have no competing interests.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.