



Consider the case of a student referred to a school psychologist with the following presenting symptoms: decline in school motivation and performance, irritability and disruptive behaviour, attention and concentration difficulties, tiredness or lethargy, withdrawal from peers, and signs of poor school attendance. Such symptoms could be indicative of a range of difficulties and most school psychologists might want to consider a mood disorder, substance use, attention deficit hyperactivity disorder (ADHD), a disruptive behaviour disorder, family or peer dysfunction, or executive functioning difficulties. By virtue of how infrequent it is in school populations, few school psychologists would be drawn to consider a diagnosis of narcolepsy for this set of presenting symptoms. And yet, students with narcolepsy will experience a broad range of academic, social and emotional challenges that, if not adequately addressed, will become highly debilitating for the student. Moreover, without proper identification, treatment and school adjustment, these students will be highly frustrating and difficult for schools — and parents — to manage. It is somewhat surprising, then, that narcolepsy has received almost no attention in the peer-reviewed school psychology literature. The purpose of this article is to provide a concise overview of narcolepsy for school psychologists. It will first provide an overview of the presenting symptoms, prevalence, and process of diagnosis. This is followed by an outline of treatment approaches to narcolepsy. Finally, it will consider school management of students with narcolepsy and the specific role of the school psychologist.
Diagnostic Features and Criteria
Narcolepsy is a chronic neurological disorder that affects the regulation of sleep-wake cycles. It is characterised by excessive daytime sleepiness (EDS) that occurs regardless of the quality and amount of nocturnal sleep (American Academy of Sleep Medicine, 2014; Plazzi et al., Reference Plazzi, Clawges and Owens2018). This sleepiness can occur throughout the day at inappropriate times, such as when in public, at work or school, when socialising or eating, and is more likely within boring and sedentary environments. In addition to EDS, narcolepsy is often accompanied by disrupted night-time sleep, such as frequent nightly waking, difficulty returning to sleep, and poor sleep quality (Roth et al., Reference Roth, Dauvilliers, Mignot, Montplaisir, Paul, Swick and Zee2013). Also frequently associated with narcolepsy is cataplexy, characterised by the sudden and involuntary loss of muscle tone during wakefulness, typically triggered by strong positive emotions. During episodes of cataplexy, falling is a common occurrence, with knees, head and jaw the frequently compromised body parts (Serra et al., Reference Serra, Montagna, Mignot, Lugaresi and Plazzi2008).
The American Academy of Sleep Medicine’s International Classification of Sleep Disorders, Third Edition (ICSD-3) classifies narcolepsy into two separate types, whereby narcolepsy type 1 is used to refer to people who experience cataplexy while narcolepsy type 2 is used in the absence of cataplexy (American Academy of Sleep Medicine, 2014).
Narcolepsy is usually diagnosed by a specialist sleep physician based on a clinical history of typical episodes and symptoms that are not explained by other causes, such as obstructive sleep apnoea, other sleep disorders, or depression. Additional objective tests that aid in the confirmation of a narcolepsy diagnosis include the measurement of hypocretin levels and both night and daytime polysomnographic (PSG) tests. A Multiple Sleep Latency Test (MSLT) is generally conducted to establish daytime sleepiness and measures how quickly a patient falls asleep during the daytime in a quiet environment over a number of trials. A combination of clinical history and these objective measures are required for accurate diagnosis.
Notably, diagnosis in childhood can be particularly difficult due to differential symptom presentation in comparison to narcolepsy in adulthood (Plazzi et al., Reference Plazzi, Clawges and Owens2018; Quaedackers et al., Reference Quaedackers, van Gilst, van Mierlo, Lammers, Dhondt, Amesz, Peeters, Hendriks, Vandenbussche, Pillen and Overeem2018). The constellation of less understood narcolepsy symptoms, including cataplexy, hypnogogic hallucinations and sleep paralysis, can lead the disorder to be misdiagnosed as other psychological difficulties (including depression, panic attacks, night terrors, dissociation, and psychotic symptoms) or other neurological disorders such as epilepsy, Klein-Levine Syndrome, syncope or neuromuscular diseases (Coelho et al., Reference Coelho, Aloe, Moreira, Sander, Roitman, Prado, Pradella-Hallinan, Fernandes and Alves2012; Stores, Reference Stores2006).
The significant variability in symptomatology — both between individuals and particularly when considering childhood versus adulthood presentation — often leads to delayed or misdiagnosis (Morse & Sanjeev, Reference Morse and Sanjeev2018; Pizza et al., Reference Pizza, Franceschini, Peltola, Vandi, Finotti, Ingravallo, Nobili, Bruni, Lin, Edwards, Partinen, Dauvilliers, Mignot, Bhatia and Plazzi2013). Whereas the presence of cataplexy makes diagnosis of type 1 narcolepsy comparatively more obvious, diagnosing type 2 narcolepsy is particularly challenging (Baumann et al., Reference Baumann, Mignot, Lammers, Overeem, Arnulf, Rye, Dauvilliers, Honda, Owens, Plazzi and Scammell2014). Subsequently, it is not uncommon for there to be a substantial gap between initial onset to diagnosis, with estimated mean delay of first diagnosis as much as 15 years (Thorpy & Krieger, Reference Thorpy and Krieger2014).
School psychologists have a particular challenge of differentiating the signs of narcolepsy in a student from those difficulties that present more frequently within schools. The most likely ‘suspects’ are daytime sleepiness stemming from insufficient nocturnal sleep (e.g., due to gaming, social media, or studying late into the night); lethargy and cognitive inefficiency due to depression; or inattention or other behavioural problems related to ADHD. Careful history taking, coupled with the use of standardised measures and/or a sleep diary will help the school psychologist tease out the likelihood of narcolepsy (or indeed other hypersomnias) from other differential diagnoses.
Prevalence and Course of Illness
Narcolepsy is a chronic, lifelong condition, which, if left undiagnosed or without adequate treatment and support, is likely to significantly impact on a person’s cognitive, academic, social and psychological functioning and result in an overall reduction in their reported quality of life (Babiker & Prasad, Reference Babiker and Prasad2015; Raggi et al., Reference Raggi, Plazzi and Ferri2019). It is estimated to affect approximately .025–.05% of the population in Western countries, with higher rates estimated in some Asian countries, possibly accounted for by a specific genetic susceptibility or methodological differences across studies. First symptoms can occur anywhere between early childhood and adulthood. In the most definitive study of the age of onset, Dauvilliers and colleagues found a bimodal distribution of onset, with one peak occurring at 14.7 years and a second at 35 years (Dauvilliers et al., Reference Dauvilliers, Montplaisir, Molinari, Carlander, Ondze, Besset and Billiard2001). Importantly, they report that those diagnosed at the younger peak were more likely to have a family history of narcolepsy and that younger age of onset was associated with more severe symptoms. Narcolepsy is evident in both males and females, with suggestions that it is slightly more common in males (Longstreth et al., Reference Longstreth, Koepsell, Ton, Hendrickson and van Belle2007).
Narcolepsy in children has some well-described psychiatric comorbidities, primarily ADHD, depression, anxiety (in particular, generalised anxiety disorder), oppositional defiant disorder, and eating disorders (Morse & Sanjeev, Reference Morse and Sanjeev2018; Szakács et al., Reference Szakács, Hallböök, Tideman, Darin and Wentz2015). Common physical comorbidities in children include obesity and precocious puberty, and in some rare cases, progression may also include deafness, dementia and ataxia later in life (Kotagal et al., Reference Kotagal, Krahn and Slocumb2004; Moghadam et al., Reference Moghadam, Pizza, La Morgia, Franceschini, Tonon, Lodi, Barboni, Seri, Ferrari, Liguori, Donadio, Parchi, Cornelio, Inzitari, Mignarri, Capocchi, Dotti, Winkelmann, Lin and Plazzi2014; Poli et al., Reference Poli, Pizza, Mignot, Ferri, Pagotto, Taheri, Finotti, Bernardi, Pirazzoli, Cicognani, Balsamo, Nobili, Bruni and Plazzi2013; Winkelmann et al., Reference Winkelmann, Lin, Schormair, Kornum, Faraco, Plazzi, Melberg, Cornelio, Urban, Pizza, Poli, Grubert, Wieland, Graf, Hallmayer, Strom and Mignot2012). Thus, without adequate diagnosis and support, narcolepsy and its common psychiatric and physical comorbidities can be extremely debilitating and significantly interfere with a person’s functioning.
Causes of Narcolepsy
The causes of narcolepsy are not well understood but appear to stem from an interaction of genetic, biochemical and environmental factors. Those with a first-degree relative with narcolepsy are 20–40 times more likely to develop the disorder than the general population, but they still only have a 1–2% risk of this (Taheri, Reference Taheri, Goswami, Thorpy and Pandi-Perumal2016). Moreover, although type 1 and type 2 narcolepsy may appear phenotypically similar, they have differing underlying causes. The causes of narcolepsy type 1 are better understood, with a loss of neurons in the hypothalamus region leading to low levels of the neuropeptides hypocretin-1 and hypocretin-2 (also known as orexin-A and -B), which play a significant role in REM sleep regulation and wakefulness. Low levels of hypocretin appear to often be linked to abnormalities in the immune system, which may be due to a combination of genetic and environmental factors. By contrast, hypocretin levels are often normal in cases of narcolepsy type 2. Research supports an association between narcolepsy and certain environmental factors, with particular interest in infections and vaccinations (Kornum, Reference Kornum, Goswami, Thorpy and Pandi-Perumal2016). In relation to infections, epidemiological studies have implicated upper airway infections, particularly streptococcal, with narcolepsy vulnerability. Interest in the relationship between narcolepsy and vaccinations was highlighted following an increase in the incidence of narcolepsy in six European countries after the H1N1 influenza (swine flu) pandemic and Pandemrix H1N1 vaccination campaign of 2009–2010 (Sarkanen et al., Reference Sarkanen, Alakuijala, Dauvilliers and Partinen2018). Similar correlations between narcolepsy rates and H1N1 exposure were also found in the UK and Asia (Han et al., Reference Han, Lin, Warby, Faraco, Li, Dong, An, Zhao, Wang, Li, Yan, Gao, Yuan, Strohl and Mignot2011; Stowe et al., Reference Stowe, Andrews, Kosky, Dennis, Eriksson, Hall, Leschziner, Reading, Shneerson, Donegan and Miller2016). These studies provide strong evidence for an association between H1N1, hypocretin deficiency and subsequent narcolepsy.
Cognitive Functioning of Young People With Narcolepsy
Several studies alert us to compromised cognitive functioning in young people with narcolepsy. Overall, IQ does not appear to be affected by narcolepsy (Posar et al., Reference Posar, Pizza, Parmeggiani and Plazzi2014; Thieux et al., Reference Thieux, Zhang, Marcastel, Herbillon, Guignard-Perret, Seugnet, Lin, Guyon, Plancoulaine and Franco2020). However, young people with narcolepsy can show diverse cognitive profiles (Dorris et al., Reference Dorris, Zuberi, Scott, Moffat and McArthur2008), with verbal comprehension and working memory being specifically implicated (Szakács et al., Reference Szakács, Hallböök, Tideman, Darin and Wentz2015). Neumann and colleagues (2006) identified executive functioning deficits in young people with narcolepsy that they attributed to a reduction in cognitive resources due to these students needing to reallocate resources for vigilance and monitoring. Excessive daytime sleepiness will leave students tired in class, which can also have a significant impact on mood and motivation for learning (Karjalainen et al., Reference Karjalainen, Nyrhilä, Määttä and Uusiautti2014).
Social, Emotional and Behavioural Functioning of Young People With Narcolepsy
A considerable degree of research has investigated the social, emotional and behavioural difficulties associated with narcolepsy. Although the number of participants in these studies has been understandably modest, a very clear picture has emerged of significantly greater social-emotional difficulties in these children and adolescents. Elevated levels of externalising behaviours, including rule breaking and aggression, has been reported in a cohort of children with narcolepsy (Dorris et al., Reference Dorris, Zuberi, Scott, Moffat and McArthur2008; Shelton & Malow, Reference Shelton and Malow2017). Likewise, children with narcolepsy are more likely to experience depression and internalising disorders (Dorris et al., Reference Dorris, Zuberi, Scott, Moffat and McArthur2008; Inocente et al., Reference Inocente, Gustin, Lavault, Guignard-Perret, Raoux, Christol, Gerard, Dauvilliers, Reimao, Bat-Pitault, Lin, Arnulf, Lecendraux and Franco2014). Children with narcolepsy are reported to feel awkward and embarrassed in social situations; different from, and at times victimised by their peers; experience low self-image; and to interpret their hallucinations as a terrifying sign that they are going crazy (Stores, Reference Stores, Goswami, Pandi-Perumal and Thorpy2010). Adolescents report specific social awkwardness, such as falling asleep at social gatherings, appearing to be under the influence of substances, and added complications with alcohol consumption, driving and judgments about sexual matters (Kavey, Reference Kavey1992; Stores, Reference Stores, Goswami, Pandi-Perumal and Thorpy2010). Overall, it is not surprising that the quality of life of these young people is rated lower than their healthy peers — both by their parents and the young people themselves (Avis et al., Reference Avis, Shen, Weaver and Schwebel2015). In light of this information, schools must make concerted and coordinated efforts to ensure a considered and comprehensive management plan.
Treatment
There is no cure for narcolepsy and currently available treatments only partially remit symptoms. Treatments can be considered within two categories — pharmacological treatments and behavioural and/or lifestyle strategies. There is no one treatment identified as the gold standard for narcolepsy management, and a combination of pharmacological and behavioural intervention is often recommended.
Pharmacological treatments focus on reducing the effects of the core symptoms of EDS and cataplexy, with separate medications used for each. A range of medications are used for EDS but on an empiric, off-label basis, including stimulant mediations (amphetamine and methylphenidate) and the wakefulness-promoting drugs modafinil and armodafinil. Similarly, various off-label medications are used for the treatment of cataplexy in children and adolescents, including tricyclic agents, selective serotonin reuptake inhibitors and selective norepinephrine reuptake inhibitors (Franceschini et al., Reference Franceschini, Pizza, Antelmi, Folli and Plazzi2020; Kotagal, Reference Kotagal2018). The only medication that can be used for the treatment of both EDS and cataplexy in children and adolescents is sodium oxybate (Xyrem). However, sodium oxybate is not approved in many countries and has restricted use in others due to the high risk of side effects, including sleep walking, nausea, sleep enuresis, exacerbation of sleep apnoea, tremor, constipation, and weight loss (Franceschini et al., Reference Franceschini, Pizza, Cavalli and Plazzi2021).
Compared to pharmacological therapies, there is comparatively little research on the efficacy of lifestyle and behavioural interventions for narcolepsy in children and young people. Consequently, much of what is described in the literature is derived from research and guidelines for adults. Bhattarai and Sumerall (Reference Bhattarai and Sumerall2017) provide a helpful summary of behavioural interventions into the following categories.
Patient education. This includes educating the young person on the symptoms of narcolepsy, the impact of these on relationships and school, the types of treatments available, and lifestyle factors that may affect symptom severity and/or treatment outcomes. For young people, including parents and siblings in such education is recommended.
Sleep hygiene. Good sleep hygiene includes optimising night-time sleep, consistent sleep-wake habits and scheduled brief daytime naps; avoiding alcohol, caffeine and tobacco in the hours before bedtime; creating an environment conducive to sleep; and manipulating body temperature.
Strategic napping. Scheduled daytime naps of 15–20 minutes, two to three times per day can be effective in treating EDS and improving alertness.
Self-report assessments. The use of self-report measures can aid clinicians in better understanding different aspects of a young person’s sleep routines, treatment effects and cognitive functioning. A broad range of self-report measures for narcolepsy are available (Krahn et al., Reference Krahn, Hershner, Loeding, Maski, Rifkin, Selim and Watson2015).
Manipulation of skin and body temperature. Warmer skin in proximal regions of the body and cooler skin in distal regions has been associated with increased wakefulness and alertness. Consequently, positive narcolepsy management can be promoted through thermoregulation, including choice of clothes, consuming warm drinks, and using fans to keep extremities cool.
Cognitive behaviour therapy (CBT). Research on CBT with people with narcolepsy — especially children and adolescents — is not well developed. However, three essential components of CBT for narcolepsy have been proposed: a behavioural component aimed at changing sleep-disordered behaviours; a cognitive component aimed at modifying beliefs, motivations and emotions that play a role in maintaining narcolepsy; and an educational component that informs the PWN about the nature of the disease and its treatment (Marín Agudelo et al., Reference Marín Agudelo, Jiménez Correa, Carlos Sierra, Pandi-Perumal and Schenck2014).
Psychosocial implications. As already stated, narcolepsy is associated with a range of other psychiatric, social and academic or vocational challenges. Effective ‘treatment’ involves careful assessment and management of these factors. The influence of such factors is particularly salient when considering school management of narcolepsy.
In addition to these aforementioned interventions, physical activity is one nonpharmacological intervention for childhood narcolepsy that displays promise, with evidence that it increases night-sleep duration and sleep quality while reducing nap frequency and subjective sleepiness (Filardi et al., Reference Filardi, Pizza, Antelmi, Pillastrini, Natale and Plazzi2018).
School Management of the Student With Narcolepsy
When a student is diagnosed with narcolepsy, the first step for a school is to meet with the student and family to understand the specific and individual nature of the student’s narcolepsy presentation. Key school staff to form a management team include the school psychologist, learning support teacher, school nurse, and wellbeing teacher. The school will need to know the extent of the daytime sleepiness; whether the student experiences cataplexy, and if so, what form it takes; whether the student requires the administration of any medications at school; and the presence and nature of any hallucinations. It is advisable that the school seeks formal consent to consult with the treating sleep specialist to better understand the student’s disorder and to enlist their support in the development of a school management plan.
From the initial school meeting with the student and family, a school management plan should be collaboratively agreed on and clearly communicated to all relevant school personnel, including classroom teachers and co-curricular staff (e.g., sports coaches). This plan should include specific details of how the student will manage daytime tiredness, inhibited class focus and motivation, and medication use. If a student experiences cataplexy or hallucinations, all school staff should be informed in the event of encountering the student during playground duty or in relief classes. Without an alternate explanation for a student’s apparent class disconnection (e.g., irritability, drowsiness, low motivation, poor application), many teachers may mistakenly develop a negative, incorrect and unhelpful formulation for the student’s behaviour, such as ‘he/she is lazy/naughty/disrespectful’. It is of the utmost importance, therefore, that all those who teach these students are given a comprehensive explanation of the nature of the disorder and how it presents in class. Students with a new diagnosis of narcolepsy will often have caused their teachers a good deal of frustration by their behaviour during the prediagnosis period. Armed with this knowledge of the diagnosis, and the collaboratively developed classroom strategies, class teachers will be empowered to manage the student with narcolepsy in a more beneficial way.
Classroom Management of the Student With Narcolepsy
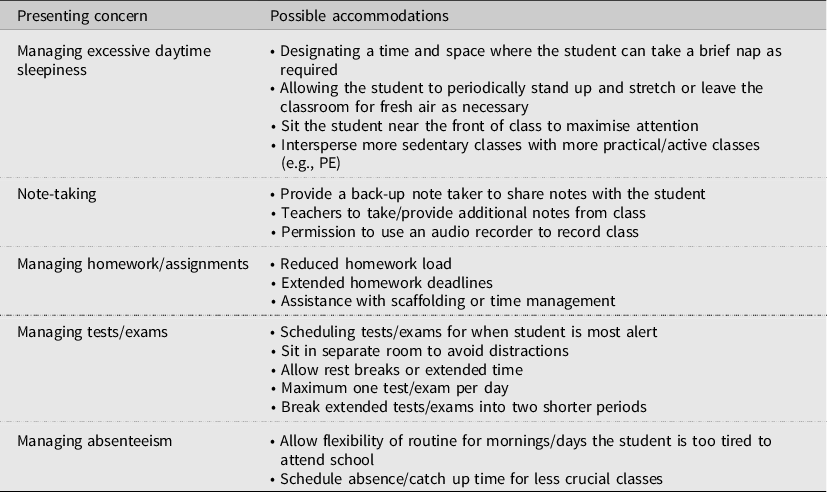
Schools should expect all students with narcolepsy to be at risk of academic complications arising from their disorder — ranging from mild to severe. That said, in most cases they can be taught within a mainstream classroom with suitable accommodations made. Karjalainen (Reference Karjalainen, Nyrhilä, Määttä and Uusiautti2014) notes that problems with concentration and work focus are most likely to occur when the student is working in a large group and suggests looking to engage the student in either small group work or individual instruction. Students with narcolepsy are likely to require a personalised learning plan that addresses their specific symptoms and educational challenges. The principles for developing personalised learning plans for a student with narcolepsy are no different to any student with a disability, and schools are usually excellent at devising these (Pierangelo & Giuliani, Reference Pierangelo and Giuliani2007). Table 1 summarises a range of suggestions for classroom accommodations for students with narcolepsy (Flygare, Reference Flygare, Goswami, Thorpy and Pandi-Perumal2016; Narcolepsy Network Inc., 2015).
Table 1. Classroom Accommodations for Students with Narcolepsy
Conclusion
Given its comparatively low prevalence rate, it is understandable that narcolepsy has not received substantial attention in the school psychology literature. Even in work that directly addresses sleep disorders in school students, narcolepsy receives not much more than a passing mention (e.g., Cain & Sakakini, Reference Cain, Sakakini, Thielking and Terjesen2017; Everhart, Reference Everhart2011). Nonetheless, narcolepsy presents significant social, emotional and academic challenges for a young person and consequently for those tasked with the challenge of educating them. It is highly concerning that in narcolepsy, like in many other disorders, the lag between the onset of first symptoms and diagnosis can be many years. Undiagnosed, a young person with narcolepsy may experience many years of academic underachievement, unintentional mismanagement by unaware teachers, poor self-esteem and impaired emotional functioning, and social exclusion and ridicule. It is within this context that an informed school psychologist is excellently placed to bring about vastly enhanced quality of life for the student with narcolepsy. We encourage all school psychologists to include a thorough appraisal of a student’s sleep as an integral part of their standard assessment. At the very least, this is warranted due to the close relationship between sleep and many emotional and behavioural problems (Zhang et al., Reference Zhang, Paksarian, Lamers, Hickie, He and Merikangas2017). However, our hope is that this article will also motivate school psychologists to consider the possibility of narcolepsy during their assessments and, where necessary, be better placed to guide the school in supporting and managing this impactful condition.

