


Since 1975, the worldwide prevalence of the condition of being overweight and that of obesity has increased threefold, reaching 39 and 13 %, respectively(1). An increase in the prevalence of obesity is associated with health conditions such as diabetes and dyslipidaemia(1). High prevalence of obesity is due to high consumption of high energy-dense foods (e.g. soft drinks with high-fructose corn syrup and high-fat foods) and low consumption of fruits and vegetables(Reference Delavari, Sønderlund and Swinburn2–Reference Drewnowski and Popkin4). In addition, lifestyle and dietary habits have changed since 1980(Reference Delavari, Sønderlund and Swinburn2–Reference Drewnowski and Popkin4). There has been a shift towards eating meals outside the home and in restaurants, which in turn has led to increases in the portion size of meals(Reference Delavari, Sønderlund and Swinburn2–Reference Drewnowski and Popkin4). Poor diet quality and dietary habits may be associated with poor nutritional knowledge(Reference Saeidlou, Babaei and Ayremlou5). Several studies have shown the influence of nutritional education in enhancing dietary knowledge and practice in terms of choices in food consumption among university students(Reference Abood, Black and Birnbaum6–Reference Ha, Caine-Bish and Holloman10). An 8-week nutritional education programme (eight educational sessions) was conducted among thirty female college students. The study reported significant improvement in nutrition knowledge scores by around 4 %(Reference Abood, Black and Birnbaum6). Other studies have found that the nutrition awareness programme has increased whole-grain, vegetable and dairy product intake and reduced soft-drink consumption(Reference Ha and Caine-Bish7–Reference Ha, Caine-Bish and Holloman10).
About 30 % of Saudi Arabians suffer from obesity(Reference M Alqarni11). This may be related to poor diet quality among Saudis. The Saudi health interview survey revealed high consumption of sugar-sweetened beverages among Saudis aged between 15 and 24 years. In addition, only around 5–7 % of Saudis met the recommendations for consumption of fruits, vegetables and sugar-sweetened beverages(Reference Moradi-Lakeh, El Bcheraoui and Afshin12). Therefore, effective intervention programmes are needed to reduce the obesity risk by increasing public nutritional knowledge and implementing national regulations to maintain healthier food options. Recent evidence showed that nutritional knowledge among adults and Saudi university residents was low(Reference Bakhotmah13–Reference Epuru and Al Shammary15). Moreover, effective and applicable intervention programmes are needed in universities to enhance nutritional knowledge and improve dietary practice, including food intake and diet quality. In 2019, the Saudi Food and Drug Authority launched regulations to include the energy content on restaurant menus with the objective of increasing the awareness about healthy food choices. It is hoped that it may help the consumers make better decisions regarding meal, food and beverage choices(16). Therefore, the objective of the current study is to assess the influence of the 2019 nutrition education and intervention programme on the nutrition knowledge and dietary practice among the Princess Nourah Bint Abdulrahman University students and staff.
Methodology
Study design and study subjects
A national initiative programme was established by the Saudi Food and Drug Authority in 2019 to improve health through food choices, and a survey was conducted at Princess Nourah Bint Abdulrahman University. The awareness programme, titled ‘Promoting Public Health through Healthy Food Choices in the Work Environment’, was focused on many aspects to increase overall health and nutritional awareness among the students and employees of Princess Nourah Bint Abdulrahman University. A pretest–posttest, non-randomised experimental study design was employed at Princess Nourah Bint Abdulrahman University in Riyadh City, the Kingdom of Saudi Arabia between September 2019 and February 2020. Princess Nourah Bint Abdulrahman University is the largest women’s university in the world and has eighteen colleges and institutions and around ninety academic programmes, hosting almost 39 000 female students and 2161 faculty members from twenty-five different nations. Participants of this study were studying or working with various faculties and offices of the university. Five colleges and corresponding institutes were identified: (1) humanities colleges – the College of Education, College of Arts, College of Social Work, College of Languages, College of Design and Arts and Community College; (2) science colleges – the College of Science, College of Computer and Information Sciences, College of Business Administration and College of Engineering; (3) health science colleges – the College of Nursing, College of Medicine, College of Dentistry, College of Health and Rehabilitation Sciences, College of Pharmacy and College of the Constitutive Year; (4) deanships and institutes – the Deanship of Community Service and Continuing Education faculty/staff, Institute for Teaching Arabic Language (students and faculty/staff) and English Language Institute and (5) administration facilities – the main administration, the central library and any other service facility not mentioned above.
The interventions conducted in this study were: (1) nutritional education to all the university staff and students and (2) policy implementation across the university.
Nutritional intervention
Nutrition education
The nutritional education programme, titled ‘Promote Public Health through Healthy Food Choices in the Work Environment’, was directed towards all Princess Nourah Bint Abdulrahman University staff, including students and employees, and focused on healthy food choices, particularly on low added sugar, salt, saturated fat and trans-fat. The programme consisted of in-campus nutrition education (total 48 h) at multiple locations across campus to cover all colleges. Additional nutritional messages were spread through (1) email (thirty-six messages), (2) television screens throughout the university (eighteen messages) and (3) social media (eighteen Twitter messages).
Policy implementation
The Princess Nourah Bint Abdulrahman University campus contains forty-two locations for food sales with fifteen food service companies and retailers. Several policy implementations were applied to support the initiative’s provisions by increasing healthier food options. The characteristics of ‘healthier food options’ are based on the WHO guidelines and include any product having 30 % or less of its kcal from fat, 10 % or less of kcal from saturated fat, 1 % or less of kcal from trans-fat, 10 % or less of kcal from added sugar or 400 mg or less of Na per serving(17). All food retailers on campus were requested to make several changes. Daily follow-up was conducted at all retail locations to ensure that the recommendations mentioned below were applied. The recommendations were: (1) not offering soft drinks as the only beverage option in the meal; (2) providing different fresh juices instead of drinks and nectar; (3) not adding sugar to fresh juices; (4) preventing misleading health and nutritional claims such as fat-burning juice, energy juice, fat-soluble juice, etc.; (5) providing products that do not contain added sugars or have little added sugar; (6) dispensing with artificial sweeteners and replacing them with natural sweeteners provided that they are available to the consumer; (7) replacing chocolate with granola, fruit, nuts and oats at accounting boxes; (8) providing low-salt (Na) products and using salt substitutes such as lemon, garlic, onion powder, spices and herbs; (9) preventing the use of palm oil and coconut oil during the cooking or frying process; (10) providing salads with lemon and olive oil instead of salad dressing or providing dressing separately from the salad and showing the dressing’s kcal value; (11) providing low-fat and skim dairy products; (12) providing prepared nutritional options using healthy cooking methods (broiling, boiling, steam cooking); (13) providing different sizes of meals, especially small meals, for those interested in reducing the size of the food portion and (14) providing high-fibre options such as whole grains (e.g. whole-grain bread, using whole-grain flour in preparing cakes and other bakery products, etc.).
Data collection tool
Questionnaires were distributed both before and after the awareness programme to assess participant knowledge and practices regarding food and health. Of the total questionnaires, 2670 (44 %) were emailed to participants and 1970 (55·4 %) were administered through face-to-face interviews. The questionnaire was administered to the Princess Nourah Bint Abdulrahman University staff, faculty and students between September and October 2019 (before the awareness programme) and between March and April 2020 (after the awareness programme). The pretest and posttest were conducted with independent samples.
The questionnaire was adapted from a previous nationwide survey titled ‘National Survey of Health, Diet, Physical Activity and Supplements among Adults in Saudi Arabia’, which was conducted by the Saudi Food and Drug Authority(Reference Nora, Althumiri and Rasha18). Additional questions were included from another awareness nutritional programme in Arabic conducted in Jordan(Reference Alnader19). The questionnaire used in the current study comprised three sections: (1) three demographic questions concerning a participant’s status (student or employee), department (e.g. faculty, library, etc.) and presence of any chronic disease (e.g. diabetes mellitus, anaemia, hypertension, hypo- or hyperthyroidism, food allergies, celiac disease, etc.); (2) fifteen dietary knowledge questions (entailing the concept of food variety and nutrients, fast food and its poor nutritional value, and the influence of cooking style on the nutritional quality of food), with three possible answers for each: ‘agree’, ‘disagree’ and ‘not sure’ and (3) twenty-three questions on dietary practices regarding choices in food consumption (entailing eating breakfast; consuming salt/sugar; eating high-salt food; eating pre-packaged food; and consumption of vegetables, fruits, supplements, water and caffeine). The possible answers for questions pertaining to practice were ‘yes’, ‘no’ and ‘sometimes’. Each correct response was awarded one point; the highest possible knowledge score was 15, and the highest possible practice score was 23. The study tested whether the effect of the intervention differed according to the health status of the participants, depending upon the participant having no disease, one disease or two or more diseases. Consent for participation was taken from the participants before responding to the survey.
Statistical analysis
Since the participants of the pretest were different from those of the posttest, independent t tests were conducted to determine whether the intervention had an effect on knowledge and practice. Assuming that knowledge and practice scores would be higher after the intervention, a one-tailed P-value of 0·05 was specified for both procedures. Two-by-two ANOVA was conducted to determine whether the effect of the intervention differed between students and employees. Finally, a Pearson correlation was conducted to determine the relationship between knowledge scores and practice scores, assuming a positive relationship between the two scores.
Results
Descriptive statistics for the study population
The survey was completed by 1824 respondents before the intervention (1350 students and 474 staff/faculty) and by a different cohort of 1731 respondents after the intervention (1317 students and 414 staff/faculty). The total number of participants was 3555 staff and students. The majority of the sample consisted of students (75·1 %), and the majority of participants, whether student or staff, had not been diagnosed with any disease (73·7 %). Approximately half (51·3 %) took the knowledge and practice tests before the intervention and were studying/working in the College of Humanities and the Community College (52·9 %) (Table 1).
Table 1 Frequencies and percentages for the variables describing the sample (n 3555)

Nutrition knowledge and practice
Table 2 shows the average knowledge and practice scores. The highest possible knowledge score was 15, and the mean score of 8·55 (sd = 2·71) was slightly above the average of possible scores. The average number of correct answers by all participants in this study was around 56 %. The highest possible score was 23, and the mean practice score was relatively low at 9·33 (sd = 3·98). The findings presented in Table 2 reveal that knowledge scores changed after the intervention, t(3550) = –3·90, P < 0·001, partial η 2 = 0·002. Knowledge scores were significantly higher after the intervention (M = 8·73, sd = 2·59) than before the intervention (M = 8·38, sd = 2·81). However, practice scores did not change significantly after the intervention, t(3526) = 0·52, P = 0·602, partial η 2 = 0·000.
Table 2 Means, standard deviations and independent t test results for knowledge and practice scores before and after the intervention (n 3555)

***P < 0·001.
The association between nutrition knowledge and practice and demographic characteristics
The findings in Tables 3 and 4 reveal that the effect of the intervention on knowledge scores differed significantly between students and employees F(1,3551) = 5·81, P = 0·016, partial η 2 = 0·002. As shown in Fig. 1a, the mean score for employees was about the same before and after the intervention; however, the mean score for students was higher after the intervention.
Table 3 Means and standard deviations for knowledge and practice scores before and after the intervention across students and employees (n 3555)

* P < 0·05.
Table 4 ANOVA results for knowledge and practice scores across students and employees (n 3555)
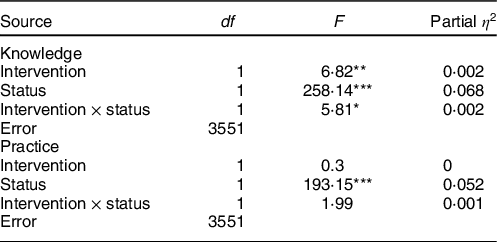
*P < 0·05; **P < 0·01; ***P < 0·001.

Fig. 1 Mean knowledge scores of (a) students (![]() ) and employees (
) and employees (![]() ) and (b) humanities (
) and (b) humanities (![]() ) and health (
) and health (![]() ) participants before and after the intervention.
) participants before and after the intervention.
The effect of the intervention on practice scores did not differ significantly across students and employees, F(1,3551) = 1·99, P = 0·158, partial η 2 = 0·001 (Table 4). Rather, regardless of the intervention, employees had higher practice scores (M = 10·76, sd = 4·22) than did students (M = 8·88, sd = 3·68) (Table 3).
The findings of the current study revealed that the effect of the intervention on the knowledge and practice scores did not differ according to the health status of the participants, F = 0·55, P = 0·576, F = 0·71, P = 0·493, respectively.
The study tested the effect of the intervention on the knowledge score across different colleges, F(4,3545) = 2·94, P = 0·019, partial η 2 = 0·002. The effect of the intervention differed only between the Humanities and Health colleges; as shown in Fig. 1b, although the mean knowledge score for those in the Health college remained almost the same after the intervention as before, the mean knowledge score for those in the Humanities college increased after the intervention.
The effect of the intervention on practice scores did not change significantly across colleges, F(4,3545) = 1·39, P = 0·236, partial η 2 = 0·002. Regardless of intervention, participants from the administrative colleges had significantly higher practice scores than those from other colleges (Table 5).
Table 5 ANOVA results for knowledge and practice scores across colleges (n 3555)
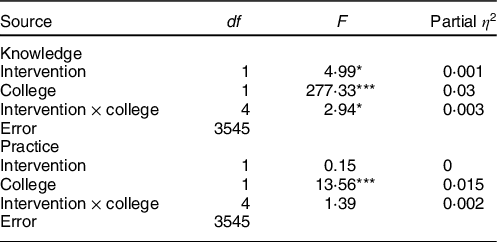
*P < 0·05; ***P < 0·001.
Finally, a Pearson correlation procedure was conducted to determine the relationship between knowledge and practice scores. The findings revealed that knowledge scores were positively correlated with practice scores, r = 0·28, P < 0·001.
Discussion
This study aimed to test the effect of a nutrition education and intervention programme on nutrition knowledge and dietary practice among the female staff and students at Princess Nourah Bint Abdulrahman University. The result of the current study showed that participants’ nutritional knowledge improved post the nutrition programme among students from the humanities and community colleges. Although no changes were found in the dietary practices pre- and posttest, employees had higher practice scores than did students.
The current study found that the average number of correct answers by all participants in this study was around 56 %. The study participants were able to answer general nutritional questions (>74 %) such as the concept of food variety and nutrients, fast food and its poor nutritional value, and the influence of cooking style on the nutritional quality of food. However, knowledge was low about nutrient content in food, such as grain products being rich sources of Fe, excessive consumption of fruits leading to obesity and the kcal content of protein v. fat. In addition, this study revealed that nutrition knowledge was higher in participants from medical colleges. This result was consistent with other studies among university students (medical and non-medical)(Reference Liu, Yang and Xu20,Reference Sajwani, Shoukat and Raza21) . The effect of the intervention on knowledge scores differed significantly across colleges. On investigating that effect across the Humanities, Sciences, Health, Administrative and Deanship faculty, it was found that the mean knowledge score for those in the Health colleges remained about the same before and after the intervention, while the mean knowledge score for those in the Humanities increased after the intervention.
The majority (75·1 %) of the participants in the current study were students. The results of the questions about dietary practices showed that the majority of the participants (>60 %) were skipping breakfast, adding salt or eating high-salt food such as pickles and pre-packaged food and were not eating vegetables and fruits daily. A study conducted in Saudi Arabia at Hail University found poor dietary practices among female students, including not eating breakfast or consuming too few vegetables and fruits daily(Reference Bano, AlShammari and Fatima22). Results by Phagava et al. indicated that 26 % of Tbilisi State Medical University students in Georgia never eat breakfast, 76 % add sugar to tea or coffee, 54 % add salt to cooked meals and 30 % never eat raw or cooked vegetables(Reference Phagava, Mikaberidze and Tavadze23). Phagava et al. further found better dietary practices and diet quality among health students compared with non-health students(Reference Phagava, Mikaberidze and Tavadze23).
Regardless of the intervention, the employees had better dietary practices than students. Acknowledging the short duration of the nutrition intervention in this study, Princess Nourah Bint Abdulrahman University staff did not have sufficient time to attend most of the nutrition intervention programme. Time factors may have played a role in employees’ knowledge and dietary practice scores compared with those of students. The majority of nutritional intervention studies assessed the changes in practice 6 weeks after intervention(Reference Pearson, Atkin and Biddle24,Reference Gardner, Sheals and Wardle25) . A study about the efficacy of nutrition intervention on knowledge, attitude and practice among working women noticed that a minimum of 6 months of intervention is needed to induce noticeable changes in dietary practices(Reference Monga, Sachdeva and Kochhar26).
Although the scores pertaining to practice did not differ significantly between students and employees after the intervention, there was a 3 % change in dietary practice, including increased vegetable intake and increased physical activity. A possible explanation is that Princess Nourah Bint Abdulrahman University students and employees are occupied with exams and class projects that might affect the motivation to monitor dietary practices(Reference Worsley27). In addition, a cross-sectional study conducted at Peshawar University showed that stress level and time are two factors that influence students’ healthy practices in addition to nutrition knowledge(Reference Zulfiqar, Hafiz and Ali28). A similar result was found in a study with Malaysian adolescents where the participants’ attitudes and practices did not change significantly after a nutrition programme, and the researchers concluded that knowledge might increase, but it is not the only factor that contributes to behavioural changes and influences dietary practices(Reference Worsley27,Reference Spronk, Kullen and Burdon29) . The current study found a positive weak correlation between nutrition knowledge and dietary practice.
This study is based on self-reporting; thus, recall bias might affect recall accuracy. To overcome this bias in future research, it is recommended for participants to use diaries to track changes in food consumption. Another limitation pertains to respondents’ comprehension of some of the technical terms and descriptions used in the survey. For future study, adding definitions of the technical terms to survey items would help the participants understand the meaning of some terminology. The generalisability of the results should be approached carefully; the results came from only one university, Princess Nourah Bint Abdulrahman University. Finally, the questionnaire about practice needs to be administrated no fewer than 6 weeks after the intervention.
Conclusion
The nutrition awareness programme was effective in improving students’ nutritional knowledge; however, no significant effect was found on dietary practices. Future nutrition awareness programmes should separate the activities for students and staff focusing on one target population at a time. A longer duration of the awareness programmes, nutrition support interventions, peer nutrition education programmes and follow-ups with participants would help to improve the dietary practices of students and staff in the academic settings. Further, a qualitative study to identify the challenges that could affect healthy practices is also needed.
Acknowledgements
Acknowledgements: This research was funded by the Deanship of Scientific Research at Princess Nourah Bint Abdulrahman University through the Fast-track Research Funding Program. The authors specially thank the Dean of Student Affairs Deanship Dr. Monerah Almgrn for supporting the research. The authors also thank the Saudi Food and Drug Authority to provide the material to conduct the education programme and the intervention study. The authors would like to thank Anfal Alshatowy, Mona al-Othaim, Muneera Alessa, Nouf Almosaiteer, Nour Albloey, Norah Alshimali, Ebtisam Alsulaiman, Buthaina Alsaif, Abeer Alnasser and Nashmiah Aljeser for helping in data collection. Financial support: This research was funded by the Deanship of Scientific Research at Princess Nourah Bint Abdulrahman University through the Fast-track Research Funding Program. No grant number provided. Conflict of interest: The authors declare no conflicts of interest. Authorship: A.S.A., N.I.A., A.A.A., N.A.A. and A.N.A. have contributed to the conceptualisation of the research idea, designing the methods. N.I.A., A.A.A. and N.A.A. facilitate the data collection. Both A.S.A. and A.N.A. analysed and interpreted the data and wrote the paper. All authors approved the final manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Princess Nourah Bint Abdulrahman University Institutional Review Board (IRB# H-01-R-059). Written informed consent was obtained from all subjects.






