
Contents
Poster Presentation
Surveillance/Public Health
Prevalence of Healthcare-Associated Infections at the National Hospital During the COVID-19 Pandemic in Peru
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s78-s79
-
- Article
-
- You have access
- Open access
- Export citation
Multifacility Outbreak of NDM/OXA-23–Producing Acinetobacter baumannii in California, 2020–2021
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s79
-
- Article
-
- You have access
- Open access
- Export citation
Surveillance of Candidemia in Connecticut: An Epidemiological Comparison Between Two Periods
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s79-s80
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Candidemia is the fourth most common bloodstream infection in hospitalized patients in the United States, with an attributable mortality rate between 30% and 50%. Understanding the epidemiology of candidemia is critical due to its prevalence and association with extended hospital stays, high treatment cost, and significant morbidity and mortality. In 2019 the Connecticut Department of Public Health deemed candidemia a mandatory reportable condition and began state-wide surveillance in conjunction with the CDC’s Emerging Infections Program (EIP). Previously, the EIP had conducted population-based statewide surveillance of candidemia in Connecticut from 1998 to 2000, allowing an opportunity to assess how the epidemiology of candidemia has evolved. The goal of this study is to compare state-wide Connecticut EIP candidemia data from 2 periods (1998–2000 and 2019) to identify trends in infections and incidence, providing insight for potential improvements to current prevention measures and treatments. Methods: The sample population included all Connecticut residents aged ≥20 who tested positive for a candidemia infection during 1998–2000 and 2019. Patients who had positive blood cultures for Candida spp but were < 20 years old or were not Connecticut residents were excluded. Connecticut EIP candidemia case report forms from each time period were compared and matching fields were chosen as variables for univariate analysis to search for statistically significant differences. Selected variables include: Candida species present in blood culture, patient demographics, previous exposures to healthcare settings, length of stay, presence of central venous catheter (CVC), and location of the patient at diagnosis (community vs. hospital onset). De-identified patient-level information was provided by the EIP. Results: In total, 381 candidemia episodes from 1998–2000 were compared to 247 episodes in 2019. The proportion of C. albicans species in 1998–2000 was 49.9% and declined to 40.5% of cases in 2019 (P = .02). Outcomes improved as well, with 65.2% of patients in 2019 having survived compared to 51.4% in 1998–2000 (P = .001). Other findings indicate that patients with candidemia in 2019 were less likely to have a central venous catheter, less likely to have undergone a recent surgery, and were more likely to have community-onset infection (all p < 0.05). Conclusions: The epidemiology of candidemia has changed over the past 20 years, with significant improvements in patient survival and a shift toward community-onset infections and non-Albicans spp. These findings have important implications in designing prevention strategies and optimizing candidemia management, particularly in the community setting where increased intravenous drug use and the availability of home healthcare may be important factors.
Funding: No
Disclosures: None
Table 1. 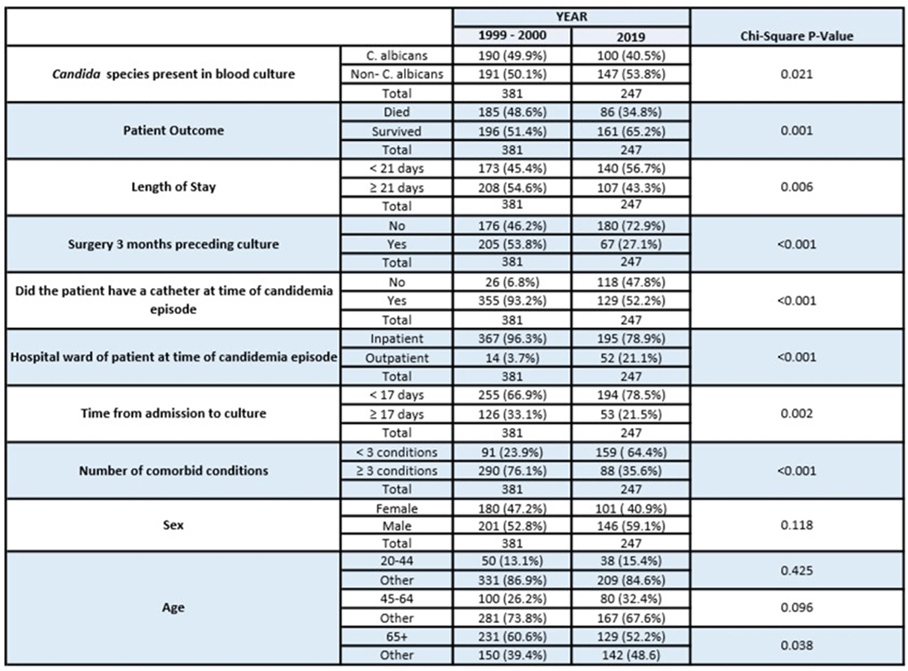

VAE
Does a Starting Positive End-Expiratory Pressure of 8 cm H2O Decrease the Probability of a Ventilator-Associated Event?
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s80
-
- Article
-
- You have access
- Open access
- Export citation
-
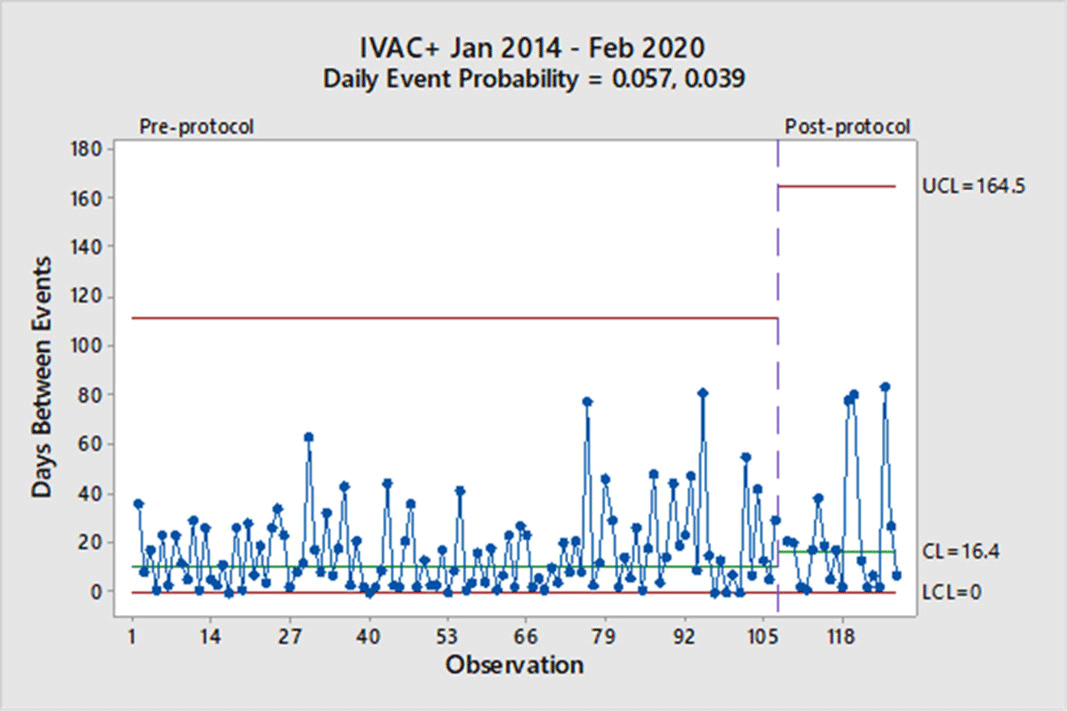
Background: Mechanical ventilation is commonly seen in critical ill patients. The vulnerability of these patients is high, and a wide range of associated conditions can stem from this intervention. To objectively identify nosocomial respiratory conditions and provide conformed surveillance definitions of these events, the Centers for Disease Control and Prevention (CDC) established the ventilator-associated event (VAE) criteria. They denote 3 categories of increasing progression in mechanically ventilated patients from a ventilator-associated condition (VAC) to an infection-related ventilator-associated complication (IVAC) and finally to a possible ventilator-associated pneumonia (PVAP). Manipulation of ventilator settings, such as starting on higher values to not trigger VAC criteria, has been criticized by some experts as not only ‘gaming the system,’ but potentially harming patients. In October 2018, our institution began a baseline of 8 cm H2O as the starting positive end-expiratory pressure (PEEP) protocol for mechanical ventilation but exempting neurosurgical patients. We sought to determine whether an 8 PEEP protocol is an effective strategy for reducing VAEs in our institution. Methods: We retrospectively examined patient data at our institution from January 2014 through February 2020. VAEs were separated by VAC only and IVAC positive (+), which are a combination of IVACs and PVAPs. Using the days between VAEs, a daily event probability can be calculated based on the geometric distribution. Furthermore, as VAEs occur, the likelihood of the event can be assessed as expected or unexpected using a strict probability limit of 0.99865 to reduce type 1 errors. Results: In total, 307 patients were identified in our hospital’s VAE surveillance. Of those, 180 met CDC-defined VAC-only criteria, and 127 patients met IVAC+ definitions. After implementation of an 8-PEEP protocol, the daily event probability for VACs decreased from 0.083 to 0.047. The last event occurred 162 days after the previous VAC, which was unexpected, because the probability of occurrence extended beyond the probability limit. With regard to IVAC+ events, the daily event probability decreased from 0.057 to 0.039 without significant reduction in the IVAC+ rate. Conclusions: Although a change in the VAC-only rate occurred, signified by a longer time between events, it took more than a year to achieve in our institution. Additionally, we did not see a reduction in the IVAC+ rate. These findings suggest that an 8-PEEP protocol may be able to reduce VAEs due to noninfectious etiologies, such as congestive heart failure and atelectasis.
Funding: No
Disclosure: None
Figure 1.
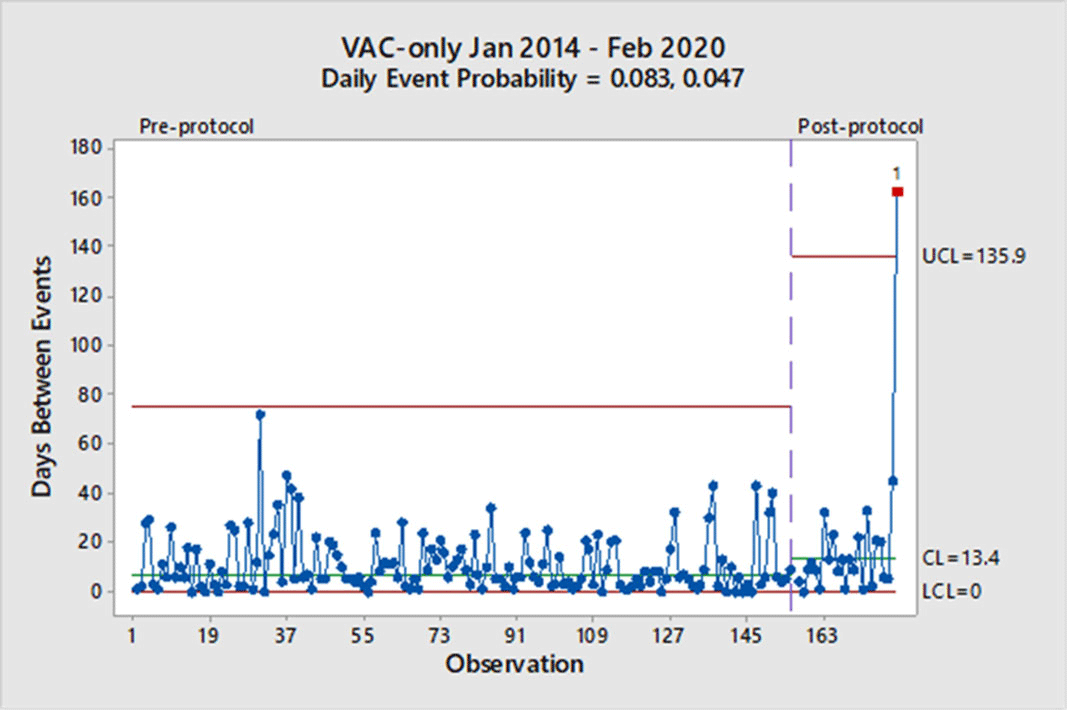
Figure 2.


Knobmanship: Dialing Up Understanding of VAE Triggers
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s80-s81
-
- Article
-
- You have access
- Open access
- Export citation
-
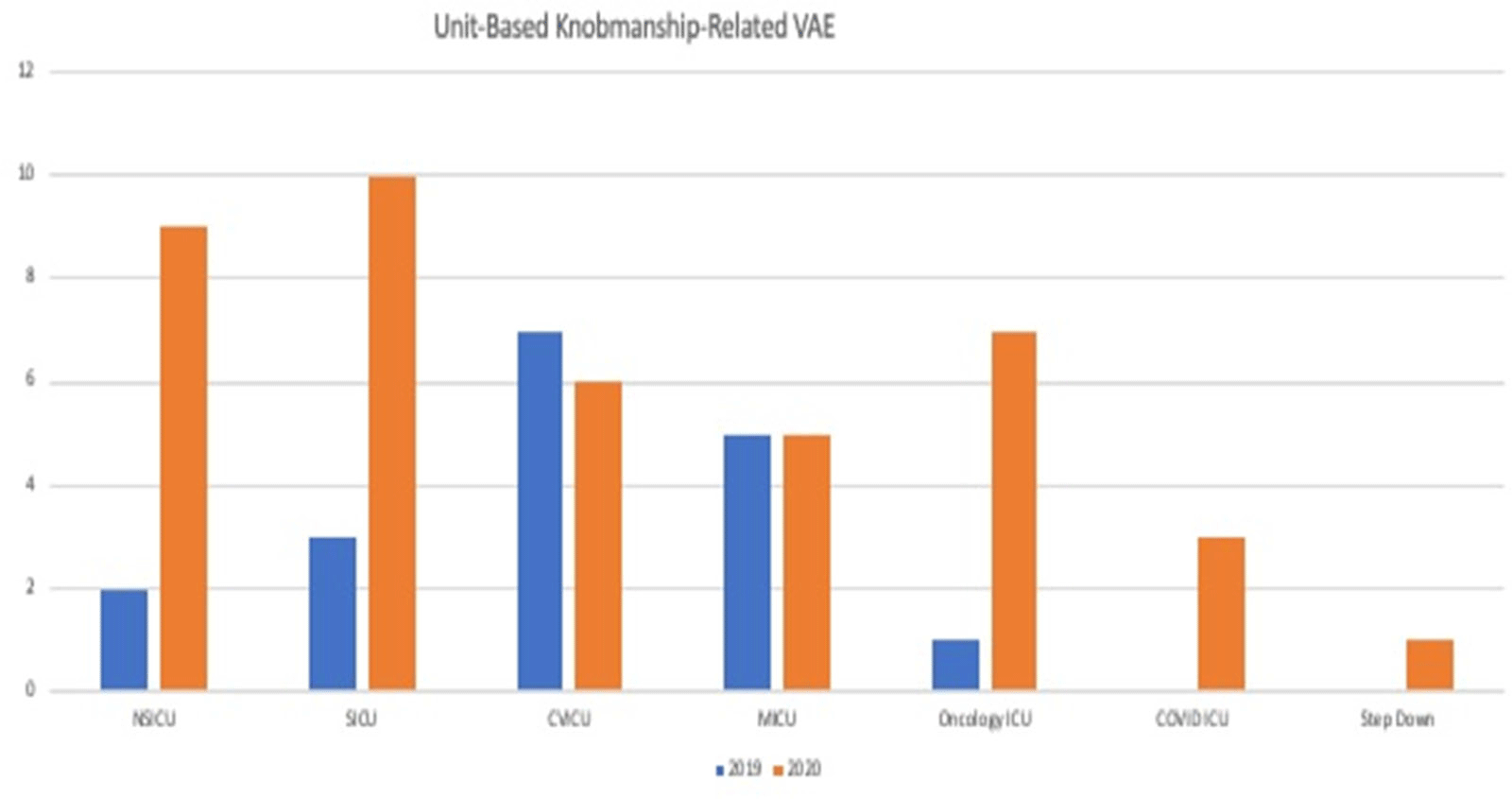
Background: Mechanical ventilation is a lifesaving therapy for critically ill patients. Hospitals perform surveillance for the NHSN for ventilator-associated events (VAE) by monitoring mechanically ventilated patients for metrics that are generally thought to be objective and preventable and that lead to poor patient outcomes. The VAE definition is met in a stepwise manner; initially, a ventilator-associated condition (VAC) is triggered with an increase in positive end-expiratory pressure (PEEP, >3 cm H2O) or fraction of inspired oxygen (FIO2, 0.20 or 20 points) after a period of stability or improvement on the ventilator. We believe that many reported VAEs could be avoided by provider and respiratory therapy attention to “knobmanship.” We define knobmanship as knowledge of the VAE definition and trigger points combined with appropriate clinical care for mechanically ventilated patients while avoiding unnecessary triggering of the VAE definition by avoiding small unneeded changes in PEEP or FIO2. Methods: We performed a chart review of 283 patients who had a reported VAE to the NHSN between January 1, 2019, and December 31, 2020. We collected data including type of VAE, VAE triggering criteria, and clinical course. Results: Of the 283 VAEs, 59 were triggered by a PEEP increase from 5 to 8 with stable or decreasing FIO2. Of the 59 VAEs, 33 were VACs, 18 were infection-related ventilator- associated complications (IVACs), and 8 were possible ventilator-associated pneumonia (PVAP). Most of these transient changes in PEEP were deemed clinically unnecessary. A 21% reduction of VAEs reported to the NSHN over the 2-year review period could have been avoided by knobmanship. Conclusions: The VAE definition may often be triggered by provider bias to the ventilator settings rather than what the patient’s clinical-condition requires. Attention to knobmanship may result in substantial decrease in reported VAE.
Funding: No
Disclosures: None
Figure 1.

Viral Infections
Impact of a Comprehensive SARS-CoV-2 Infection Prevention Bundle on Rates of Hospital-Acquired Respiratory Viral Infections
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s81
-
- Article
-
- You have access
- Open access
- Export citation
-
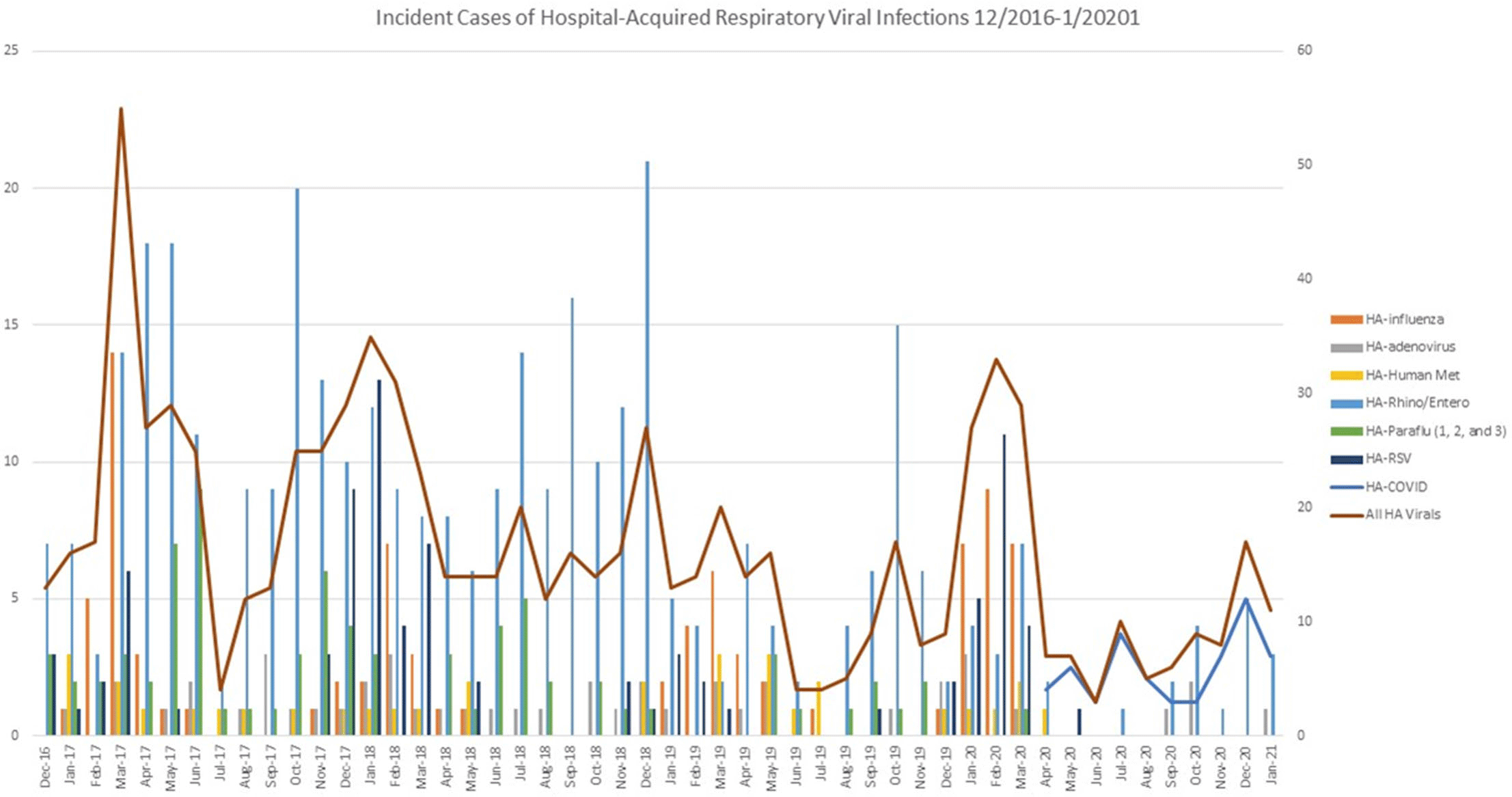
Background: We evaluated the impact of a comprehensive SARS-CoV-2 (COVID-19) infection prevention (IP) bundle on rates of non–COVID-19 healthcare-acquired respiratory viral infection (HA-RVI). Methods: We performed a retrospective analysis of prospectively collected respiratory viral data using an infection prevention database from April 2017 to January 2021. We defined HA-RVI as identification of a respiratory virus via nasal or nasopharyngeal swabs collected on or after hospital day 7 for COVID-19 and non–COVID-19 RVI. We compared incident rate ratios (IRRs) of HA-RVI for each of the 3 years (April 2017 to March 2020) prior to and 10 months (April 2020 to January 2021) following full implementation of a comprehensive COVID-19 IP bundle at Duke University Health System. The COVID-19 IP bundle consists of the following elements: universal masking; eye protection; employee, patient, and visitor symptom screening; contact tracing; admission and preprocedure testing; visitor restrictions; discouraging presenteeism; population density control and/or physical distancing; and ongoing attention to basic horizontal IP strategies including hand hygiene, PPE compliance, and environmental cleaning. Results: During the study period, we identified 715 HA-RVIs over 1,899,700 inpatient days, for an overall incidence rate of 0.38 HA-RVI per 1,000 inpatient days. The HA-RVI IRR was significantly higher during each of the 3 years prior to implementing the COVID-19 IP bundle (Table 1). The incidence rate of HA-RVI decreased by 60% after bundle implementation. COVID-19 became the dominant HA-RVI, and no cases of HA-influenza occurred in the postimplementation period (Figure 1). Conclusions: Implementation of a comprehensive COVID-19 IP bundle likely contributed to a reduction in HA-RVI for hospitalized patients in our healthcare system. Augmenting traditional IP interventions in place during the annual respiratory virus season may be a future strategy to reduce rates of HA-RVI for inpatients.
Table 1. 
Figure 1.


Front Cover (OFC, IFC) and matter
ASH volume 1 issue s1 Cover and Front matter
-
- Published online by Cambridge University Press:
- 29 July 2021, p. f1
-
- Article
-
- You have access
- Export citation