



Road traffic injuries (RTIs) constitute an important public health and socioeconomic problem, globally. It is estimated that road traffic accidents (RTA) are responsible for about 1.35 million deaths every year, 50 million severely injured, and millions more disabled. However, low- and middle-income countries (LMICs) bear the brunt (90%) of the global RTI and mortality burden. Countries on the African continent carry the highest rate of road traffic death among world regions, despite having the fewest number of vehicles (1% of the total registered vehicles worldwide). Reference Kobusingye, Hyder, Bishai, Jamison, Bremen and Measham1,2
In 2016, Liberia had the highest rate of road traffic death (35.9 per 100 000 people) in Africa, followed by Burundi and Zimbabwe. Although Nigeria reported lower rates (21.4 per 100 000 people) than Ghana and South Africa, the burden of RTI and mortality is still predicted to increase in LMICs. 2,3 The disproportionate burden in LMICs can be attributed to a number of factors, including poor implementation of primary prevention strategies, such as laws on speeding and driving under the influence of alcohol or drug; lack of helmet use; distracted driving with mobile phone; and a weak prehospital care (PHC) system. 2,Reference Sasser, Varghese and Kellermann4,Reference Mock, Arreola-Risa and Quanssah5
Specifically, the barriers to PHC system development in LMICs include inadequate funding, lack of leadership, poor legislation, inadequate skilled personnel, and other factors. Reference Nielsen, Mock and Joshipura6,7 Currently, the continent of Africa contains only 25 emergency medical services (EMS) systems, located in 16 countries, and serving a meager 30% of the continent’s population. Reference Mould-Millman, Dixon and Sefa8 PHC is the first aid/basic life support (FA/BLS) given to injured victims at the scene and during transportation to a health facility for definitive care, especially within the “golden hour of injury,” that is, the first hour after the injury’s occurrence. 9 Many injury providers recognize that providing care within the golden hour increases the likelihood of favorable clinical outcomes. Reference Carr, Caplan, Pryor and Branas10 Studies have shown that the majority of road traffic accident-related deaths in LMICs occur during the prehospital phase. Reference Evans, van Wessem and McDougall11,Reference Murad, Larsen and Husum12 Therefore, a timely and coordinated PHC system is essential to the significant reduction of RTI morbidity and mortality. Reference Rogers, Rittenhouse and Gross13,Reference Mock, Joshipura, Arreola-Risa and Quansah14
Although there is no formal national PHC system in Nigeria, Lagos State has a functional and efficient PHC system, which was created in 2001—the Lagos State Ambulance Service. Reference Mock, Joshipura, Arreola-Risa and Quansah14–16 First responders (road safety corps, police, firefighters, drivers, relatives, and bystanders) are expected to have some FA/BLS knowledge and skills as well, since they are often the ones who assist most trauma victims in Nigeria. 7,9,Reference Adeloye15,Reference Olumide, Asuzu and Kale17,Reference Geduld and Wallis18 However, studies have shown that they generally provide little to no PHC to these victims, aside from transporting them to the emergency department. Reference Adeloye15,Reference Kobusingye, Hyder and Bishai19,Reference Solagberu, Ofoegbu and Abdur-Rahman20 Despite the ongoing efforts in developing a national PHC system in Nigeria, especially with the launch of its first national policy on emergency medical services and operational guidelines for national ambulance services in February 2018, implementation remains a major challenge. Reference Nielsen, Mock and Joshipura6,21
A study in Tanzania reported that only 3% of police officers had good knowledge of FA for PHC of road traffic accident victims. Reference Lukumay, Ndile and Outwater22 Another study from Thailand found that 23% of police officers had good knowledge of FA. Reference Shrestha, Pacheun, Boonshuyar and Shrestha23 In Nigeria, nothing is known about police officers’ competencies in FA or BLS for PHC of road traffic accident victims. Reference Sztajnkrycer, Callaway and Baez24 With a view to strengthening the existing PHC system in Nigeria through evidence-based interventions toward achieving sustainable development goal (SDG) targets 3.6 and 11.2, we conducted this study to assess police officers’ experience with FA/BLS, identify gaps in their FA/BLS knowledge and skills, and also to assess police stations’ FA/BLS equipment capacity for PHC of RTA victims.
Methods
Study Design
We used a cross-sectional descriptive study design. Data were collected from November to December 2018.
Setting
The study was conducted in police stations located in the Federal Capital Territory (FCT) Abuja. Each police station consisted of general-duty (GD) police and specialist police officers (SP). GD police are officers whose duties involve road check-point patrols, arrest of offenders and traffic control, whereas SP officers (eg, medical personnel) do not usually engage in such activities. Abuja is the capital city of Nigeria. It is located in central Nigeria within the Federal Capital Territory (FCT) and comprises 6 area councils: Abaji, Abuja Municipal, Gwagwalada, Kuje, Bwari, and Kwali. Abuja has an estimated population of 8 million, is the second most populous city in Nigeria, and the fastest growing city in Africa. 25 GD police were selected for this study because they are more commonly involved in PHC of RTA victims, particularly for accidents that occurred on highways. Abuja was selected because it was reported to have the highest number of RTA according to a 2017 road transport data. 26
Study Population
The study population was the GD police working in Abuja across the 6 area councils. The inclusion criteria were English speaking police and those who consented to the study while the exclusion criteria were specialist police, non-English speaking, and non-consenting GD police.
Sample Size
Sample size was calculated using Leslie Kish’s formula for qualitative dependent variable, with 50% of the true proportion estimated to be in the population. Reference Bamgboye27 The level of significance was set at 5%, and after adjusting for a non-response rate of 10%, the sample size was 428 police.
Sampling Technique
A stratified random sampling with proportional allocation method was used to randomly select police who participated in the study. After receiving approval from the Inspector General of Police (IGP), we requested the Commissioner of Police in Abuja to provide information on the total number of police stations and the police population in each station. There were 31 stations and the total police population was 7413 officers. The sample size for each station was calculated using the formula (Ns x n/N), where Ns, n, and N represented police population in each station, study sample size, and total police population, respectively. Reference Bamgboye27 A ballot system was used to randomly select police from each station. At each station, the police assembled into a private room and were selected by doubling the calculated sample size per station. Folded pieces of paper, half labeled with both “yes” and the other half with “no,” were put into a box. Police were asked to pick a folded paper from the box and those who picked a yes-labeled paper were asked if they would voluntarily participate in the study. All consenting police then participated in the study.
Data Collection Instrument, Technique, and Validation
A self-designed, semi-structured questionnaire was used to collect data. The questionnaire was developed through an in-depth literature review and shared trauma competencies by this study’s authors. Of these 5 authors, all are certified first aiders/life support providers, 2 are trauma surgeons, and 1 is a trauma research fellow. The questionnaire was pretested and the calculated Cronbach’s alpha of 0.76 demonstrated the internal consistency and reliability of our study instrument. Pretesting of the questionnaire was done among 43 police who were randomly selected from a different setting (Police Force Headquarters) that was not included in the actual study.
Study data were collected and managed using REDCap (Research Electronic Data Capture), a secure, web-based software platform for survey data management. Reference Harris, Taylor and Thielke28 The questionnaire was in English and contained an informed consent page along with 4 sections, which can be found in Appendix A. The questionnaire had 25 questions. Section A contained questions on socio-demographics (eg, age, sex, level of education, work experience, and rank). The question on level of education did not have “no formal education” and “primary” options because the minimum educational requirement to join the Nigerian Police Force (NPF) is a secondary school or “O Level” certificate. 29 The age and work experience requirements for retirement in the NPF are 60 years and 35 years of service, respectively. 30 Hence, the maximum range for age was 59 years and work experience was 34 years. Section B had questions on participant awareness of and training on FA/BLS. Further questions included locations of and topics taught in their most recent FA/BLS training. Section C had 6 closed-ended questions on knowledge of FA/BLS. Section D had 8 closed-ended questions on skills of FA/BLS that were answered based on a simulation scenario, whose development was guided by the literatures.
Additionally, a checklist was used to determine the presence or absence of FA/BLS equipment in each police station. Reference Morgan31,Reference Glavin and Gaba32 With the exception of not understanding some medical terminology (eg, automated external defibrillator) that the trained research assistants helped explain, none of the police reported difficulty in understanding the questionnaire. Although the questionnaire was self-administered by the participants, the data were collected in the presence of trained research assistants in order to ensure completeness of data and to provide necessary clarifications. The participants took 20–30 minutes to complete the questionnaire.
Data Analysis
Data analysis was performed using STATA v 14.0 (StataCorp, College Station, TX). Of the 428 GD police who were enrolled for this study, 419 participants were analyzed. The data collected on outcome qualitative variables (eg, awareness, knowledge, skills, and preparedness on FA/BLS for PHC of RTI victims) and independent qualitative variables (eg, age, sex, level of education, and rank) were presented as frequencies and percentages. Officer ranks, including constable, corporal, sergeant, and inspector, were grouped as “junior police” while assistant superintendent of police, deputy superintendent of police, superintendent of police, chief superintendent of police, and assistant commissioner of police and above were grouped as “senior police.” Means and standard deviations were used to summarize data collected on quantitative variables (eg, knowledge score and skills score). Bivariate analysis using chi-square was done to test statistical significance of the association between outcome and independent variables. Multivariate logistic regression was further used to adjust for the effect of confounders in the associations observed. A total of 14 questions were used to assess both knowledge and skills on FA/BLS. We categorized the composite knowledge and skills score into 3 groups: “Poor” (0–4), “Fair” (5–9), and “Good” (10–14). These groups corresponded to “Underprepared,” “Somewhat Prepared,” and “Prepared,” respectively.
Ethical Consideration
The FCT Health Research Ethics Committee approved this study (FHREC 2018/01/57/08-05-18) and the University of Texas Southwestern Medical Center’s Institutional Review Board also granted its approval as non-regulated research (45 CFR 46.102). Permission to conduct this study was granted by the IGP. Before data collection, the purpose of this study was explained to the police, and they were assured of confidential responses. Also, the participation of each police was voluntary and a written informed consent with signature was obtained. The NIH Partnerships to Develop Injury Research Capacity in the Sub-Saharan Africa grant (5D43TW010463-03) supported this research.
Results
Sociodemographic Characteristics of Study Participants
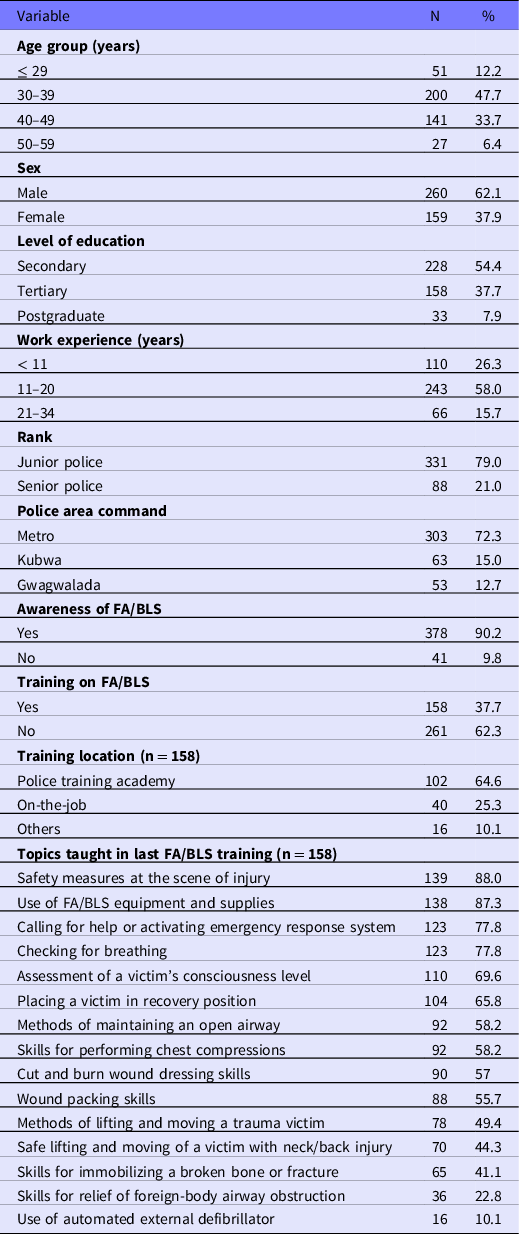
About two-thirds (62.1%) were male. Police in the age interval 30–39 years were about half (47.7%) of the participants. A little more than half (54.4%) had a secondary level of education. Police in the work experience interval 11–20 years were more than half (58.0%) of the participants. Slightly more than three-quarters (79.0%) had a rank in the junior police category. Regarding police area command, a majority (72.3%) of the participants were from metro area command (Table 1).
Table 1. Sociodemographic characteristics of and awareness and training in study participants on FA/BLS (N = 419)
Awareness and Training on FA/BLS
Nearly all (90.2%) of the police were aware of FA/BLS. Slightly more than one-third (37.7%) of the participants had ever received training on FA/BLS. Of those who had received previous training on FA/BLS, 64.6% were trained at the police academy, while 25.3% were trained on-the-job (see Table 1).
Knowledge on FA/BLS
The mean knowledge score was 3.48 (SD = 0.99). Concerning questions on assessment of level of consciousness and initial care for a victim with cardiac arrest, slightly more than two-thirds (68.0% and 68.7%) of the police respectively provided the correct answers. A little more than half (53.0%) gave the correct answer to the question about assessment of an unconscious breathing victim. The proportions of police who knew the importance of severe bleeding control and spine protection in a victim with neck/back injury were only 6.4% and 8.8%, respectively. Nearly half (47.0%) correctly answered the question on identification of priority conditions in mass casualties (Table 2).
Table 2. Knowledge and skills of participants on FA/BLS (N = 419)

Skills on FA/BLS
The mean skills score was 3.10 (SD = 1.49). Higher proportions (79.5% and 78.0%) of the participants respectively gave correct answers to the questions pertaining to initial care for a conscious victim with breathing difficulty and safe lifting of a victim with neck/back injury. Slightly more than three-quarters (76.1% and 77.1%) of the police respectively could accurately provide initial care for an unconscious breathing victim and ensure safety at the scene of injury. Almost one-quarter (23.2%) lacked the skills on severe bleeding control. About one-third (32.0%) did not know how to immobilize a broken bone or fracture. More than half (55.9%) had the skills to provide initial care for a victim with cardiac arrest. A little more than two-thirds (68.7%) could correctly identify priority conditions in mass casualties (see Table 2).
Rating of Knowledge, Skills, and Preparedness on FA/BLS
The mean total knowledge and skills score was 6.58 (SD = 1.92) and the distribution of scores is shown in Figure 1. Only 5.7% of officers scored in the Good (Prepared) category, with 79.0% scoring in the Fair (Somewhat Prepared) category, and 15.3% scoring in the Poor (Underprepared) category, as seen in Figure 2.
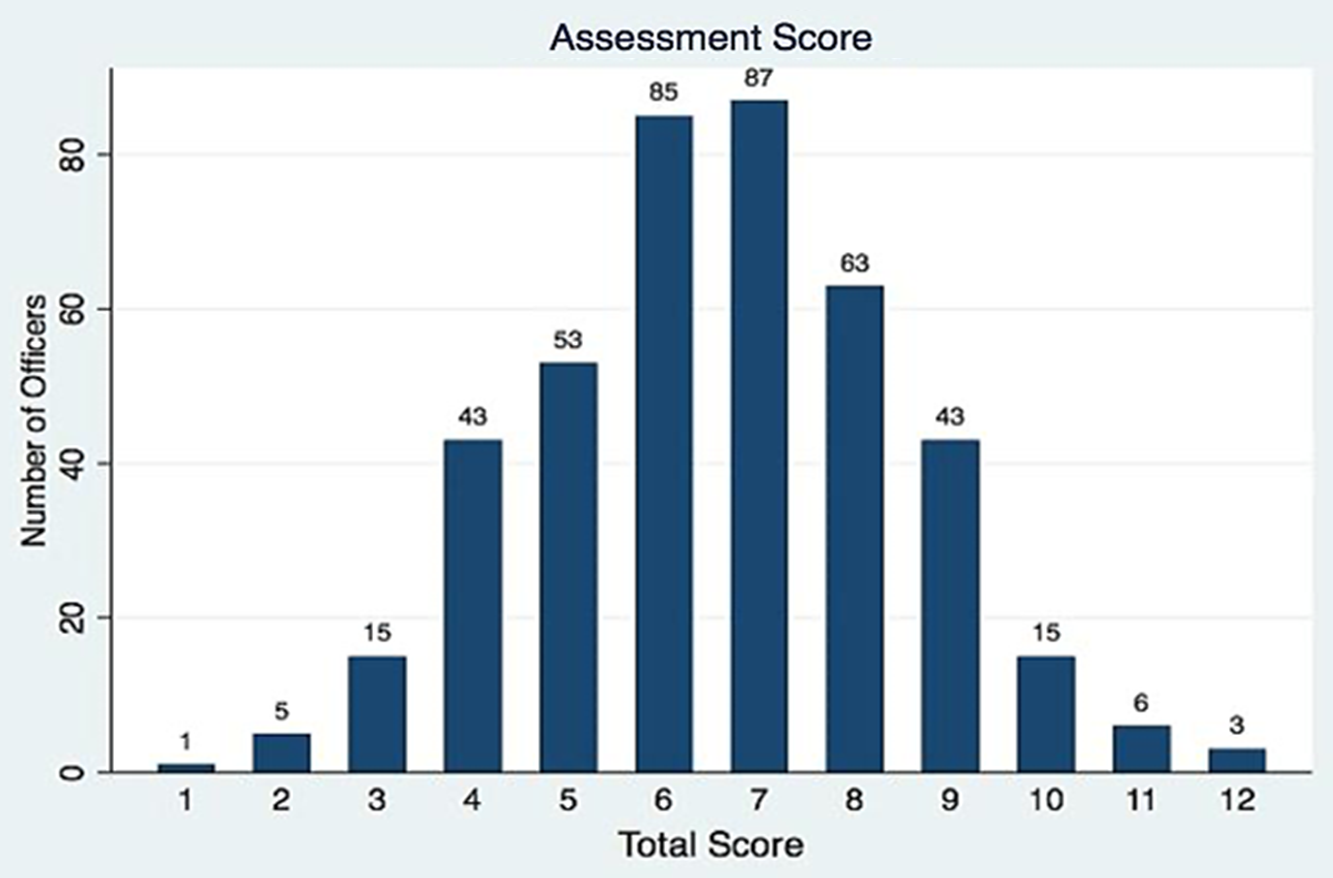
Figure 1. Total knowledge and skills score on FA/BLS (N = 419).
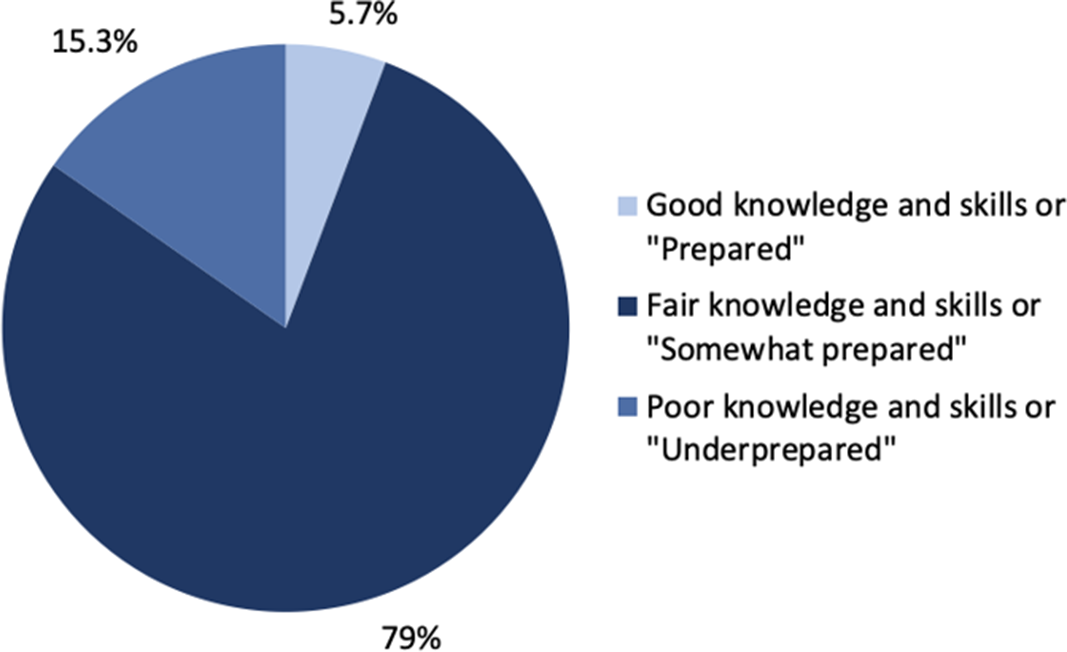
Figure 2. Ratings of knowledge, skills, and preparedness on FA/BLS (N = 419).
Rating of Knowledge and Skills by Variables on Sociodemographics, Awareness, and Training on FA/BLS
Of the GD police with secondary level of education, 1.8% showed good knowledge and skills on FA/BLS; 3.9% of those with rank in the junior police category exhibited good performance; 6.1% or one out of every 16 participants who were aware of FA/BLS had good knowledge and skills. One out of every 13 GD police who had previous training on FA/BLS demonstrated good knowledge and skills (Table 3).
Table 3. Rating of knowledge and skills of GD police by variables on sociodemographics, awareness, and training on FA/BLS

Factors Associated with Knowledge and Skills on FA/BLS
The bivariate analysis in Table 4 showed that level of education (P = 0.000) and rank (P = 0.004) were statistically associated with knowledge and skills of FA/BLS. The results of multivariate analyses reinforced the association between knowledge and skills of FA/BLS and level of education. However, rank was no longer statistically associated with either Poor or Good knowledge and skill categories. Both tertiary (OR = 3.35, 95% CI: 1.01-11.11, P = 0.048) and postgraduate (OR = 6.89, 95% CI: 1.63-29.19, P = 0.009) levels of education had statistically significant associations with Good knowledge and skills. Police with tertiary level of education were 3.35 times more likely to have good knowledge and skills on FA/BLS and 73% less likely to have poor knowledge and skills on FA/BLS (OR = 0.27, 95% CI: 0.13-0.57, P = 0.001) when compared to police with secondary level of education. Police with postgraduate level of education were 6.89 times more likely to have good knowledge and skills when compared to police with secondary level of education (Table 5).
Table 4. Bivariate analysis of factors associated with knowledge and skills on FA/BLS

χ 2 , chi-square test.
* P-value < 0.05 significance level.
Table 5. Multivariate logistic regression analysis of factors associated with knowledge and skills on FA/BLS
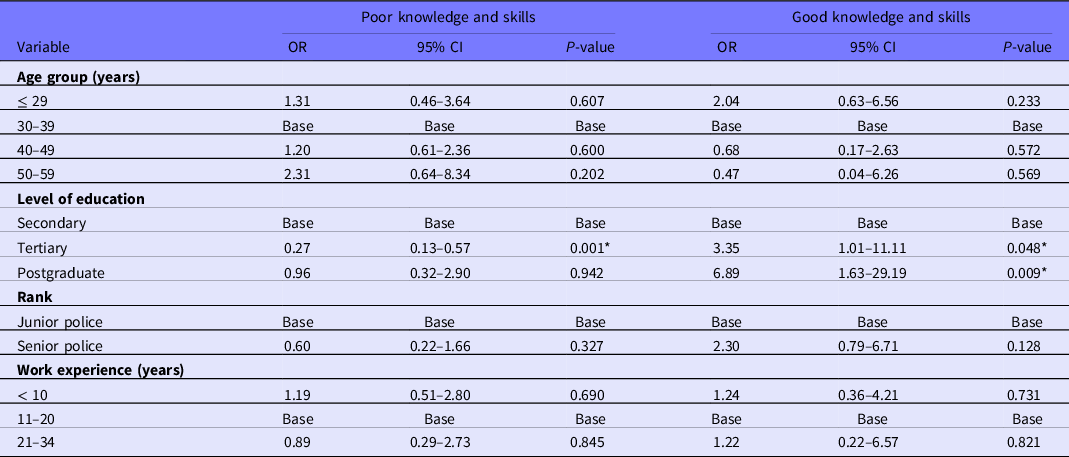
Base, the median for each variable. Fair knowledge and skills were also used as a base and therefore not displayed in the table.
* P-value < 0.05 significance level.
FA/BLS Equipment Checklist
Almost all of the police stations surveyed lacked an overwhelming majority of the specified items (eg, disposable gloves, bandages, spine board, automated external defibrillator), which can be found in Appendix B.
Discussion
The objective of this study was primarily to assess police officers’ experience with FA/BLS and to identify gaps in their FA/BLS knowledge and skills. We surveyed 419 GD police across all police stations in Abuja, Nigeria, and found that most of the participants were between 30 and 39 years old and had completed secondary education. Although the overwhelming majority of the GD police were aware of FA/BLS, only 5.7% had good knowledge and skills.
Our study found that only 37.7% of GD police had ever received training on FA/BLS even though it is recommended as one of the training courses for new and serving police officers in many countries, including Nigeria, Tanzania, Thailand, and the United States. This training is important so that police can fulfil their role as one of the first responders in providing PHC during emergency situations, particularly trauma from RTA. In contrast, a study conducted among police in Thailand found that more than half (56.2%) had received training on handling RTI cases. Reference Shrestha, Pacheun, Boonshuyar and Shrestha23 Furthermore, we observed that only a quarter of those previously trained on FA/BLS were trained on-the-job, while other studies from Tanzania and the United States reported that more than half of their police had received their most recent FA/BLS training on-the-job. Reference Lukumay, Ndile and Outwater22,Reference Sztajnkrycer, Callaway and Baez24 These differences might be explained due to varying availability of resources (such as funds, equipment, and experts) for FA/BLS training. Another explanation could be the lack of prioritization of limited government funds for FA/BLS training by the NPF management. This could be addressed through reprioritizing FA/BLS training and equipping the NPF with the necessary funds and resources. Similarly, the development and implementation of PHC policy and strategic planning within the NPF are also essential to achieving a sustainable FA/BLS training program. In addition, it is important for the NPF to build upon existing collaborations and also create new partnerships with local and international stakeholders in the public and private sectors, to harness adequate resources for this training.
Regarding FA/BLS skills, only 23.2% of the GD police in Nigeria knew the correct method of controlling severe bleeding, which greatly differs from the 81.8% of Tanzanian police officers who possessed this skill. The proportion of police in our study who knew to use a piece of hard material and bandage to immobilize a broken bone (32.0%) was lower than 46.5% reported with Tanzanian police. This is consistent with our findings that “skills for immobilizing broken bone” and “cut dressing skills” were part of the rarely taught topics reported by the police who have had a previously attended FA/BLS training (see Table 1). Additionally, the deficiencies in these skills could be possibly attributed to our findings that only 6.4% and 8.8% of police had accurate knowledge on the importance of controlling a severely bleeding cut and protecting a broken spinal bone, respectively (see Table 2). This suggests that there is a need for trauma experts to review and further develop the FA/BLS training curriculum for the NPF.
Equally important is the need to ensure that the police make informed decisions whenever they are confronted with emergency situations, rather than being robotic in their approach. When trainees are only exposed to practical teachings without being taught the theoretical basis for the skills acquired, their training is incomplete. For example, training inadequacy can potentially explain our finding that, even though 78.0% of the police knew how to correctly lift a victim with a neck or back injury, only 8.8% of the police knew that the importance of protecting the spine in neck and back injuries was to prevent further damage that may lead to paralysis. Likewise, a low skills performance was observed regarding initial care for victim with cardiac arrest even though more than two-thirds (68.7%) of the police had correct knowledge, that is, performing chest compression, when an answer option that read “rapidly transport the victim to the hospital for immediate assistance,” was not included in the knowledge test question. Nevertheless, we found that only 55.9% of the police knew that performing chest compression was the right thing to do when this answer option was included in the skills test question. This observed performance drop showed that some of the police who initially displayed good knowledge still got confused during their skills test or simulation exercise, hence selecting wrong answers. Based on these findings, there is need to improve the quality and teaching methods of the FA/BLS training, such that it has both theoretical and practical components, in order to increase police officers’ FA/BLS competencies (see Table 2).
Concerning the initial care for conscious victim with breathing difficulty, the police in Nigeria did much better than their colleagues both in Thailand and Tanzania, whereby 79.5% of the police in our study knew the appropriate procedure, while about 45.5% of Thai police officers and only 4.7% of Tanzanian officers demonstrated this skill. Reference Lukumay, Ndile and Outwater22,Reference Shrestha, Pacheun, Boonshuyar and Shrestha23 Although the general performance of police in our study was better than what was reported in the Tanzanian study, our finding that 5.7% of the police had good knowledge and skills or were “prepared” on FA/BLS is still comparable to 2.9% reported in the Tanzania. The similarity observed could be attributed to the following explanations. First, Nigeria and Tanzania, as low-income countries, may be faced with the similar challenges, such as inadequate funding, poor leadership, and other issues that have been implicated in the development of PHC, especially in LMICs. Second, the majority of police surveyed in both countries had a secondary level of education (see Table 5). Reference Nielsen, Mock and Joshipura6,7,Reference Lukumay, Ndile and Outwater22 A competency-based educational intervention could improve police knowledge and skills on FA/BLS in Nigeria.
By contrast, the study performed in Thailand showed that about a quarter (23%) of the traffic police surveyed had good knowledge on post-crash FA/BLS. Reference Shrestha, Pacheun, Boonshuyar and Shrestha23 Thailand’s higher economic status is likely to have more resources than a low-income country like Nigeria, which could contribute to the high proportion of well-trained officers.
Also, we found that only 1 out of every 13 police who had previous training on FA/BLS demonstrated good knowledge and skills. This is in contrast to 1 out of every 57 police reported in a study done in Tanzania and comparable to a study conducted in Thailand that showed that 1 of every 4 police had such knowledge. These findings suggest that the quality of FA/BLS training of police in Nigeria was possibly better than that of Tanzania and also lower when compared to Thailand. Reference Lukumay, Ndile and Outwater22,Reference Shrestha, Pacheun, Boonshuyar and Shrestha23
Conclusively, we could not do enough comparative analysis due to limited data that exist on the knowledge of police on FA/BLS for PHC of RTA victims. Notwithstanding, the studies conducted in Thailand and Tanzania were quite useful for arriving at logical inferences in our discussion.
Limitations of the Study
One of the limitations of this study was that, based on the cross-sectional nature of the study, it was not possible to determine causality but only to test for associations. Also, there was unavailability of internationally validated data collection tools that have been used in similar settings; however, data quality was achieved through trauma experts’ review and pretesting of our questionnaire. There may have been possibility of information bias, which could result from either the interviewer or respondent. The interviewer bias may have been due to the varying ways each research assistant gave explanations on questions asked by the participants. To limit such information bias, we conducted an intensive training for the research assistants. Similarly, respondent bias was possible due to the self-reported nature of the questionnaire. In order to reduce this bias, we ensured that the participants were informed of the importance of answering the questions as accurately as possible and were also assured of confidentiality of their responses. Furthermore, a recall bias may have occurred due to retrospective data collected in the questionnaire.
Strengths of the Study
Despite the limitations discussed previously, our study has various strengths. Our study sample is more representative of the police population that actively participates in PHC of trauma victims, unlike the Tanzania and Thailand studies that focused only on traffic police, which is a subunit of the general-duty police. Also, a stratified random sampling technique was used because it has a high precision in estimate of the true proportion of a population with a given outcome variable when compared with simple random sampling technique that was used in these studies. Reference Lukumay, Ndile and Outwater22,Reference Shrestha, Pacheun, Boonshuyar and Shrestha23 Last, this study had a high response rate of 97.9%.
The findings in our study have future implications for evidence-based interventions in the NPF (eg, trainings, policy development, and researches). Also, our study has the potential to advance the body of knowledge on PHC competency among the first responder population considering the fact that it was the first study conducted within this population in Nigeria.
Conclusion
The proportion of police with good knowledge and skills on FA/BLS for PHC of RTA victims is very low. Therefore, the need to plan and implement an educational intervention to increase the police as well as other first responders’ competencies on FA/BLS for PHC of RTA victims is warranted. To achieve this goal, the existence of organized systems such as the medical department in the police or federal road safety corps provides a window of opportunity to standardize and monitor FA/BLS training among first responder populations with respect to its curriculum content, mode of delivery, type of training materials, and frequency. The curriculum content should include contextual realities such as improvisation of FA/BLS equipment. Also, existing digital technology should be leveraged to improve FA/BLS training access through virtual training, electronic training manual, and mobile application. The frequency of the training should be based on available evidence for the time interval (in years) that they are less likely to demonstrate sufficient retention of FA/BLS knowledge and skills, and these competencies could be monitored through mandatory assessments during FA/BLS training sessions and promotional examinations. The training should be delivered in a robust way such that it incorporates both theory and practical components. However, before such trainings are conducted, there is need to develop the FA/BLS curriculum based on the identified knowledge and skill gaps. In addition, we recommend that the NPF management identify strategies to mobilize more resources (eg, first aid kit, police ambulance, communication system, and data registry system) for efficient PHC service delivery.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/dmp.2022.196.
Acknowledgments
We thank the National Institute of Health and Fogarty International Center, United States of America, for funding this project through the D43 Injury Training Grant. We appreciate the entire team of Office of Global Health, University of Texas Southwestern Medical Center for the technical and administrative support. We are highly indebted to our study participants and research assistants for their involvement in this study. Also, we are grateful to the IGP, the Commissioner of Police FCT Command, and all Divisional Police Officers in Abuja for their support through the study period.
Data availability statement
Data collected and analyzed are stored in the University of Texas Southwestern Medical Center data repository system and are available upon justified request to the corresponding author.
Funding statement
This research was supported by the NIH Partnerships to Develop Injury Research Capacity in Sub-Saharan Africa grant (5D43TW010463-03).
Conflict(s) of interest
The authors report no conflicts of interest.










 Open access
Open access