



1. Background
Iraq experiences a high population growth rate. In the 1970s, it was above 3% per year, then it fell in the 1980s and resumed its rise in the 1990s (Ministry of Planning and National Population Commission (NPC), 2013). The conflicts that Iraq fought in during these times (The Iran-Iraq war from 1980-1988 and the Gulf War at the beginning of the 1990s) impacted the high population growth rate. By the end of the period 2009-2018, the population growth rate decreased to 2.1% according to national statistics by the Central Statistical Organization (CSO) of Iraq. Meanwhile, population policies encouraged childbearing to increase the population. However, the population growth rate did not decrease during 1997-2009; instead, it increased by 3% during these years (CSO, 2012).
Consequently, it had a negative impact on maternal and child health. Maternal mortality, neonatal mortality, and under-five mortality rates were high (Ministry of Planning and NPC, 2013). The high population growth also reduced population doubling times in Iraq. According to the NPC (2012), the population of Iraq doubled 12 times during the 20th century. Over the last 50 years, Iraq’s population has increased fourfold, doubling over the previous 25 years from 10 million in 1970 to 20 million in 1995 to approximately 40 million in 2020 (Ministry of Health, 2020).
The Iraqi population is the 4th largest among Arab countries (39.3 million), representing 9% of the Arab countries’ total population in 2019 (World Bank, 2020). According to a modest estimation, the United nation (UN) Population Division expected that the population of Iraq would reach 57.2 million by 2040. However, according to moderate and high estimations, it will reach 60.6 million and 63.9 million (double the population size in 2009), respectively (United Nations, Department of Economic and Social Affairs (UN-DESA, 2019).
Iraq is characterised by a very high total fertility rate (TFR), reaching 5.7 births per woman from 1990-1995. Then, it declined to 4.6 births per woman in 2011 (NPC, 2012) and continued to decrease to 3.6 births per woman, according to the Iraq Multiple Indicator Cluster Survey 2018 (IMICS 2018). Nevertheless, the country still experiences high fertility rates. It was ranked in the top six countries in the Arab world in terms of fertility rates and the second Arab country in adolescent birth rates in 2018 (World Bank, 2020).
According to IMICS data, the contraceptive prevalence rate (CPR) was approximately 43.6% among currently married Iraqi women in 2000. Approximately one-quarter of married Iraqi women used modern methods, and approximately one-fifth used traditional methods (Republic of Iraq Council of Ministers et al., 2001). The CPR continued to rise, reaching 49.8% in 2006, according to IMICS data (Central Organization for Statistics et al., 2007). However, between 2011 and 2018, the CPR plateaued at 52.5%-52.8% (CSO and Kurdistan Region Statistics Office (KRSO), 2012; CSO et al., 2019). Over time, currently married Iraqi women were more likely to use modern methods (36.1%). Concerning method mix, intrauterine devices (IUDs) and pills were the most popular methods during 2000-2018, as indicated by IMICS 2018.
According to UN-DESA (2020a), there was a decreasing trend in the percentage of unmet need for family planning (FP) from 1990 to 2020. First, it decreased from 24.1% in 1990 to 18.2% in 2000, and then it continued to decline in 2010 (13.2%). By 2020, it became 12.9%, almost half the reported percentage in 1990. Conversely, the demand satisfied for modern contraceptive methods constantly increased from 33.2% in 1990 to 45.5% in 2000 to 56.7% in 2020.
The Iraqi Ministry of Planning initiated the formation of the First Committee of the Population Policy in 1988. The committee was reformed by the ministry more than once. However, its activities were halted following events in 2003 (NPC, 2012). Before 2003, there was no explicit policy for reproductive health in Iraq because of the long periods of wars and conflicts. The government developed a plan to increase the population size to compensate for the human loss in these wars and conflicts (Ministry of Planning and NPC, 2013). This plan was confirmed as indicated by the 2013 World Population Policy Report (UN-DESA, 2013). Iraq under Saddam Hussein had a pronatalist policy that changed after the end of his regime.
The Iraq Family Planning Association played a central role in Iraq’s FP policies. All FP services were managed in coordination and cooperation with the Iraqi Ministry of Health. However, its role was minimized after 2003. In 2004, the Iraqi Ministry of Health developed the first strategic plan for maternal and child health (2005-2008). Even though it is uncertain to what extent women could access FP services, almost one-third of FP institutions have been destroyed since 2003 (Allami, Reference Allami2015 cited in Tull, Reference Tull2020). These institutions offer primary integrated and comprehensive services through the preventive and therapeutic fields. In addition, these institutions encourage breastfeeding, FP, and postnatal care, but to a lesser extent (Tull, Reference Tull2020). The first strategy was revised in 2009 and did not achieve many of its FP goals. Therefore, the next strategic plan for maternal and child health and reproductive health (2010-2015) listed FP among its priorities (Ministry of Planning and NPC, 2013) and implemented a new family health care system. An additional small number of centres was established in 2013. Between 2017 and 2020, Médecins du Monde (Doctors of the World, MdM) implemented sexual and reproductive health (SRH) services in Iraq (Tull, Reference Tull2020).
Iraq still aims to reduce population growth rates, which requires the expansion in contraceptive use, thus prompting the government to adopt the National Birth Spacing and Family Planning Strategy (2021-2025). The National Birth Spacing and Family Planning plan had three targets: to reduce the TFR to an average of 3.5 births per woman, reduce the adolescent birth rate to 60 births per 1000 adolescent girls, and reduce maternal mortality (a decrease of 0.9% yearly) by 2025. The plan suggested achieving these targets through the following goals by 2025: 1) increasing the proportion of women using modern contraceptive methods to approximately 45% or more, 2) decreasing traditional method use to less than 8%, 3) reducing the unmet need for modern methods from 24.3% in 2011 to 15%, 4) increasing satisfied demand for modern methods from 53.8% in 2018 to 75%, and 5) decreasing the percentage of couples declining FP methods use to 12% and 20% (Ministry of Health, 2020).
Many studies discussed FP programmes in Iraq. These studies could be categorised into three domains: (1) those concerned with knowledge of contraceptives and estimation of CPR and unmet need, (2) those studying the relation between the different background characteristics of women and contraceptive use and (3) those concerned with the determinants of using contraceptives.
The literature indicates that women in Iraq have sufficient knowledge about FP methods and suffer from many negative side effects of contraceptives—a primary reason for contraceptive discontinuation. According to a study performed in Duhok, north of Iraq, 2003 (Agha and Rasheed, Reference Agha and Rasheed2007), there has been a change in the method mix; modern methods became more common among women than traditional methods. Pills were the most commonly used method from 2011 to 2017, and pharmacies were the dominant contraceptive providers for Iraqi women (Ebrahim and Muhammed, Reference Ebrahim and Muhammed2011; Abd, Reference Abd2017; Al-Hamzawi and Al-Tameemi,Reference Al-Hamzawi and Al-Tameemi2020). The IUD became the most popular method, followed by pills in 2018, according to a study performed in the region of Mosul in Iraq (Aldabbagh and Al-Qazaz, Reference Aldabbagh and Al-Qazaz2020). Female sterilisation was less popular among Iraqi women and still is (Agha and Rasheed, Reference Agha and Rasheed2007; Ebrahim and Muhammad, Reference Ebrahim and Muhammed2011; Abd, Reference Abd2017; Aldabbagh and Al-Qazaz, Reference Aldabbagh and Al-Qazaz2020).
Characteristics play an essential role in determining the level of contraceptive use among women. The most important characteristic is age. Some studies have shown a significant relation between a woman’s current age, her educational level, and the use of contraceptives (Al-Azzawi et al., Reference Al-Azzawi, Salman and Hamid2005; Ebrahim and Muhammed, Reference Ebrahim and Muhammed2011; Ministry of Planning and NPC, 2013).
The Ministry of Planning and NPC (2013) performed a multivariate analysis and found that the most significant factors affecting contraceptive use in Iraq are the woman’s current age, age at first marriage, and number of living children. Moreover, the parent’s educational level, the stable income of the husband, place of residence, and the family type (nuclear or extended family) play an essential role. Therefore, a young woman (15-19 years) or older woman (45-49 years) who married at an older age, who has experienced the death of a child, has the lowest education level along with her husband, whose husband does not have a stable income, lives in a rural area, and lives in an extended family would have a low chance of using contraceptives.
Previous studies focused on simple descriptive analysis. These studies were limited to small sample sizes or cases of a specific region or territory. Increasing the prevalence of contraceptive use is one of the means to reduce TFR in the National Birth Spacing and Family Planning Strategy of Iraq. Therefore, there is a need to quantify the impact of demographic, fertility, socioeconomic, and cultural determinants that determine the use of traditional and modern contraceptives separately in Iraq.
Contraceptive use is affected by both supplies of FP services and demand factors. However, this study will focus on the demand factors that might affect contraceptive use in Iraq. The following variables were selected based on Iraqi and international evidence, as shown in Figure 1.
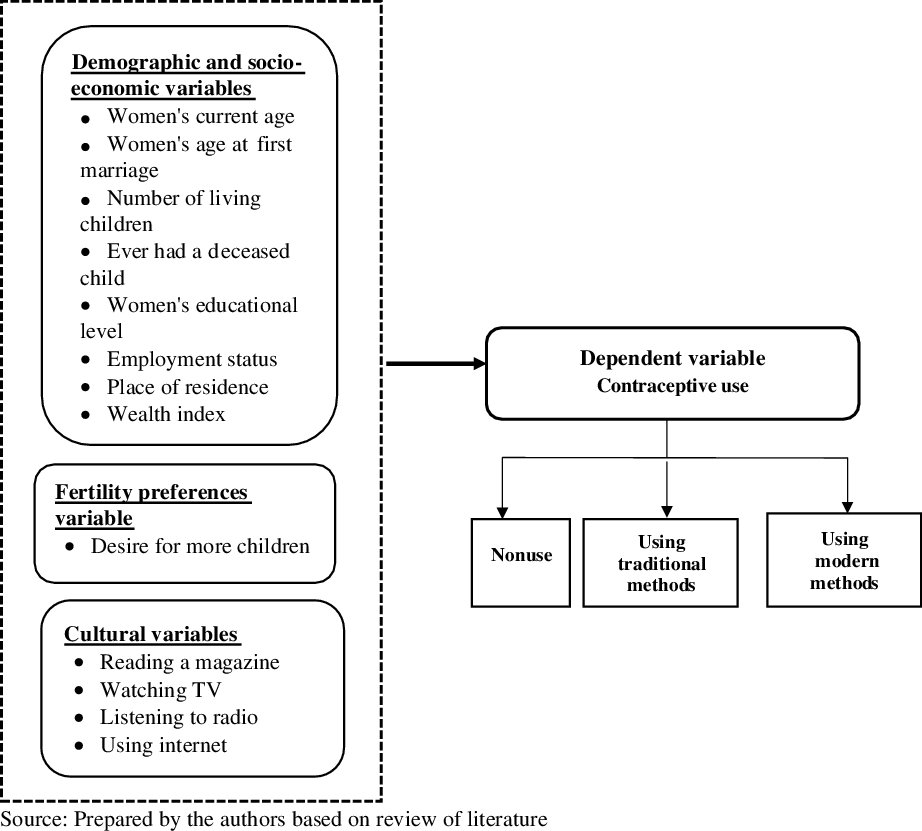
Figure 1. Theoretical framework of factors affecting contraceptive use in Iraq.
2. Data and Methods
2.1 Data
The study used data from the 2018 Iraq Multiple Indicator Cluster Survey carried out by the CSO and the KRSO in coordination with the ministries of health in the central and Kurdistan region and the technical and financial support of the United Nations Children’s Fund (UNICEF). The main objective of the IMICS 2018 was to provide estimates of various indicators about women’s and children’s health and the essential services for women and children at the national, regional, and governorate levels for urban and rural areas.
Out of 20,521 households selected for the IMICS 2018, 20,214 were successfully interviewed, representing a response rate of 99.5%. A total of 31,060 women were identified as eligible to be interviewed in IMICS 2018. Out of these women, 30,660 were successfully interviewed, representing a response rate of 98.7%.
The traditional methods reported by Iraqi women in IMICS 2018 included periodic abstinence and withdrawal, while modern methods included female sterilisation, male sterilisation, IUD, injectables, implants, pills, male condoms, female condoms, diaphragm, foam, jelly, and the contraceptive patch (CSO et al., 2018).
The study limited the analysis to currently married nonpregnant women aged 15-49 at the time of the survey. In addition, women who reported that they were infecund were excluded from the analysis. Therefore, the final sample size was 15,532 women.
2.2 Methods
Since the dependent variable (contraceptive use) has more than two outcomes, the study adopted a multiple multinomial logistic regression model to investigate the role of fertility preferences and the demographic, socioeconomic, and cultural determinants of contraceptive use among currently married nonpregnant Iraqi women in 2018.
2.3 Variables
2.3.1 Dependent variable
The outcome variable consists of three categories: not currently using a contraceptive method, currently using a traditional method, and currently using a modern method. The first category is the reference group.
2.3.2 The independent variables
The demographic and socioeconomic variables consist of 8 variables as follows: 1) Women’s current age, classified into seven categories: 15-19 years, 20-24 years, 25-29 years,…, 45-49 years; (2) Women’s age at first marriage, classified into four categories: less than 16 years, 16-20 years, 21-25 years, 26+ years; (3) Number of living children, classified into four categories: one child at most, 2, 3 and 4+; (4) Ever had a deceased child, classified into two categories: no/yes; (5) Women’s educational level, grouped into none or preprimary, primary, intermediate/lower secondary, and upper secondary education or above (upper secondary+); (6) Place of residence, classified into two groups: urban/rural; (7) Region, classified into two regions: Kurdistan and southern/central Iraq; and (8) Wealth index quintiles, grouped into three categories: low, middle, and high.
The fertility preferences variable is measured by the desire for more children and is classified into three categories: yes, no more children and undecided/do not know.
Cultural variables consist of two variables: mass media exposure and internet accessibility. (1) For mass media exposure, the study created a cumulative variable that expresses the exposure to different types of mass media, consisting of three categories. The value of mass media exposure ranges from 0 (no mass media exposure) to 2+ (women were exposed to at least two types of mass media). (2) Using the internet has two categories: no/yes.
2.4 Study Limitations
The analysis is limited in three respects. First, the IMICS is a cross-sectional survey; therefore, it tests association rather than causality. Second, the study could not test the association between women’s employment and contraceptive use because IMICS 2018 provided no information on women’s employment status. Additionally, the study examined the influence of exposure to mass media rather than FP messages, as information on the latter was missing.
3. Results
3.1 Bivariate associations between contraceptive use and the independent variables
As indicated by Table 1, close to half of the currently married Iraqi women (45.4%) were modern method users, 21% were traditional method users, and the rest were nonusers (approximately one-third). All the bivariate associations were statistically significant. More Iraqi women used modern methods among all categories except women who lived in Kurdistan and had at least one living child. The highest proportion of nonuse was observed among women who were younger (15-19), married late (age at first marriage was 26 years or more), had at least one living child, had not experienced the death of a child, and had a desire for more children. Additionally, they had less than primary education, belonged to the low wealth category, lived in rural southern/central Iraq, had no mass media exposure, and did not use the internet.
Table 1. The distribution of currently married nonpregnant women by contraceptive use and background characteristics, IMICS 2018

*P<.05, **P<.01, ***P<.001
The proportion of women using modern methods decreased as women’s age at first marriage and wealth index increased but increased with the number of living children and women’s current age except for the age category 40-44 years. Women with 4 or more living children, those with primary education or less, and those who had no desire for more children had the highest likelihood of using modern methods. Women who lived in southern/central Iraq used modern contraceptives more than those in Kurdistan. Regarding the place of residence, modern contraceptive methods were used over traditional methods in both rural and urban areas. Women exposed to one type of mass media had the highest proportion of using modern methods. Concerning traditional methods, the likelihood of their use increased as women’s current age increased until age 35; women’s age at first marriage increased except for the last category; and education, wealth, and mass media exposure increased.
3.2 Reproductive intentions
Table 2 presents the reproductive intentions of currently married Iraqi women at the time of the survey according to their number of living children. Slightly more than half did not want any more children, 40% of them desired to have another child, and the rest were undecided. As expected, the desire for no more children is strongly related to the women’s number of living children. Women with three or more living children were less likely to desire more children. In contrast, women with two children were more likely to desire more children than other women. Almost all women with no living children (96%) desired a child. On the other hand, more women with four or more children wanted no more children (82.9%).
Table 2. Percent distribution of currently married nonpregnant women by desire for more children according to number of living children, IMICS 2018

3.3 Determinants of modern and traditional contraceptive use
Table 3 summarises the multinomial logistic regression models of traditional and modern contraceptive methods on selected demographic, socioeconomic, and cultural variables, and fertility preferences. The results are presented as relative risk ratios (RRRs) (unadjusted and adjusted) and their respective confidence intervals.
Table 3. RRRs of contraceptive use among currently married nonpregnant women aged 15-49, IMICS 2018

Reference categories: number of living children (one child at most), ever had a deceased child (no), women’s age at first marriage (26+ years); education level (none or preprimary); desire for more children (yes); mass media exposure (zero); internet use (no); place of residence (rural); region (southern/central Iraq); and wealth (low).
*P<.05, **P<.01, ***P<.001
For unadjusted RRRs, each explanatory variable is the only predictor in the multinomial regression model. On the other hand, adjusted RRRs control for multiple factors in the multinomial regression model. All explanatory variables are included in the adjusted model except for women’s current age. In all explanatory variables, the results indicated a difference between the unadjusted and adjusted RRR but at a different pace. The adjusted and unadjusted RRRs of the explanatory variables were in the same direction, except for three variables: (1) women with experience of child death, (2) the last category of women’s level of education, and (3) internet use. The first two were influenced by the desire for more children (RRR was reversed). In the descriptive analysis, modern method use was lowest among women who received at least upper secondary education. However, this group became significantly more likely to use modern methods than nonuser women with limited schooling in the adjusted model. Additionally, women with experience of child death became less likely to use modern methods than women without child death experience. Finally, women who used the internet became more likely to use modern methods after adding the number of living children within the other controlling variables.
The main findings of the adjusted model indicated that there was a strong positive association between using either traditional or modern contraceptive methods and the number of living children. However, women who had only one live child were less likely to use either contraceptive method than other women.
The experience of having a deceased child had a significant negative impact on traditional and modern contraceptive use. Women who had experienced the death of a child had 25% and 34% lower risks of using traditional and modern contraceptives, respectively, compared with women who had not. In addition, increasing the age at first marriage had a negative impact on modern method use. Compared to women who were first married after 25 years old, women who first married before age 16 and between age 16-20 had double the risk of using modern methods. Women who were first married between ages 16-20 were the most likely to use a traditional method. Women who were first married after 25 years old were significantly less likely to use any method.
The results indicated that women’s education was significantly related to the use of traditional methods and modern methods. As women’s educational level increased, the likelihood of using traditional contraceptive methods also increased. Women with primary and intermediate/lower secondary education had a risk of using traditional methods 1.5 times and 1.9 times more than women who had less than primary education, respectively. There was an almost 1.20 times higher risk of modern method use among women with primary education and women with intermediate/lower secondary education compared with women with limited schooling. Women who received at least upper secondary education had the highest risk of using both methods compared with other women. They had 2.5 times and 1.6 times higher risk of using traditional and modern methods, respectively.
Women who declared their desire for no more children were more likely to use traditional and modern contraceptive methods. On the other hand, women who reported being undecided or did not know had a risk of using traditional and modern contraceptive methods 1.7 times and 1.4 times that of women who declared their desire for more children.
Exposure to mass media and access to the internet positively influenced contraceptive use. Women who had no media exposure had the lowest risk of using traditional and modern contraceptive methods compared with other categories. Women exposed to only one type of mass media had an approximately 1.6 times higher risk of using traditional or modern contraceptive methods. Exposure to at least two types of mass media increased the risk of using traditional or modern contraceptive methods by approximately 1.7 times. Women who had internet access had 1.5 times and 1.1 times the risk of using traditional and modern contraceptive methods, respectively.
The results indicated that the use of traditional and modern contraceptive methods varies by region. Women living in urban areas had a 1.2 times higher risk of using a modern method than rural residents. Women who lived in Kurdistan were more likely to use traditional and modern methods than women living in southern/central Iraq. Living in Kurdistan increased the risk of using traditional and modern contraceptive methods by 6.2 times and 1.3 times, respectively.
There was no difference in the risk of using traditional methods with wealth. However, for modern methods, the risk of using contraceptives did not differ between women in the middle and low categories of wealth, while women in the high wealth category had an 11% lower risk of using contraceptives than women in the low wealth category.
4. Discussion and Conclusion
Iraq is committed to the Sustainable Development Goals (SDGs 3 & 5). One of the SDGs-2030 is to ensure universal access to sexual and reproductive health care services, including FP services, information, and education, as well as the integration of reproductive health into national strategies and programmes by 2030 (Target No. 3-7). The two measures of progress for this target are the proportion of women of reproductive age who have satisfied their need for FP through modern methods and the adolescent birth rate (aged 10-14 years; aged 15-19 years) per 1,000 girls and women in that age group (UN-DESA, 2020b).
Iraq experiences high fertility rates, especially among adolescents. Increasing the prevalence of modern contraceptive method use to approximately 45% or more and reducing the use of traditional methods to less than 8% by 2025 are identified as essential tools for achieving the target of the Iraqi National Birth Spacing and Family Planning Strategy (2021-2025), which aims to decrease TFR to an average of 3.5 births per woman in 2025.
The level of contraceptive use is one of the primary proximate determinants of fertility level. A comparative study focusing on fertility and FP among all women (UN-DESA, 2020b), which included data from 185 countries or areas, reported an inverse relationship between contraceptive use and the fertility level in all countries studied, and Iraq is no exception.
Within the context of high fertility in Iraq, this paper identified traditional and modern contraceptive use determinants among currently married nonpregnant Iraqi women. The study applied the multiple multinomial logistic regression model based on IMICS 2018 data. The study’s main findings indicated a strong positive association between the number of living children and the use of contraceptive methods, which is in line with previous studies (Imran et al., Reference Imran, Nasir and Zaidi2015; Ajmal et al., Reference Ajmal, Idris and Ajmal2018; Riese and Juan, Reference Riese and Juan2020).
Several studies have confirmed the negative impact of child mortality experience on fertility (Kabir et al., Reference Kabir, Jahan, Islam and Ali2001; Fitaw et al., Reference Fitaw, Berhane and Worku2004) and contraceptive use (Osmani et al., Reference Osmani, Reyer, Osmani and Hamajima2015; Solanke, Reference Solanke2017). Although the child mortality variable is available in many survey data, such as the IMICS and Demographic and Health Survey (DHS), statistical modelling rarely examines its impact on contraceptive use. Our study findings confirmed its association with the use of traditional and modern methods.
The likelihood of using traditional contraceptive methods increased with women’s age at first marriage until age 20, after which it reverted to a decreasing trend. The highest risk of using modern contraceptive methods was among women who were first married before age 21. Only the minority of women who were first married at 26+ years had significantly lower use levels than the other categories of women marrying at other ages. Women who marry late are more educated and empowered and thus are assumed to be more likely to use contraception than women who marry early. Therefore, this minority must have shorter marriage durations than the other categories. Nevertheless, the lower RRRs of use methods among women who marry late was contrary to our expectations and remains unexplained.
The descriptive analysis showed that there were high levels of modern method use among women with minimal schooling. Approximately 47% of those with no or preprimary schooling used modern methods, suggesting that limited schooling is not a significant barrier. In the multivariate analysis, higher levels of education had a positive and statistically significant influence on the risk of using traditional contraceptive methods. However, women who received at least upper secondary education had a significantly higher risk of using modern contraceptive methods. However, this risk was lower than using traditional contraceptive methods among these women. This implies that better-educated women, compared with women with limited schooling, prefer to use traditional contraceptive methods rather than modern methods.
The most interesting result is that there were small adjusted associations of household wealth and residence (rural/urban) with modern method use versus nonuse. Thus, modern method use is widely dispersed across these different socioeconomic strata. Access to FP services does not appear to be a problem for rural and poor women.
Not surprisingly, there were regional differences in contraceptive use in Iraq. The Kurdistan region has experienced very different conditions compared with the rest of Iraq. It witnessed virtually no violence during the 2003 United States-led invasion. Eventually, it enjoyed a better security environment in subsequent years. Kurdish families currently enjoy an adequate living standard (KRSO et al., 2018). As a result, Kurdistan has better fertility and FP indicators than southern/central Iraq. Its TFR and adolescent birth rate were 3.1 births per woman and 40 births per 1000 girls, respectively, compared with 3.8 births per woman and 77 births per 1000 girls, respectively, in south-central Iraq. Additionally, Kurdish women have a higher CPR (66.6%) and a lower unmet need (8%) versus 49.8% and 15.7%, respectively, among their south-central Iraqi counterparts. Moreover, the study estimated a trivariate percent distribution of contraceptive use by education and region and wealth and region. In contrast to our assumptions, the results indicated that the more educated and wealthy women were, the more likely they were to use traditional contraceptive methods than modern methods or nonuse (results are available upon request). Consequently, it might be challenging to achieve the target of reducing the use of traditional methods in the strategic plan of Iraq. The association of traditional method use with higher education and residence in Kurdistan is a matter of choice rather than access problems. Iraq is not unique in this regard. Similar findings have been reported in India (Basu, Reference Basu2005), Iran (Erfani and Yuksel-Kaptanoglu, Reference Erfani and Yuksel-Kaptanoglu2012), and Sri Lanka (Perera, Reference Perera2014). Basu (Reference Basu2005) proxied upper-class women by their college education and residence in urban areas. She mentioned that they might face more facilitating conditions for using traditional methods. Better husband/wife communication is essential for effective birth control, especially when using traditional methods that require spousal cooperation. She offered another explanation about the contraceptive behaviour of urban college-educated women. According to her, they might be married later than other women, and thus they might be less worried about contraceptive method effectiveness at an earlier stage of their childbearing experience. Additionally, Basu showed that much higher prevalence levels of traditional methods were found in urban than in rural areas and among the highest educated groups in India. Erfani and Yuksel-Kaptanoglu (Reference Erfani and Yuksel-Kaptanoglu2012) pointed out that among the wealthier and more educated users in Iran, awareness, fear of the side effects of modern methods (especially the pill), and greater spousal cooperation are among the main reasons they prefer withdrawal over modern methods. Perera (Reference Perera2014) indicated that traditional method use was relatively higher among educated women than less educated women in Sri Lanka.
It is worth noting that the contribution of the governmental sector in providing FP services was limited (NPC, 2012; Shabila et al., Reference Shabila, Ahmed and Yasin2014; Ministry of Health, 2020). Undoubtedly, motivating Iraqi women to receive maternity care services, especially FP, from the public sector and improving interpersonal communication with health care providers in this sector will eventually raise the prevalence of contraceptive method use.
Furthermore, mass media and the internet are additional sources of information and communication, which are expected to limit the knowledge gap about FP methods and services. However, the influence of internet access on contraceptive use has rarely been examined, and the most examined variable is mass media exposure. This study found that mass media exposure and internet use positively affected contraceptive use. In addition, there was a strong adjusted association of media exposure with traditional and modern method use.
It is worth mentioning that three pieces of information were missing in the dataset used: women’s employment status, occupation, and work sector. Therefore, the study was not able to examine their impact on contraceptive use. However, it is expected that improving education and increasing the participation of women in the labour force will strengthen women’s economic position and empower their independence; consequently, they will have the awareness and motivation to use contraceptives.
Contraceptive prevalence, unmet need, and contraceptive discontinuation are considered FP core indicators (United States Agency for International Development (USAID), 2021). However, more research is required to explore the role of unmet need, either for spacing or limiting births, in hampering Iraqi efforts to reduce the TFR. Additionally, studies on FP in Iraq lack other dimensions, notably the discontinuation of contraceptive use.
Through creative and innovative campaigns, FP programme efforts should motivate well-educated women to expand their choices of FP methods and become modern method users rather than traditional users. Therefore, the FP programme should exert more effort to enhance interpersonal communication between health service providers and contraceptive users, in addition to providing better counselling to reduce avoidable health concerns and side effects among modern method users.
Additionally, more advocates of FP programmes should be directed to women who live in the southern/central areas of Iraq, as they were the least expected to use contraceptives. Additionally, FP programmes should motivate Iraqi women to use modern contraceptives rather than traditional contraceptives, especially those who live in Kurdistan.
Funding
This research received no specific grant from any funding agency, commercial entity, or not-for-profit organisation.
Conflicts of Interest
The author has no conflicts of interest to declare.
Ethical Approval
The author asserts that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.




