



A 38-year-old woman with cyanosis of unknown cause resulting from hypoxaemia was referred to our hospital. She had a history of cyanosis of the finger since teenager and general fatigue; however, the cause was not clear. Her oxygen saturation on admission was 91% in room air and arterial blood gases showed significant hypoxaemia (PO2, 57.8 mmHg). Transesophageal echocardiography revealed a secundum 18 × 12 mm atrial septal defect (Fig 1). Additionally, an abnormal mass in the right atrium was diagnosed as prominent crista terminalis (Fig 1). Doppler flow through the atrial septal defect showed bidirectional interatrial shunt (Fig 2). The abnormal structure was involved in directing the flow toward the left atrium (Fig 3, Videos 1 and 2). Right-heart catheter examination showed no pulmonary hypertension. A contrast-enhanced chest CT showed no evidence of pulmonary arteriovenous fistula or thrombus. A 44-mm GORE CARDIOFORM ASD Occluder (GORE) was deployed with no residual shunt flow (Fig 4). After deployment, the patient’s oxygen saturation immediately improved to 100%, and her cyanosis resolved.

Figure 1. Transesophageal echocardiography showing a single secundum atrial septal defect and prominent crista terminalis (red arrow). RA, right atrium; LA, left atrium; Ao, aorta; SVC, superior vena cava.
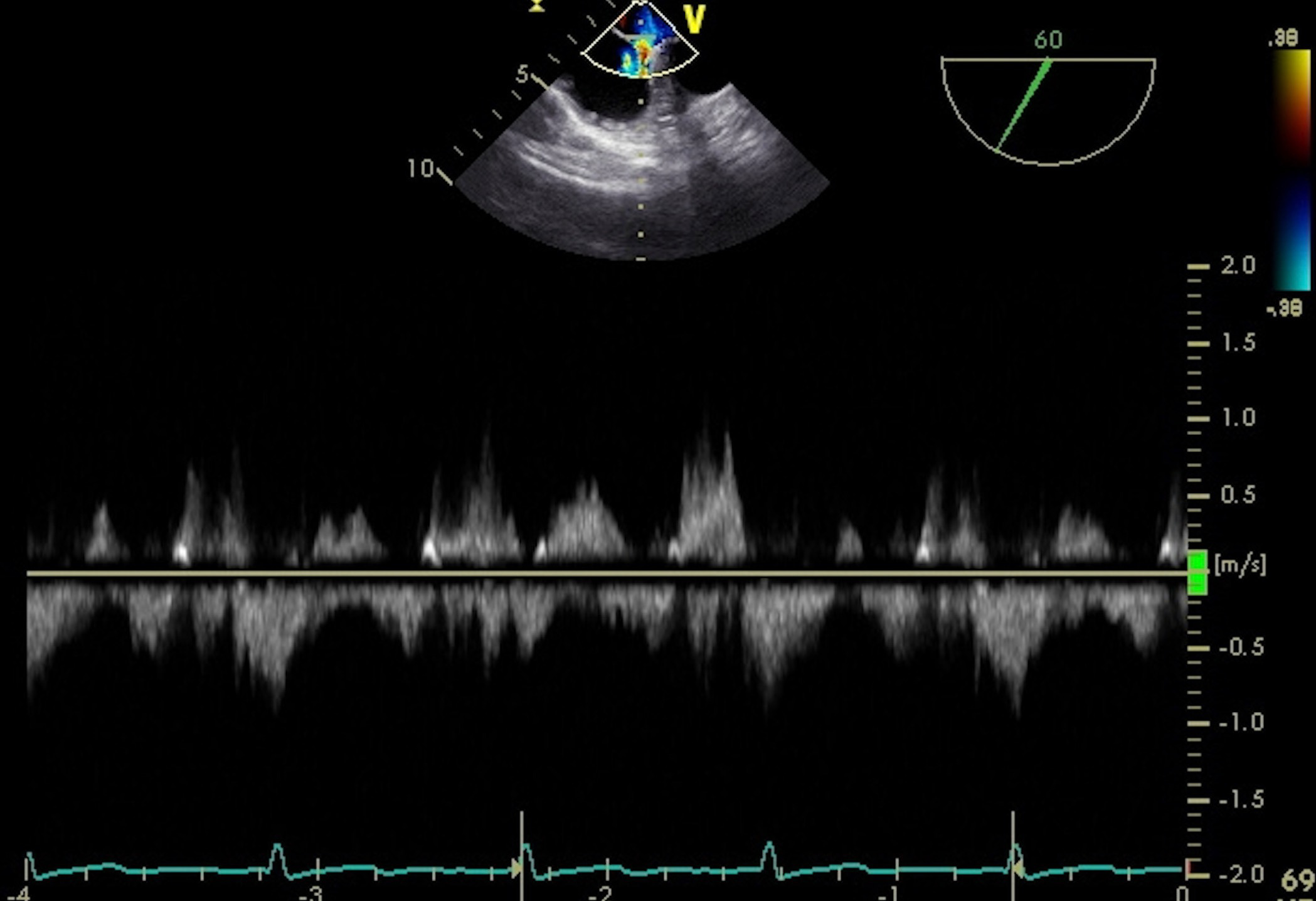
Figure 2. Doppler flow on preprocedural transesophageal echocardiography through the atrial septal defect showing bidirectional interatrial shunt.
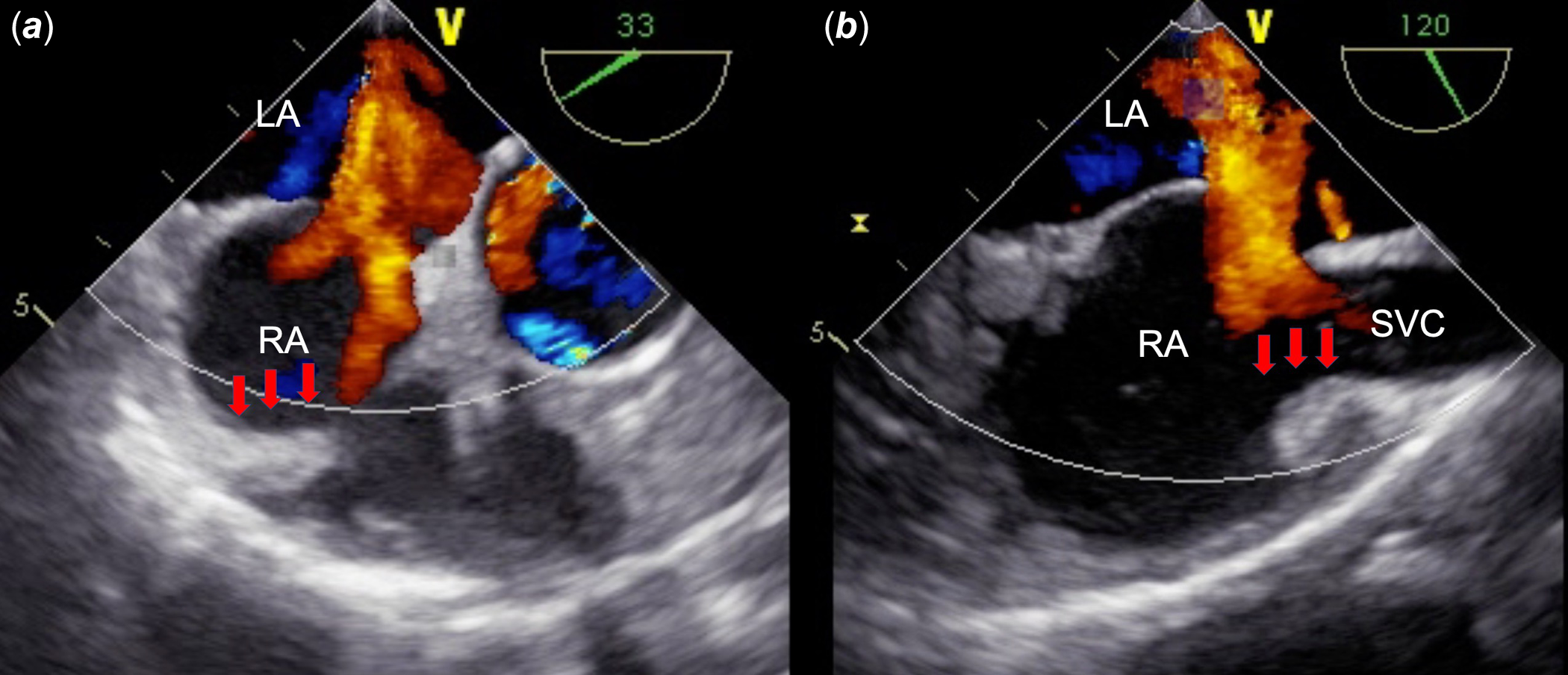
Figure 3. Preprocedural transesophageal echocardiography showing that prominent crista terminalis is involved in directing the flow toward the left atrium. RA, right atrium; LA, left atrium; Ao, aorta; SVC, superior vena cava.
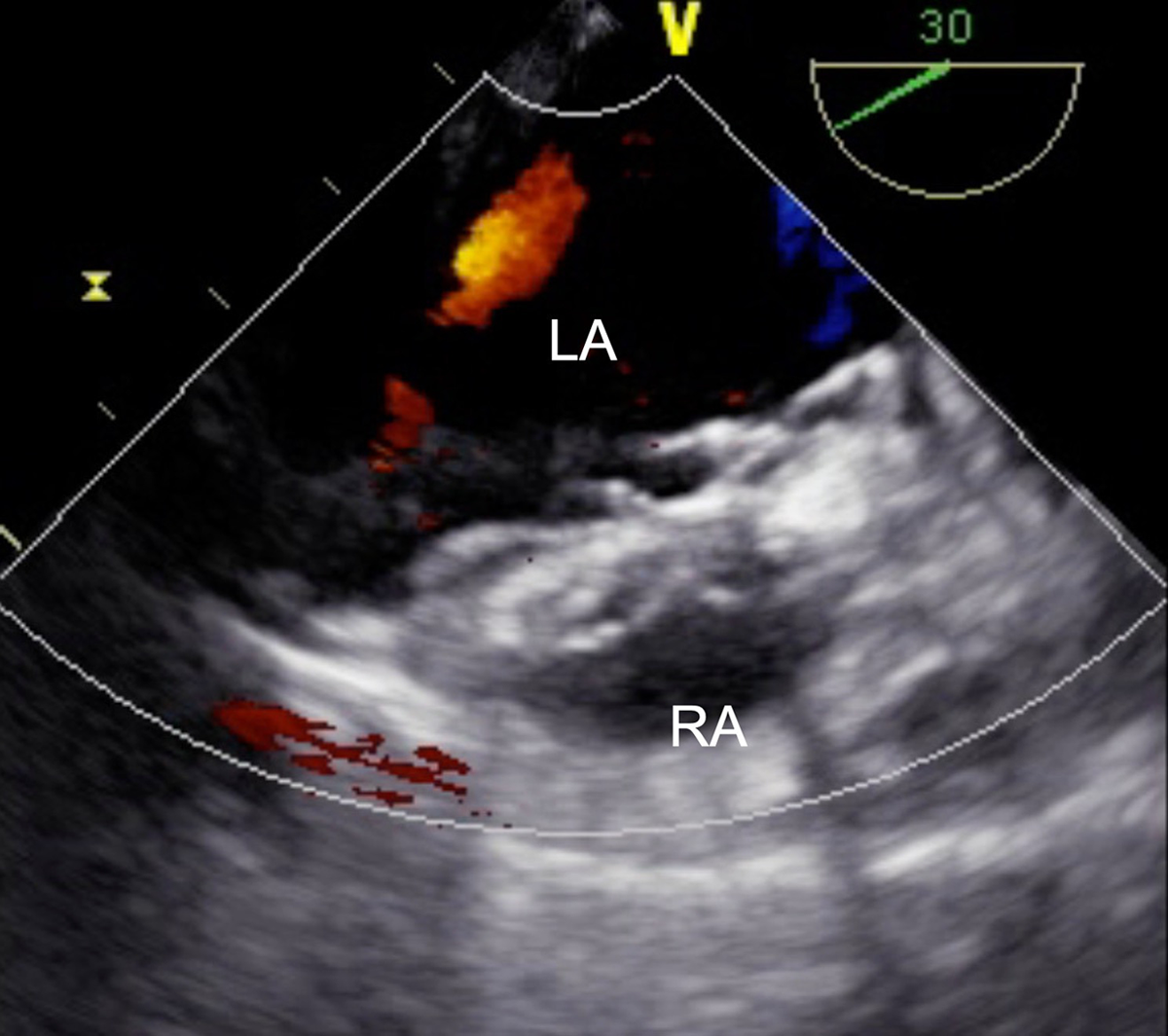
Figure 4. A 44-mm GORE CARDIOFORM ASD Occluder is successfully deployed with completely no residual shunt flow. RA, right atrium; LA, left atrium.
Right-to-left shunt in atrial septal defect without pulmonary hypertension is a rare condition and can present with complications such as cyanosis. In general, cyanosis in the setting of high pulmonary vascular resistance (Eisenmenger syndrome) is well-known. However, cyanosis in some cases is not associated to high pulmonary vascular resistance. Crista terminalis is known to be normal anatomical variant; however, this structure can vary considerably in thickness and depth. Reference Hahn, Abraham and Adams1 This is a rare case of cyanosis caused by right-to-left shunt atrial septal defect related to prominent crista terminalis.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951122004255
Acknowledgement
None.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of interest
None.
Ethical standards
All study procedures complied with the ethical standards of the Helsinki Declaration.





