



Introduction
Adhesive otitis media is adhesion of the tympanic membrane to the cochlear promontory and/or ossicles. It occurs as a sequela of long-standing inadequate ventilation of the middle ear.Reference Doğru, Tüz, Uygur, Candir and Yariktaş1 The functions of the Eustachian tube include ventilation of the middle ear, drainage of secretions and protection against pathological micro-organisms.Reference Sudhoff and Mueller2 Inadequate ventilation of the middle ear results from abnormal function of the Eustachian tube.Reference Djalilian and Paparella3 Chronic dysfunction of the Eustachian tube leads to progressive adhesion of the tympanic membrane to the medial wall of the middle-ear cavity and ossicular chains, resulting in fibrosis and progression to adhesive otitis media.Reference Sadé4
Adhesive otitis media accounts for 3–5 per cent of all chronic otitis media cases.Reference Dommerby and Tos5 Irreversible adhesion and fibrosis of the middle ear in adhesive otitis media results in significant hearing loss, tinnitus, ear fullness and otorrhoea.Reference Doğru, Tüz, Uygur, Candir and Yariktaş1,Reference Si, Chen, Xu, Chen, He and Zhang6 The diagnosis of adhesive otitis media is established during otomicroscopic examination by permanent tympanic membrane retraction and adhesion to the medial wall of the middle-ear cavity, confirmed with the Valsalva manoeuvre.Reference Larem, Haidar, Alsaadi, Abdulkarim, Abdulraheem and Sheta7 Audiological assessment also helps in establishing the diagnosis.Reference Si, Chen, Xu, Chen, He and Zhang6
Several factors contribute to the pathogenesis of adhesive otitis media, including dysfunction of the Eustachian tube, degree of mastoid pneumatisation, variations of the compartments and folds in the middle ear, variations in craniofacial development, and middle-ear cavity size.Reference Satar, Hidir and Coskun8–Reference Ruah, Schachern, Paparella and Zelterman10 Eustachian tube dysfunction is the most critical cause in the pathogenesis of adhesive otitis media, leading to negative pressure in the tympanic cavity, and resulting in the invagination and adhesion of the tympanic membrane to the medial wall of the middle-ear cavity.Reference Tos11,Reference Sadé and Berco12 Variations in petrous bone angles, including the petroclival and Eustachian tube–tympanic cavity ventilation angles, can indicate relatively less pneumatisation of the mastoid and small middle-ear cavity, which portends greater susceptibility to the adhesion process.Reference Satar, Hidir and Coskun8
An effective treatment, balloon Eustachian tuboplasty, was recently introduced to treat patients with obstructive Eustachian tube dysfunction.Reference Plaza, Navarro, Alfaro, Sandoval and Marco13 Balloon Eustachian tuboplasty can be performed to improve Eustachian tube function in patients with adhesive otitis media. However, there have been no defined parameters for Eustachian tube dysfunction and ventilation for planning appropriate surgical techniques. This study aimed to investigate the parameters for adequate ventilation through the Eustachian tube in adhesive otitis media ears on computed tomography (CT).
Methods
Patients
This study included 26 patients with a mean (± standard deviation (SD)) age of 47.2 ± 17.3 years, who were diagnosed with unilateral adhesive otitis media at hospital between January 2016 and December 2020. Their healthy side was used as the control. Adhesive otitis media was diagnosed when one or more tympanic membrane quadrants adhered to the cochlear promontory and/or ossicles. The diagnosis was established based on otomicroscopy, audiometry and temporal bone CT findings. Patients with craniofacial anomalies, temporal bone trauma history or tympanic membrane perforation were excluded. The institutional review board at the hospital approved the study (approval number: 2021-08-024), and informed consent was exempted.
Computed tomography scan
All patients underwent multi-detector CT scanning to evaluate further the anatomical nature of the temporal bone and the extent of the disease. The CT imaging was performed with Toshiba Aquilion One scanner (Canon Medical Systems, Tochigi, Japan) with the following settings: 135 kVp tube voltage, 300 mA tube current, 22 mm field of view, 4000 HU window width, 1000 HU window level, 0.5 mm slice thickness and 0.25 mm slice interval.
Measurements
The radiological measurements were performed retrospectively. The Eustachian tube length was measured as a straight line between the tympanic and pharyngeal orifices of the Eustachian tube on axial CT. The tympanic orifice was identified at the cochlear basal turn level, and then the point of measurement was adjusted to be at the centre of the tympanic orifice. The pharyngeal orifice was identified lateral to the torus tubarius, and the orifice was adjusted to be at the level of the torus tubarius tip. After that, the axial CT section was moved until both points of measurement (tympanic and pharyngeal orifices) appeared in the same section; the length was measured in millimetres (Figure 1).Reference Janzen-Senn, Schuon, Tavassol, Lenarz and Paasche14,Reference Falkenberg-Jensen, Hopp, Jablonski, Pripp and Silvola15 The connection of fibrocartilaginous and osseous portions of the Eustachian tube on the axial CT section was identified. The most irregular and narrowest part of the Eustachian tube was considered the diameter, measured in millimetres (Figure 2).Reference Paltura, Can, Yilmaz, Dinç, Develioğlu and Külekçi16
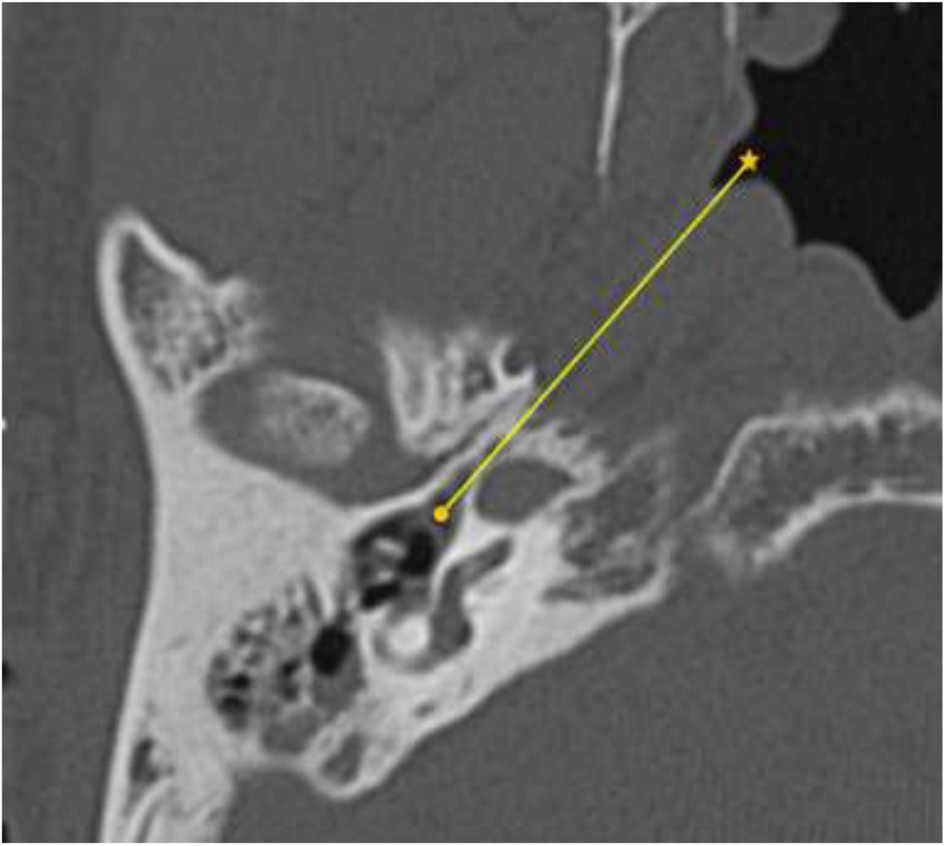
Fig. 1. Eustachian tube length was measured as a straight line between the tympanic and pharyngeal orifices of the Eustachian tube on an axial computed tomography scan (● = tympanic orifice, ★ = pharyngeal orifice).

Fig. 2. An Yellow line (arrow) on an axial computed tomography scan shows the narrowest section of the bony portion of the Eustachian tube.
In order to assess mastoid pneumatisation and middle-ear formation by the Eustachian tube function, the petroclival and Eustachian tube–tympanic cavity ventilation angles were measured. The petroclival angle was described as the angle between the midsagittal line passing through the sphenoid crest and protuberantia occipitalis interna and the other line starting from the midclivus and passing through the posterior surface of the petrous bone at the internal auditory canal level that appeared widest (Figure 3). The Eustachian tube–tympanic cavity ventilation angle was defined as the angle between a longitudinal axis through the Eustachian tube–tympanic orifice and the tangential line to the external auditory canal posterior bony wall (Figure 4).Reference Satar, Hidir and Coskun8

Fig. 3. The petroclival angle was measured on an axial computed tomography scan between the midsagittal line (a line on the sphenoid crest through nasal septal bone and protuberantia occipitalis interna) and the other line passing into the posterior surface of the petrous bone at the level of the internal auditory canal.
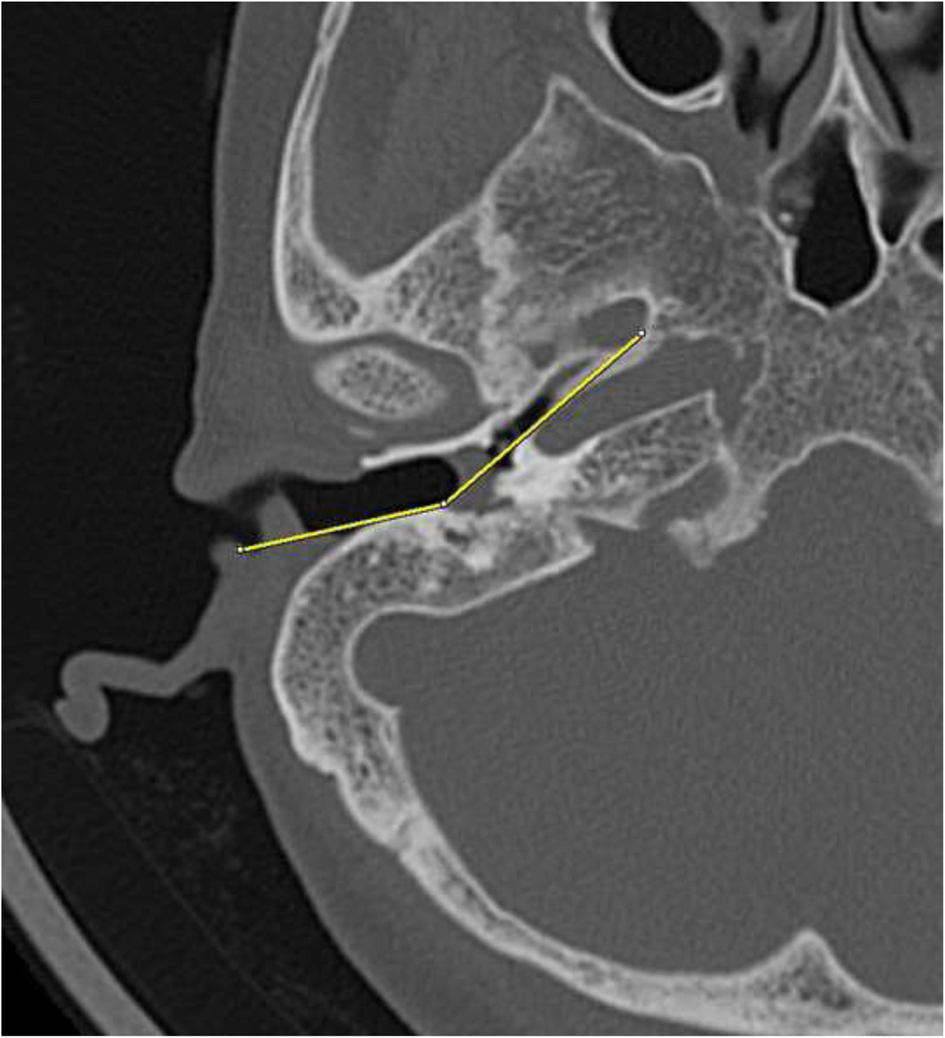
Fig. 4. The Eustachian tube–tympanic cavity ventilation angle was measured on an axial computed tomography scan. The angle was defined between a line through the posterior lip of the tympanic orifice of the Eustachian tube and the other line to the posterior bony wall of the external auditory canal.
The measurements were carried out bilaterally in both adhesive otitis media and healthy ears by one radiologist and one otologist, and the results were compared between adhesive otitis media and healthy ears.
Statistical analysis
The data were analysed with Stata statistical software, version 17 (StataCorp, College Station, Texas, USA), and presented as numbers (percentages) for categorical variables, and as means (± SDs) for continuous variables. Comparison between continuous variables was performed using independent t-tests. A p-value of less than 0.05 was considered statistically significant.
Results
Of the 26 patients diagnosed with unilateral adhesive otitis media, 13 (50 per cent) were male and 13 (50 per cent) were female. The mean age was 47.2 ± 17.3 years (range, 9–72 years). The unilateral adhesive otitis media was right- and left-sided in 15 (57.69 per cent) and 11 (42.31 per cent) patients, respectively.
The Eustachian tube length in adhesive otitis media and healthy ears was 38.4 ± 2.5 mm and 38.9 ± 3.1 mm, respectively. The difference between the two groups was not statistically significant (p = 0.528). The diameter of the Eustachian tube in adhesive otitis media and healthy ears was 1.47 ± 0.44 mm and 1.83 ± 0.58 mm, respectively. The diameter of the Eustachian tube in adhesive otitis media ears was significantly narrower than in healthy ears (p = 0.018) (Table 1).
Table 1. CT parameters for Eustachian tube ventilation*
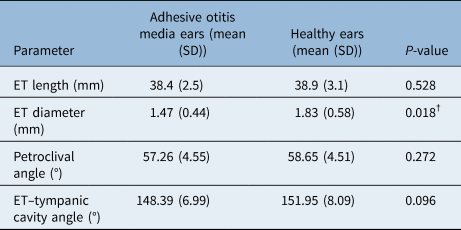
*Comparison between adhesive otitis media ears and healthy ears. †Indicates significant difference (p < 0.05). CT = computed tomography; SD = standard deviation; ET = Eustachian tube
The petroclival angle in adhesive otitis media and healthy ears was 57.26 ± 4.55° and 58.65 ± 4.51°, respectively. The Eustachian tube–tympanic cavity ventilation angle was 148.39 ± 6.99° in adhesive otitis media ears and 151.95 ± 8.09° in healthy ears. There was no statistical difference in the petroclival angle (p = 0.272) or the Eustachian tube–tympanic cavity ventilation angle (p = 0.096) between adhesive otitis media and healthy ears.
Discussion
Various craniofacial measurements have been studied in relation to otitis media. In a cadaver study, a short Eustachian tube, interaural length, and distance between the midsella and staphylion were associated with otitis media.Reference Todd17 Another study using lateral cephalography reported that the bony Eustachian tube, the vertical portion of the tensor veli palatini muscle, and the mastoid air cell system were smaller in secretory otitis media cases than in controls.Reference Kemaloğlu, Göksu, Ozbilen and Akyildiz18 Additionally, the length of the anterior skull base, the angle between the anterior and medial skull base, upper facial height, and maxillary depth on lateral cephalography have been reported as predictive factors for otitis media.Reference Di Francesco, Sampaio and Bento19
The length and angle of the Eustachian tube can be precisely measured using CT. A straight measurement between the tympanic and pharyngeal orifices is an appropriate and straightforward method to assess Eustachian tube length. The length of the Eustachian tube is 37.0 ± 4.16 mm in adults, while the Eustachian tube angle is 45° and 10° in adults and infants, respectively.Reference Ishijima, Sando, Balaban, Suzuki and Takasaki20,Reference Dinç, Damar, Uğur, Öz, Eliçora and Bişkin21 We investigated a straight line between the tympanic and pharyngeal orifices to measure the length of the Eustachian tube. The average length in adhesive otitis media and healthy ears was 38.4 mm and 38.9 mm, respectively. There was no difference in Eustachian tube length between adhesive otitis media and healthy ears. This finding is consistent with that of Dinç et al.,Reference Dinç, Damar, Uğur, Öz, Eliçora and Bişkin21 who reported no difference in Eustachian tube length between the chronic otitis media and healthy sides. In addition, Takasaki et al.Reference Takasaki, Takahashi, Miyamoto, Yoshida, Yamamoto-Fukuda and Enatsu22 reported Eustachian tube length and angle using multiplanar reconstruction CT in children with and without secretory otitis media. No difference was found in the length and angle of the Eustachian tube, suggesting that a short and horizontal Eustachian tube might not be a main aetiological factor for developing otitis media in children.
In our study, the CT axial section was used to measure the Eustachian tube diameter to find any contribution in patients with unilateral adhesive otitis media. This measurement is relatively simple, easy and non-time-consuming, and can be performed routinely on a temporal bone CT scan. The diameter of the Eustachian tube was narrower in adhesive otitis media ears than in healthy ears, indicating a positive correlation between Eustachian tube diameter and adhesive otitis media development. Despite different ear pathology, this result is consistent with a study by Paltura et al., where they found a smaller bony Eustachian tube diameter in chronic otitis media patients.Reference Paltura, Can, Yilmaz, Dinç, Develioğlu and Külekçi16 Shim et al.Reference Shim, Choi, Yoon, Kwon and Yeo23 reported that a larger cross-sectional area of the Eustachian tube on pre-operative coronal CT was associated with better post-operative results. According to the results of this study, the diameter of the Eustachian tube can be used to choose the appropriate surgical technique with or without Eustachian tube dilatation, and to predict the surgical outcomes.
Balloon Eustachian tuboplasty is a novel treatment procedure for Eustachian tube dilatory dysfunction. Balloon Eustachian tuboplasty treatment improved Eustachian tube ventilation in patients with mild to moderate atelectasis (Sadé grade I and II).Reference Plaza, Navarro, Alfaro, Sandoval and Marco13 Eustachian tube score was improved in patients with adhesive otitis media who underwent balloon Eustachian tuboplasty with cartilage tympanoplasty, compared with those undergoing cartilage tympanoplasty alone.Reference Si, Chen, Xu, Chen, He and Zhang6 Balloon Eustachian tuboplasty treatment also reduced tympanic membrane retraction in children with chronic otitis media with effusion.Reference Tisch, Maier, Preyer, Kourtidis, Lehnerdt and Winterhoff24
The petroclival and Eustachian tube–tympanic cavity ventilation angles have been reported to be more acute in adhesive otitis media.Reference Satar, Hidir and Coskun8 However, we did not find any difference between the adhesive otitis media and healthy ears. We investigated the angles using the healthy side in the unilateral adhesive otitis media patients as the control, while the other study investigated different healthy participants as the controls. This difference in the study participants may have contributed to the differences in the results. However, Sirikci et al.Reference Sirikci, Bayazit, Bayram and Kanlikama25 examined the Eustachian tube angle in chronic otitis media cases, and did not find any difference in the angles between disease and control groups.
• Eustachian tube diameter in adhesive otitis media ears was significantly narrower than in healthy ears
• Measuring Eustachian tube diameter is simple
• This measurement can be routinely performed when examining temporal bone computed tomography scans for Eustachian tube function evaluation
• Eustachian tube diameter measurement can be used to plan appropriate surgical techniques
Dynamic imaging and cine techniques of the Eustachian tube using four-dimensional CT have been reported to evaluate the dynamic changes between the open and closed states of the Eustachian tube.Reference Jufas, Deveau and Bance26,Reference Smith, Scoffings and Tysome27 We investigated the parameters of conventional CT imaging, which offers no insight into dynamic changes of the Eustachian tube. Further studies are necessary to evaluate the dynamic function of the Eustachian tube in patients with adhesive otitis media.
Conclusion
The diameter of the Eustachian tube was significantly narrower in the adhesive otitis media ears and was associated with developing adhesive otitis media. Measuring Eustachian tube diameter can be routinely performed, and used to plan appropriate surgical techniques and predict outcomes.
Acknowledgement
This study was financially supported by research funding from Chosun University, Gwangju, South Korea (2022).
Competing interests
None declared





