Introduction
Mild cognitive impairment (MCI) refers to a transitional state between the cognition of normal aging and mild dementia (APA, 1994), in which patients have complaints of impairment in memory or other cognitive functions without a relevant impact on the day-living activities. However, it has been reported that MCI patients may also show neuropsychiatric symptoms (Geda et al., Reference Geda2014; Lyketsos et al., Reference Lyketsos, Lopez, Jones, Fitzpatrick, Breitner and DeKosky2002). These symptoms refer to non-cognitive, behavioral, or psychiatric dysfunctions and include disturbances of mood, perception, thinking, or behavior related to a neurocognitive disorder (Mallo et al., Reference Mallo2018). Occurrence of neuropsychiatric symptoms in MCI has been associated with greater functional impairment, accelerated progression of dementia, and poorer quality of life. The presence of psychotic signs (i.e. delusion and hallucinations; Fuller et al., Reference Fuller, Choudhury, Lowe and Balsis2020), anxiety (Mah et al., Reference Mah, Binns and Steffens2015), or apathy (Delrieu et al., Reference Delrieu2015) may increase the risk for cognitive and functional impairments, dementia, and institutionalization (Maresova et al., Reference Maresova, Hruska, Klimova, Barakovic and Krejcar2020). Among these symptoms, depression is the symptom most frequently observed in patients with MCI followed by apathy, irritability (Lyketsos et al., Reference Lyketsos, Lopez, Jones, Fitzpatrick, Breitner and DeKosky2002) aggression, agitation, and anxiety (Palmer et al., Reference Palmer2010). Conversely, disinhibition, euphoria, eating disorders, and aberrant motor behavior seem to be less commonly observed in MCI patients (Martin and Velayudhan, Reference Martin and Velayudhan2020). Some authors (Geda et al., Reference Geda, Roberts and Knopman2008) observed that MCI showed higher frequency of apathy, agitation, irritability, and depression, compared to normal adults, and that psychotic symptoms were rather rare.
However, most of the studies focused on which specific neuropsychiatric symptom may predict the conversion from MCI to dementia (Tampi and Jeste, Reference Tampi and Jeste2022). Only a few studies explored the association between neuropsychiatric symptoms, cognitive functioning, and imaging biomarkers in individual with MCI. It has been reported that MCI individuals with apathy showed poorer performance on decision-making tasks than MCI patients without apathy (Bayard et al., Reference Bayard, Jacus, Raffard and Gely-Nargeot2014). Other authors (Brodaty et al., Reference Brodaty2012) observed significant associations of depression and anxiety with executive functions, agitation and anxiety with memory functions, and agitation, anxiety and apathy with visuo-spatial functions. However, these authors explored the neuropsychiatric symptoms by conducting the interviews over the phone within a median of 34 days. In other studies (Beaudreau and O’Hara, Reference Beaudreau and O’Hara2008), it has been observed that anxiety MCI is associated with impairments in global cognitive functioning and anterograde memory.
Brain structural correlates of neuropsychiatric symptoms in patients with MCI are largely unknown, with most imaging studies focusing on the association of a specific symptom with regional brain changes. Previous literature reviews (Boublay et al., Reference Boublay, Schott and Krolak-Salmon2016) have shown variable associations between behavioral symptoms and atrophic and vascular changes in brain, especially involving areas in the default mode network (such as the hippocampus, posterior cingulate cortex/precuneus complex, lateral parietal cortex) and the salience network (such as the anterior cingulate cortex, orbitofrontal cortex, amygdala, and striatum). Others have correlated CSF amyloid and tau levels to neuropsychiatric burden in AD patients (Ramusino et al., Reference Ramusino2021). When looking at individual symptoms, agitation/aggression has been shown as the most consistent neuropsychiatric symptom related to core AD CSF biomarkers (Showraki et al., Reference Showraki2019). A systematic review of imaging studies suggested that apathy and psychosis have been associated with either volume reductions or decreased metabolism in the prefrontal cortex, anterior cingulate, and medial temporal lobes (Alves et al., Reference Alves2017). In MCI subjects, the presence of affective neuropsychiatric symptoms does not seem to be related to CSF biomarkers profile (Jang et al., Reference Jang2020), while mild behavioral impairment in older adults without dementia is associated with brain amyloid pathology (Sun et al., Reference Sun2021), but not with tau or neurodegeneration (Lussier et al., Reference Lussier2020). Interestingly, locus coeruleus integrity in AD has been recently shown as a significant predictor of neuropsychiatric symptom severity (Cassidy et al., Reference Cassidy2022).
To the best of our knowledge, no studies explored the possible association of specific neuropsychiatric symptoms with specific cognitive dysfunctions and their neuroanatomical correlates, in patients with MCI. Therefore, in the present study, we sought to characterize the association of global neuropsychiatric symptoms burden with gray matter volume and tau deposition in predefined brain regions and to evaluate which neuropsychiatric symptoms more purely relate to cognitive dysfunction, relative to other neuropsychiatric symptoms.
Methods
Participants
All data used in the present study were obtained from the third study phases of the Alzheimer’s Disease Neuroimaging Initiative (ADNI-3) database (see adni.loni.usc.edu for more information) from September 2021 to December 2021. ADNI is an ongoing international longitudinal study aimed at the identification of markers for the early detection and monitoring of AD such as CSF tau and amyloid, MRI, FDG, amyloid and tau PET scans, proteomics, as well as demographics and psychometric data of older adults with normal cognition, healthy adults (HA), and MCI. ADNI-3 phase, in particular, includes tau PET scans with Flortaucipir (AV-1451).
According to the ADNI guidelines (ADNI-3 Protocol, 2016), MCI is defined by a Mini-Mental State Examination (MMSE; Folstein et al., Reference Folstein, Folstein and McHugh1975) raw score of 24-30, an abnormal memory function as documented by scoring below education-adjusted cutoff value on the Logical Memory II subscale from the Wechsler Memory Scale – revised (Wechsler, Reference Wechsler1987), and by a clinical dementia rating scale (CDR; Morris, Reference Morris1993) score of 0.5, with preserved daily functioning at home confirmed by a study partner. For this study, data from a total of 233 (103 female) MCI participants were available. We also included data from 305 (174 female) HA participants who did not show occurrence of neuropsychiatric symptoms as assessed by means of the Neuropsychiatric Inventory (see below).
Assessment of cognitive abilities
Beyond the MMSE as inclusion criteria of the ADNI-3 study phase, all the participants underwent neuropsychological tests assessing several cognitive domains. In particular, memory abilities were assessed by means of the word recall, word delayed recall, and word recognition tests of the Alzheimer’s disease Assessment Scale – Cognition (ADAS-Cog; Rosen et al., Reference Rosen, Mohs and Davis1984) and the immediate recall, delayed recall, and recognition of the Rey auditory verbal learning test (Rey, Reference Rey1964). The language abilities were assessed by means of the ADAS-Cog naming test (Rosen et al., Reference Rosen, Mohs and Davis1984), the Multilingual naming test (Gollan et al., Reference Gollan, Weissberger, Runnqvist, Montoya and Cera2012), and the Category fluency animals test (Morris, Reference Morris1993). The visuo-spatial abilities were assessed by means of the ADAS-Cog copying geometric designs (Rosen et al., Reference Rosen, Mohs and Davis1984) and the Clock drawing test (Cahn et al., Reference Cahn1996). Finally, the frontal/executive abilities were assessed by the ADAS-Cog number cancelation (Rosen et al., Reference Rosen, Mohs and Davis1984) and the Trail making test (part A, part B, and difference between part A and part B; Reitan, Reference Reitan1958).
Assessment of neuropsychiatric symptoms
Presence and severity of neuropsychiatric symptoms were assessed by means of the Neuropsychiatric Inventory (NPI; Cummings, Reference Cummings1997). The NPI is an informant-report structured interview assessing the following psychopathological domains: delusions, hallucinations, agitation/aggression, depression, anxiety, euphoria, apathy, disinhibition, irritability, aberrant motor behavior, sleep, eating. For each psychopathological domain, if the screening question is answered negatively the interviewer moves to the next domain, whereas if it is answered affirmatively then the specific clinical signs are rated on a four-point frequency scale and a separate three-point severity scale. For each psychopathological domain, a total score is provided by multiplying frequency and severity scales (range: 0–12). The total NPI score is provided by the sum of the individual domain score (score range: 0–144).
Imaging data extraction
Analysis protocol from the UC Berkeley and Lawrence Berkeley National Laboratory is available on the ADNI website (Landau S, Flortaucipir (AV-1451) processing methods). For each subject, data are expressed as regional SUVR and the Flortaucipir scans were paired with a structural MRI scans. The available MRI that is closest in time to each PET is segmented with Freesurfer (version 7.1.1) to define regions of interest in native space. Each Flortaucipir scan is coregistered to its corresponding bias-corrected T1 created by Freesurfer, and the mean Flortaucipir uptake is computed within each region. In order to reduce the influence of off-target Flortaucipir binding, available data with partial volume correction (PVC) using the geometric transfer matrix (GTM) have been used for this analysis.
The normalized Flortaucipir SUVRs used in this study were generated by dividing the SUVR in the region of interest by the inferior cerebellar GM SUVR, which was used as a reference region. Selection of the regions of interest was based on previous studies (Alves et al., Reference Alves2017; Boublay et al., Reference Boublay, Schott and Krolak-Salmon2016; Femminella et al., Reference Femminella, Harold, Scott, Williams and Edison2021; Siafarikas et al., Reference Siafarikas2021; Victoroff et al., Reference Victoroff, Lin, Coburn, Shillcutt, Voon and Ducharme2018); thus, the areas included in the analysis were middle frontal region, orbitofrontal region, amygdala, hippocampus, anterior cingulate cortex, posterior cingulate cortex, striatum, and the composite regions Braak 3–4 and Braak 5–6. Freesurfer-generated regional volumes were also compared in predefined areas in the study.
Statistical Analyses
As a first step, we computed number and type of neuropsychiatric symptoms in MCI participants. For descriptive purposes, we divided MCI participants into two groups: MCI patients without neuropsychiatric symptoms (MCI- group) and MCI patients with neuropsychiatric symptoms (MCI+ group), including in this last group all the patients who presented occurrence of at least one type of neuropsychiatric symptom. Analysis of variance (ANOVA) was used to compare the diagnostic groups in terms of demographic, cognitive, and imaging data. Then, to detect differences on demographic (age, education) and clinical (CRD) data, and cognitive test scores between the participants, we ran a multivariate analysis of variance (MANOVA) entering the group (MCI+, MCI-, and HA) as an independent variable, whereas the demographic, clinical, and cognitive data were entered as dependent variables. Post hoc analyses were performed by means of Bonferroni-corrected post hoc comparisons, setting the level of significance at p < 0.05.
To test whether any possible association existed between neuropsychiatric symptoms and cognitive performance, we computed Spearman’s correlation coefficients among the total number of neuropsychiatric symptoms (as assessed by the Neuropsychiatric Inventory), and the raw scores on cognitive tests, in MCI+ participants. Then, we performed a sub-analysis by further computing Spearman’s correlation coefficients between individual neuropsychiatric domains and raw scores on relevant cognitive tests.
Finally, in order to verify whether MCI+ participants showed more severe degenerative changes compared to MCI- participants, we ran a MANOVA entering normalized Flortaucipir SUVR in the preselected regions (middle frontal region, orbitofrontal region, amygdala, hippocampus, anterior cingulate cortex, posterior cingulate cortex, striatum, and the composite regions Braak 3–4 and Braak 5–6.), accounting for age, gender and education. We also run a separate MANOVA for brain volumes in the same regions as dependent variables, accounting for age, gender, and education in MCI+ vs MCI- participants. Moreover, we run two separate multiple linear regression models with NPI scores as the dependent variable and regional MRI volumes and regional Flortaucipir SUVR as independent predictors, respectively, correcting for age, gender, education, and MMSE.
Results
In MCI individuals, the neuropsychiatric symptoms occurred in 143/233 (61.4%) participants (MCI+ group), whereas 90/233 (38.6%) MCI did not show neuropsychiatric disorders (MCI- group). Among MCI+, 2/233 (0.8%) patients showed delusions, 1/233 (0.4%) hallucinations, 32/233 (13.7%) agitation/aggression, 61/233 (26.1%) depression, 30/233 (12.8%) anxiety, 4/233 (1.7%) euphoria, 37/233 (15.8%) apathy, 28/233 (12%) disinhibition, 55/233 (23.6%) irritability, 8/233 (3.4%) aberrant motor behavior, 55/233 (23.6%) sleep disturbances, and 21/233 (9%) eating disorders.
Regional normalized PVC Flortaucipir uptake in healthy comparisons, MCI- and MCI+ subjects are shown in Figure 1.

Figure 1. Individual SUVR values for 18F-AV-1451 binding in MCI- and MCI + compared to the comparisons (HA) (* indicates a significant difference set at p < 0.05 on ANOVA with Bonferroni post hoc correction).
MANOVA on demographic and clinical data, and cognitive tests scores (see Table 1) comparing the three participants groups (MCI+, MCI-, and HA) revealed a significant effect of the group diagnosis (Wilks’ lambda = .16; p < 0.001; η2 p = 0.59). In particular, MCI+ individuals showed significantly poorer performance on MMSE, MOCA, memory and language tests, Clock drawing test, and Trail making test (part A, part B, B-A), compared with HA. Moreover, MCI+ individuals showed significantly poorer performance on MMSE, ADAS-cog memory subtests, ADAS-cog naming, and Trail making test (part B, and B-A), compared with MCI- individuals.
Table 1. Mean, standard deviation (SD), and effect size measure (Cohens’ d) on demographic and clinical data, and cognitive tests scores in individuals with mild cognitive impairment showing (MCI+), or not showing (MCI-) neuropsychiatric symptoms, and healthy adults (HA)

Note: MMSE (Mini-Mental State Examination); MOCA (Montreal Cognitive Assessment); CDR (Clinical Dementia Rating scale); *significantly different from HA at p < 0.001; °significant different from MCI- at p < 0.001; the Neuropsychiatric Inventory – total score was not entered in the statistical analysis; the effect sizes were measured by determining the Cohens’ d.
Spearman’s correlation analysis (see Table 2) revealed that the total number of neuropsychiatric symptoms was significantly associated with performance on RAVLT – delayed recall and TMT (part A, part B, and B-A score). In particular, we observed that agitation/aggression symptom was associated with scores on Trail making test – part B (p = 0.01) and irritability symptom to score on Trail making test – part B (p = 0.01).
Table 2. Spearman’s correlation coefficients between scores on cognitive test and total number of neuropsychiatric symptoms in MCI patients showing neuropsychiatric symptoms

Note: In bold are the significant values.
In order to verify whether MCI subjects with neuropsychiatric symptoms would show more severe degenerative changes compared to those with no behavioral symptoms, we compared in these two groups both in vivo tau deposition and brain volume of our predefined regions. MANOVA on normalized PVC Flortaucipir uptake did not show any significant differences between the two groups in all the predefined regions (see Table 3). In terms of regional volumes, there was a significant effect of the group diagnosis, as subjects with behavioral symptoms had lower orbitofrontal cortex and bilateral posterior cingulate cortex volumes (Wilks’ lambda = 0.88; p = 0.001; η2 p = 0.11), compared to MCI subjects without behavioral symptoms (see Table 4). Spearman’s correlation analysis between the most frequent behavioral symptoms in this cohort (depression, irritability, sleep disturbances, apathy, and agitation) and orbitofrontal cortex and bilateral posterior cingulate cortex volumes did not show significant associations (data not shown).
Table 3. Normalized Flortaucipir SUVR with partial volume correction in MCI patients with and without behavioral symptoms

Table 4. Regional brain volumes (mm3) in MCI patients with and without behavioral symptoms

* Significantly different from MCI + at p < 0.05.
In order to evaluate the potential independent contribution of imaging markers on NPS in MCI subjects, we run multiple linear regression models with total NPI scores as dependent variable, correcting for age, gender, education, and MMSE. Table 5 (reported in Supplemental material) shows that, among regional volumetric measures, only bilateral posterior cingulate cortex showed an independent predictive value on total NPI scores. The model built with regional Flortaucipir uptake in the predefined regions as independent predictor was not significantly associated with NPI scores (data not shown).
Discussion
Neuropsychiatric symptoms may often occur in individuals with MCI, thus causing significant distress and functional impairments. In the present study, we were able to demonstrate that the global burden of neuropsychiatric symptoms in MCI is associated with regional brain atrophy and with impairment in frontal/executive functions, but not with regional tau deposition. In this population, we observed a high prevalence of neuropsychiatric symptoms (61.4%), thus confirming that this pattern is common in individuals with MCI (Alves et al., Reference Alves2017). Among these symptoms, depression, irritability, and sleep disturbances were the most common. However, our findings suggested that neuropsychiatric impairments were associated with dysfunctions of select cognitive abilities and with reduction of gray matter volume in orbitofrontal cortex and posterior cingulate cortex, while no differences were observed in terms of regional tau deposition.
Indeed, our results showed that neuropsychiatric symptoms were mainly related to general cognitive functioning and frontal/executive dysfunctions in individuals with MCI. Thus, we observed that MCI individuals showing neuropsychiatric symptoms achieved poorer performance on tasks assessing planning and organization of behavior, selective and divided attention, and inhibitory control abilities. Indeed, clinical signs such as depression, irritability, or sleep disturbances would result from inadequate and unpreserved frontal/executive abilities (De Lucia et al., Reference De Lucia, Grossi, Mauro and Trojano2015; De Rosa et al., Reference De Rosa2018; Grossi et al., Reference Grossi, De Lucia and Trojano2015).
A possible link between neuropsychiatric symptoms and biomarkers profiles in the AD trajectory has been often suggested, but conclusive data are still missing. Previous studies have shown an association between high CSF total tau levels and anxiety in MCI subjects (Ramakers et al., Reference Ramakers, Verhey and Scheltens2013), higher total, and phospho-tau levels in AD subjects with agitation and apathy (Bloniecki et al., Reference Bloniecki, Aarsland, Cummings, Blennow and Freund-Levi2014), and an association between sleep disturbances and CSF biomarkers profile (Kim et al., Reference Kim2022). Other reports, however, have shown that affective neuropsychiatric symptoms (depression, anxiety, apathy, irritability) in MCI subjects from the ADNI dataset were not associated with CSF AD biomarkers (Jang et al., Reference Jang2020). Thanks to the availability of Flortaucipir PET scans in the ADNI population, we sought to evaluate whether regional tau deposition was associated with neuropsychiatric symptoms in MCI subjects, but we did not find a significant effect in this cohort. Our results are in line with those by Sun and colleagues (Sun et al., Reference Sun2021) who specifically explored the association between mild behavioral impairment in non-demented ADNI subjects and biomarkers profile, finding that brain amyloid pathology, but not tau, might be associated with early behavioral disturbances in subjects at risk for AD. Recently presented conference data have shown an association between apathy scores and regional tau deposition in MCI and AD subjects from the ADNI cohort but a methodological comparison with our work cannot be made at the present time (Premnath et al., Reference Premnath, Gonzalez, Properzi, Rosenberg, Marshall and Gatchel2021).
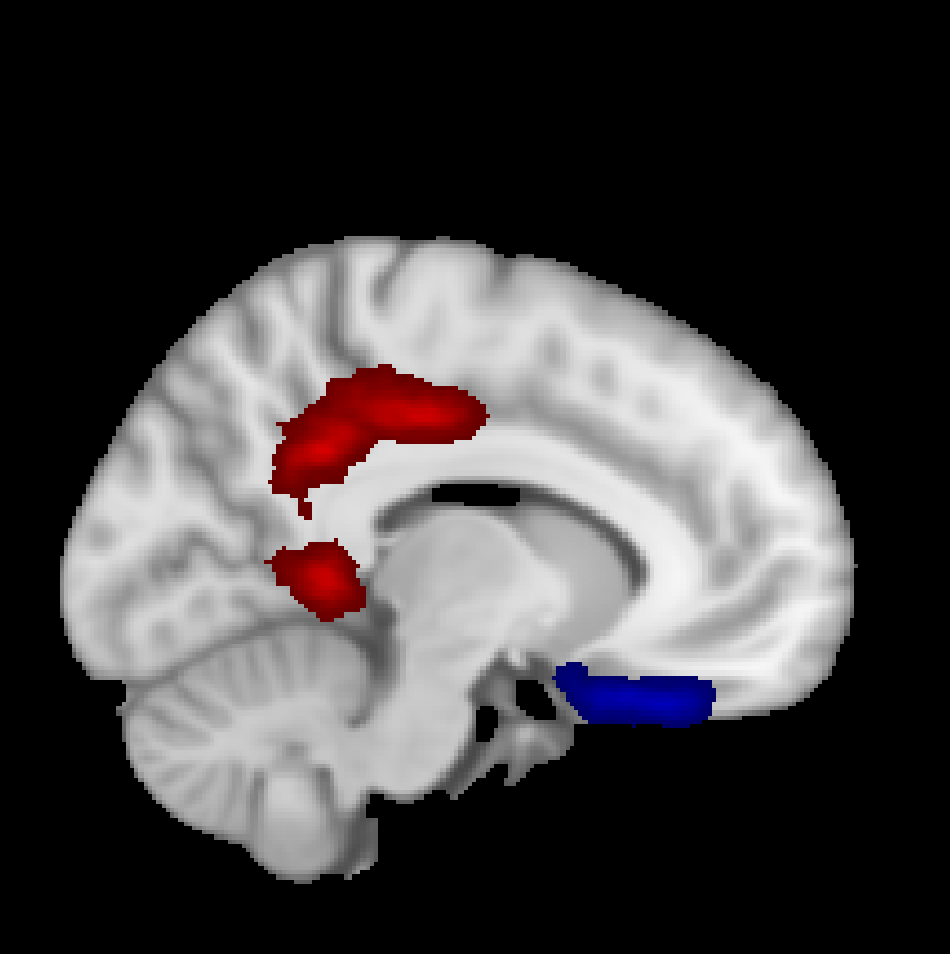
Neuroimaging correlates of neurodegeneration have been associated with neuropsychiatric symptoms in the AD continuum. In particular, high medial temporal atrophy scores were significantly associated with apathy and disinhibition (García-Alberca et al., Reference García-Alberca, Florido, Cáceres, Sànchez-Toro, Lara and Garcìa-Casares2008). Others have reported reduced brain metabolism in the prefrontal cortex and anterior cingulate cortex in AD patients with psychosis and apathy (Alves et al., Reference Alves2017). In this study, we were able to demonstrate that MCI subjects with behavioral symptoms had lower orbitofrontal cortex and bilateral posterior cingulate cortex volumes (for a graphical representation, see Figure 2 reported in Supplemental material). Orbitofrontal cortex has been associated with emotions since it receives inputs from sensory and limbic amygdala and medial temporal regions and integrates this information. Atrophy of this area might have an impact on processing of emotional behavior, leading to difficulties with inhibitory and aggressive behavior (Alves et al., Reference Alves2017). Posterior cingulate cortex volume was the only significant predictor of global neuropsychiatric burden in this MCI population. The posterior cingulate cortex is a central node in the default mode network of the brain and is early affected by neurodegeneration in AD. Previous reports have shown that high NPI scores predicted 2-year hypometabolism in the posterior cingulate cortex in preclinical AD patients (Ng et al., Reference Ng2017). More recently, decreased posterior cingulate gyri perfusion, in prodromal AD was associated with behavioral and psychological symptoms of dementia (Yasuno et al., Reference Yasuno, Matsuoka, Miyasaka, Takahashi, Kitamura, Yoshikawa, Hattori, Kichikawa and Kishimoto2019).
Some limitations of the present study have to be considered. We did not perform a qualitative analysis of the different types of neuropsychiatric symptoms, but further studies could consider investigating the correlation of regional gray matter volumes with frequency and severity of different clinical signs in MCI. Second, our sample size was relatively small, and since the lower the subjects-to-variables ratio the lower the generalizability, our results await to be confirmed on larger samples of participants.
Notwithstanding these limitations, this study provided evidence that neuropsychiatric symptoms occur even in the lack of clinically relevant cognitive deterioration, and that are mainly related to defects of control executive abilities, and to the reduction of gray matter volume in the orbitofrontal and posterior cingulate cortices. A better understanding of the cognitive and neuroanatomical mechanisms of neuropsychiatric symptoms in MCI could help develop more targeted and efficacious treatment alternatives.
In conclusion, we found that MCI individuals show neuropsychiatric disorders, especially depression, irritability, and sleep disturbance. These dysfunctions were associated with impairments of frontal/executive functions, especially planning and organization of behavior, selective and divided attention, and inhibitory control abilities. Moreover, the neuropsychiatric symptoms in our MCI individuals were related to reduction of gray matter volume in the orbitofrontal and posterior cingulate cortices. Take together, these findings contribute to a better comprehension of the cognitive and neuroanatomical mechanisms underlying the neuropsychiatric symptoms in MCI individuals.
Conflict of interest
None.
Description of author’s role
All the authors contributed to study conception and approved the final version of the manuscript. In particular, N. De Lucia and G.D. Femminella contributed to literature research, data analysis and interpretation, and manuscript writing. N.M. Maldonato and N. Ferrara contributed to edit the manuscript. G. Carbone, G, Rengo, and B. Muzii assisted with acquisition of data.
Acknowledgements
We are grateful to all the patients and subjects for their consent to participate in the ADNI study.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S104161022200117X