
 Quick Check
Quick Check
A Acute Mania 35
B Rapid Cycling 38
C Acute Bipolar Depression and Bipolar II Disorder (BD-2) 44
D Bipolar Disorder Maintenance and Response Prediction 48
E Unipolar MDD 55
F Suicidality 57
G Neuroprotection 65
H Aggressive or Impulsive Behavior in Child/Adolescent Patients with Conduct Disorder, Borderline Personality Disorder (BPD) and Intellectual Disability 74
I Neutrophilia 76
J Lithium’s Mechanisms of Action 77
Principles
Lithium is considered the gold standard for bipolar I disorder (BD-1) prophylaxis. Lithium monotherapy is effective in mania within the first seven days of treatment, and is no less effective than other mood stabilizer monotherapies for rapid cycling BD (RC-BD).
Lithium remains an effective adjunctive option with antidepressants for unipolar major depressive disorder (MDD), but is not comparably effective as monotherapy for acute BD depression.
Retrospective data indicate lithium reduces attempted and completed suicides, and reduces dementia incidence 50% among BD patients.
Lithium has limited data for management of aggressive or impulsive behavior in child/adolescent patients with conduct disorder, in patients with borderline personality disorder or with intellectual disability, but can be considered in select circumstances.
Lithium directly increases neutrophil counts by inducing production of granulocyte colony stimulating factor. This can be of clinical value in the management of clozapine treated patients.
There are numerous intracellular pathways modulated by lithium therapy which explain its mood stabilizing and neuroprotective effects.
Introduction
What to Know: Introduction
Lithium is considered the preferred maintenance mood stabilizer for any bipolar spectrum patient with a history of mania (e.g. bipolar I disorder; schizoaffective disorder, bipolar type [SAD-BT]). The role of lithium for bipolar II disorder depends on the need for mood stabilization.
In real world studies, use of lithium, but not valproic acid, is associated with lower psychiatric hospitalization rates in bipolar disorder patients. Oxcarbazepine, topiramate and gabapentin have no effect on hospitalization risk.
Retrospective studies provide compelling evidence for lithium’s unique impact on risk for completed suicide, and for reduction in dementia risk with long-term use in older bipolar patients.
Lithium is an effective adjunctive option for unipolar major depression.
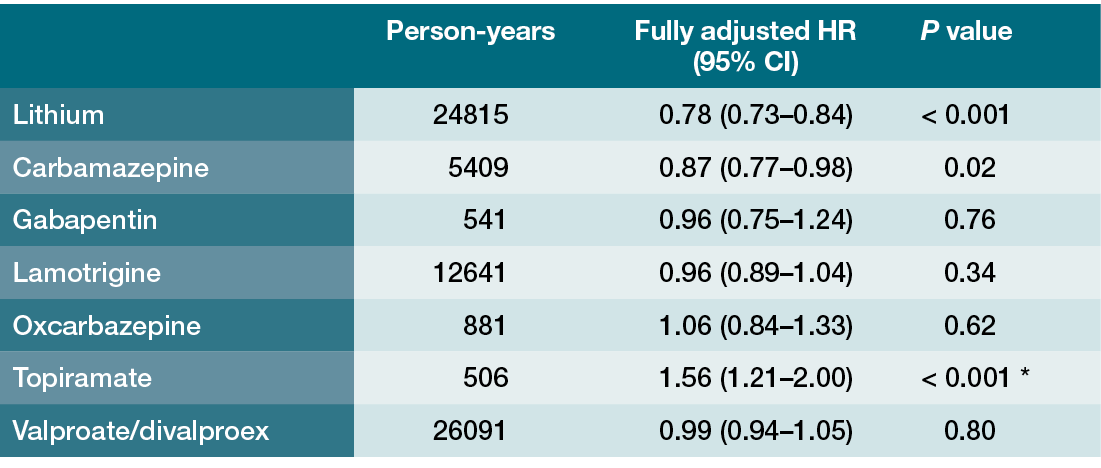
As of this writing, every international bipolar disorder (BD) treatment guideline or major published review recommends lithium as the gold standard for acute and maintenance therapy in BD spectrum patients, especially those with a history of mania [Reference Malhi, Gessler and Outhred1–Reference Fountoulakis, Tohen and Zarate4]. Lithium’s acute antimanic properties and prophylactic effectiveness have been known for over 70 years, but the approval of second generation antipsychotics (SGAs) for BD-1 mania, BD depression and BD-1 maintenance (as monotherapy or adjunctive to mood stabilizers), and the increased use of anticonvulsant mood stabilizers such as divalproex (valproic acid or VPA), resulted in dramatic declines in lithium use over the past 20 years (Figure 1.1) [Reference Poranen, Koistinaho and Tanskanen5]. These trends have stabilized, albeit at low levels, with a Finnish study noting that only 4.1% of newly diagnosed BD spectrum patients from 2016 to 2018 received lithium [Reference Poranen, Koistinaho and Tanskanen5]. One epiphenomenon of low utilization is the loss of a shared cultural memory among mental health professionals regarding lithium’s efficacy, leading to erroneous conclusions that non-lithium therapies are equivalent, despite evidence to the contrary. Supporting the notion of lithium’s overall superiority are papers that report real world outcomes among BD patients treated in an era when clinicians have access to an array of medication options including SGAs. One of the largest analyses examined rates of rehospitalization among 18,018 Finnish patients previously hospitalized for BD from 1996 to 2012 [Reference Lahteenvuo, Tanskanen and Taipale6]. Although the data were not analyzed by BD subtype, the underlying assumption was that this population was predominantly BD-1, as other forms of BD have lower psychiatric hospitalization rates. The study used a within-individual analytic method in which each individual was used as his or her own control to examine hospitalization risk during periods on or off various treatments. Over a mean follow-up period of 7.2 years, 54.0% of the initial sample experienced a least one psychiatric rehospitalization. As noted in Table 1.1, lithium was the most effective mood stabilizer in preventing psychiatric rehospitalization, and carbamazepine also displayed efficacy, but this was not true for VPA or for any other anticonvulsant [Reference Lahteenvuo, Tanskanen and Taipale6]. When outcomes were broken down by drug class, mood stabilizers were effective at reducing psychiatric rehospitalization risk while antipsychotics were not, and use of sedatives, benzodiazepines or antidepressants increased rehospitalization risk.

Figure 1.1 20-year trends in use of mood stabilizing (MS) medications among newly diagnosed Finnish BD patients [5]
Table 1.1 A within-individual analysis of the association between use vs. no use of medications and the risk of psychiatric rehospitalization among Finnish BD patients previously hospitalized for bipolar disorder from 1996 to 2012 (n = 18,018) [Reference Lahteenvuo, Tanskanen and Taipale6]
| Person-years | Fully adjusted HR (95% CI) | P value | |
|---|---|---|---|
| Lithium | 24815 | 0.78 (0.73–0.84) | < 0.001 |
| Carbamazepine | 5409 | 0.87 (0.77–0.98) | 0.02 |
| Gabapentin | 541 | 0.96 (0.75–1.24) | 0.76 |
| Lamotrigine | 12641 | 0.96 (0.89–1.04) | 0.34 |
| Oxcarbazepine | 881 | 1.06 (0.84–1.33) | 0.62 |
| Topiramate | 506 | 1.56 (1.21–2.00) | < 0.001 Footnote * |
| Valproate/divalproex | 26091 | 0.99 (0.94–1.05) | 0.80 |
* increased rehospitalization risk
In-Depth 1.1 Antipsychotics Have Antimanic Properties but Are Not Equivalent to Lithium Mechanistically or Clinically
Few would dispute lithium’s efficacy for acute mania, and a 2022 comprehensive meta-analysis on lithium treatment of adult BD noted that all of the placebo-controlled randomized clinical trials (RCTs) performed using modern study methodologies were positive, with onset of therapeutic effect by day 7 [Reference Fountoulakis, Tohen and Zarate4]. Despite the strength of this evidence, some clinicians lack familiarity with lithium loading or other means of rapidly starting lithium, and this can lead to relatively slow titrations and prolonged periods of subtherapeutic levels [Reference Kook, Stimmel and Wilkins7]. Any perceived lack of early efficacy in acute mania may partly be the product of the lithium initiation method [Reference Keck, McElroy and Bennett8, Reference Cipriani, Barbui and Salanti9], but it is important to state that antipsychotics are extremely effective antimanic agents with faster onset than mood stabilizer monotherapy [Reference Cipriani, Barbui and Salanti9, Reference Sun, Woods and Findling10]. Many first generation antipsychotics (FGAs) and SGAs have acute mania indications, some of which have injectable formulations that can be used for floridly manic patients who refuse oral mood stabilizers. Antipsychotics are indisputably an important part of acute mania management, and aripiprazole, olanzapine and injectable risperidone microspheres have indications as maintenance monotherapy in BD-1 adults; however, antipsychotics do not share lithium’s impact on 2nd messenger systems, and failing to add lithium has clinical implications [Reference Du, Quiroz and Yuan11, Reference Meyer, Brunton and Knollmann12]. As will be discussed in the section on lithium’s mechanisms of action, stimulation of dopamine D2 receptors by agonists (e.g. amphetamines) induces hyperlocomotion, a useful animal model for the psychomotor agitation of mania [Reference Del’ Guidice and Beaulieu13]. Dopamine D2 receptor stimulation affects intracellular G-protein dependent pathways resulting in decreased cyclic AMP (cAMP) levels, but D2 agonists also alter signaling in a non-G-protein pathway involving beta arrestin 2 (βArr2), increasing activity of glycogen synthase kinase 3-β (GSK3-β) and inducing hyperlocomotion [Reference O’Brien, Huang and Buccafusca14]. Lithium robustly inhibits GSK3-β activity and markedly decreases D2 agonist stimulated hyperlocomotion; moreover, lithium is an even more selective and potent inhibitor of GSK3-β activity than SGA antipsychotics [Reference Urs, Snyder and Jacobsen15]. Therefore, while certain features of mania will improve after antipsychotic administration, other untreated aspects can continue to drive positive psychotic symptoms, ongoing acts of impulsivity or mood instability [Reference Meyer, Cummings and Stahl16]. This phenomenon was described by the Danish psychiatrist and lithium pioneer Mogens Schou in the sixth edition of his guide to lithium treatment: “An experienced patient, who during previous manias had first tried a neuroleptic and then lithium, reported that during treatment with the former he felt as if the gas pedal and the brake were pressed down at the same time. With lithium it was as if the ignition had been switched off” [Reference Schou17]. The differential effects of SGAs and lithium on mood stability are seen very clearly in long-term naturalistic outcomes of BD-1 patients after a manic episode. Follow-up data subsequent to 5713 hospitalizations for mania among Swedish BD-1 patients aged 18–75 (2006–2014) showed that those on SGA monotherapy experienced markedly higher rates of treatment failure than those on lithium, with medication switching and discontinuation the leading reasons for failure to persist with SGA monotherapy [Reference Wingård, Brandt and Bodén18].
Despite the abundant RCT and retrospective data supporting lithium’s effectiveness in BD-1, there is a surprising paucity of studies for other bipolar spectrum disorders such as BD-2, schizoaffective disorder, bipolar type (SAD-BT) and RC-BD patients [Reference Tondo, Baldessarini and Floris19–Reference Parker, Ricciardi and Tavella22]. As SAD-BT and BD-1 share the same liability for mania, it is often assumed that lithium’s efficacy in BD-1 (acutely and prophylactically) should generalize to this related disorder. There are no data to suggest otherwise, but any statements about lithium’s efficacy in SAD-BT patients rest largely on retrospective studies or older studies with methodological or definitional issues [Reference Öhlund, Ott and Bergqvist21, Reference Keck, McElroy and Strakowski23].
In-Depth 1.2 Lithium in Schizophrenia Spectrum Patients
The limited prospective studies of lithium primarily involve schizophrenia, not SAD-BT, and a 2015 Cochrane review of trials where lithium was added adjunctively to antipsychotic therapy for schizophrenia (22 studies, total n = 763) found that most studies were small and methodologically weak. For nonaffective psychosis (i.e. schizophrenia), any evidence lithium is effective in augmenting antipsychotics was of low quality, and the effects were not significant when more prone-to-bias open RCTs were excluded [Reference Leucht, Helfer and Dold24]. However, a 2022 Finnish real world outcomes analysis of every individual hospitalized for schizophrenia during 1972–2014 (n = 61,889) found that use of adjunctive lithium, VPA or lamotrigine reduced risk of psychosis related rehospitalization by 12% during the follow-up period (1996–2017) [Reference Puranen, Koponen and Lahteenvuo25]. That these effects were seen across several mood stabilizers with varying mechanisms of action suggests that a small subset of patients labeled with a schizophrenia diagnosis most likely have SAD-BT and therefore benefit from mood stabilization in a manner that patients with schizophrenia would not [Reference Meyer, Cummings and Stahl16]. Employing this logic, a 2021 handbook on management of complex treatment resistant psychotic disorders suggests an empiric lithium trial in cases where the working diagnosis is schizophrenia, but SAD-BT is suspected based on history or clinical features [Reference Meyer, Cummings and Stahl16]. Failure to improve with adjunctive lithium confirms the schizophrenia diagnosis, while substantial improvement demands a change in the working diagnosis to SAD-BT.
More research is clearly needed to examine lithium’s efficacy for acute mania and mania prophylaxis in SAD-BT since these patients need mood stabilization for optimal symptom control [Reference Lintunen, Taipale and Tanskanen26]. Conversely, the clinical course of BD-2 dictates less dependence on mood stabilization to prevent hypomania/mania, and the lithium literature in this area is underdeveloped (Figure 1.2) [Reference Chakrabarty, Hadjipavlou, Bond and Parker20, Reference Judd, Akiskal and Schettler27, Reference Judd, Akiskal and Schettler28]. The few prospective lithium trials in BD-2 focus exclusively on depressive symptomatology, with the limited data indicating modest efficacy for lithium as monotherapy [Reference Fountoulakis, Tohen and Zarate4]. There are also studies showing that BD-2 patients respond to and tolerate traditional antidepressant therapies (e.g. venlafaxine) without risk of hypomania induction [Reference Amsterdam, Lorenzo-Luaces and Soeller29]; nevertheless, lithium remains an important option for those BD-2 patients who do need mood stabilization and for whom non-lithium maintenance options such as lamotrigine have been insufficiently effective.

Figure 1.2 Proportion of time spent asymptomatic or with mood symptoms based on long-term weekly follow-up of BD-1 (n = 146, mean follow-up 12.8 years) and BD-2 (n = 86, mean follow-up 13.4 years) patients [27, 28]
The exact place of lithium in the BD-2 algorithm is not easily answered with existing data, yet one area of the BD spectrum that has been addressed more successfully is the value of lithium for RC-BD patients [Reference Hui, Kandola and Shen30, Reference Strawbridge, Kurana and Kerr-Gaffney31]. Extensive research into the clinical course of RC-BD has revealed that these patients respond poorly to any form of mood stabilizer monotherapy due to frequent depressive episodes of short duration [Reference Strawbridge, Kurana and Kerr-Gaffney31]. Lithium is effective in preventing hypomania or mania in BD-1 or BD-2 patients with a history of rapid cycling, and lithium treated RC-BD patients do not spend a greater proportion of time ill than lithium treated BD patients without a history of rapid cycling [Reference Baldessarini, Tondo and Floris32]. The findings from multiple sources point to the fact that RC-BD patients will often need combination therapy, especially for management of recurrent major depressive episodes [Reference Strawbridge, Kurana and Kerr-Gaffney31]. The few prospective studies in RC-BD show that lithium is not inferior to divalproex [Reference Calabrese, Shelton and Rapport33, Reference Kemp, Gao and Ganocy34], and therefore lithium remains the mood stabilizer of choice for RC-BD-1 patients, with the recognition that an adjunctive medication will almost certainly be needed for bipolar depression (e.g. certain SGAs for acute depressive symptoms, lamotrigine for maintenance) [Reference Strawbridge, Kurana and Kerr-Gaffney31, Reference Zhihan, Fengli and Wangqiang35].
In-Depth 1.3 Despite its Anti-Suicide Properties There are Limited Data for Lithium’s Efficacy in Acute Bipolar Depression
Although there is a vigorous debate about the extent of lithium’s anti-suicide properties [Reference Baldessarini and Tondo36], there is no high-quality evidence that lithium is an effective treatment for acute BD depression [Reference Fountoulakis, Tohen and Zarate4]. There is at least one study demonstrating that lithium monotherapy can reduce depressive recurrences during maintenance therapy of euthymic patients [Reference Weisler, Nolen and Neijber37], but 10 of the 11 lithium monotherapy trials for acute BD depression were methodologically weak by modern standards. The one rigorous, prospective, double-blind, 8-week RCT randomized 802 depressed BD subjects (BD-1, n = 499; BD-2, n = 303) to one of 4 treatment arms: quetiapine 300 mg/d (n = 265), quetiapine 600 mg/d (n = 268), lithium 600–1800 mg/d (n = 136) or placebo (n = 133) [Reference Young, McElroy and Bauer38]. This study did not find efficacy for lithium; there was no correlation between lithium serum levels and depression rating changes; and the lack of efficacy was true in study completers and in the subgroup with higher serum lithium levels (> 0.80 mEq/l) [Reference Fountoulakis, Tohen and Zarate4, Reference Young, McElroy and Bauer38]. Other agents with regulatory approval for acute BD depression are the treatments of choice (e.g. cariprazine, lumateperone, lurasidone, quetiapine, olanzapine/fluoxetine combination), with lamotrigine considered only for maintenance therapy to mitigate depressive relapse. (Lamotrigine’s extended titration to eliminate Stevens–Johnson Syndrome risk prevents acute use for bipolar depression [Reference Calabrese, Bowden and Sachs39].)
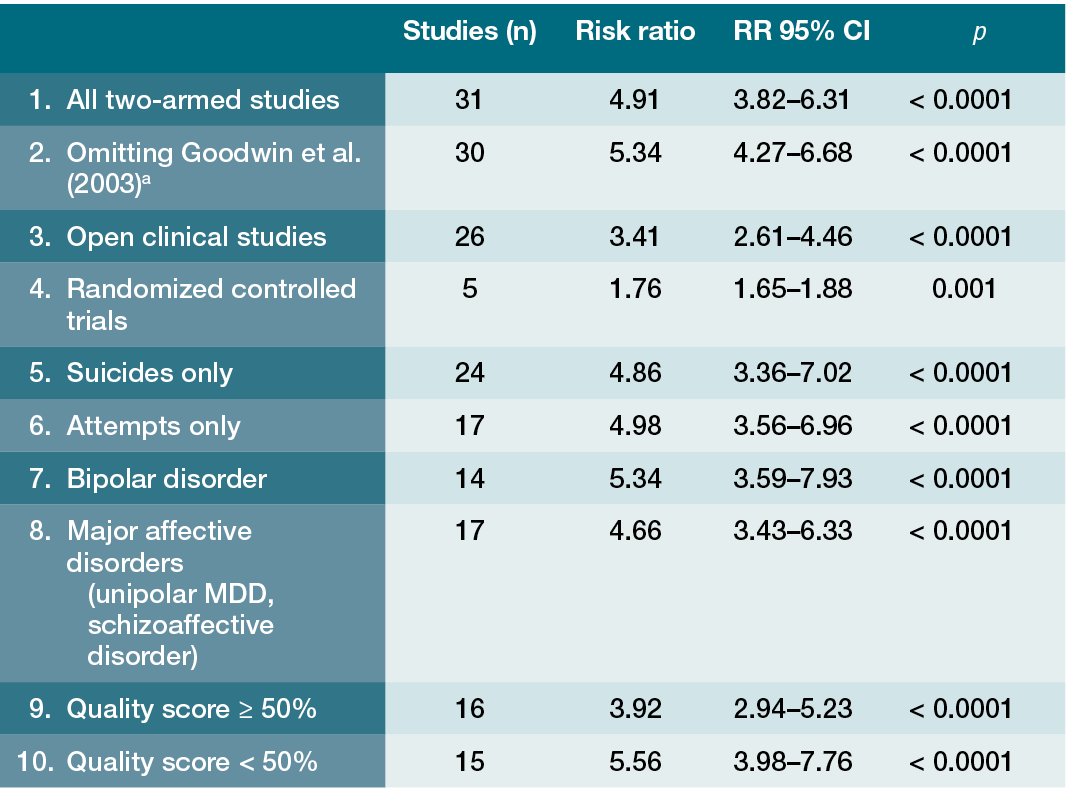
The difficulty in using RCT results to prove that lithium has an impact on risk of completed suicide and possesses neuroprotective properties limits the robustness of conclusions for those applications [Reference Katz, Rogers and Lew40]; however, it is worth noting the lack of compelling data to suggest greater effectiveness for other mood stabilizing agents in these areas, and the accumulation of findings from some (but not all) meta-analyses indicating that lithium has comparatively superior reduction vs. non-lithium therapy for dementia risk among older BD patients, and for reduction in serious suicide attempts and suicide mortality [4, Reference Baldessarini, Tondo and Davis41–Reference Velosa, Delgado and Finger44]. Some of these data come from epidemiological studies in multiple countries that found a correlation between higher lithium levels in the municipal water supply and lower rates of suicide in certain geographic regions, as opposed to ones with comparable sociodemographic and psychiatric characteristics but lithium levels below the median [Reference Barjasteh-Askari, Davoudi and Amini45–Reference Kugimiya, Ishii and Kohno47]. The large number of studies reporting this finding across the Americas, Europe and Asia argue for a plausible association, with a significant caveat about the limitations of such retrospective analyses. Nonetheless, the weight of the evidence is sufficient for clinicians to consider lithium as the preferred agent for BD patients with a history of suicide attempts, despite the limitations of the RCT literature. The same logic also applies when treating older BD-1 patients: the findings of lithium’s effect on dementia risk in BD patients are from retrospective analyses and not prospective RCTs; however, unlike suicidality, there are RCT data demonstrating neuroprotective properties among adults with mild cognitive impairment [Reference Forlenza, Radanovic and Talib48]. With that in mind, having a BD diagnosis is associated with a 3-fold increased risk for dementia, and a 2020 meta-analysis found that long-term lithium use was associated with a 50% reduction in dementia risk [Reference Velosa, Delgado and Finger44].
Lithium has been studied repeatedly for unipolar MDD, primarily as adjunctive therapy, but there is no consensus on lithium’s place in the unipolar MDD treatment algorithm [Reference Undurraga, Sim and Tondo49]. One issue is that certain SGA and glutamate based strategies (e.g. ketamine, esketamine) have double-blind placebo-controlled studies performed with patients on newer antidepressants, thus providing a certain level of confidence for the clinician that these findings will generalize to current practice settings. Unfortunately, much of the early lithium MDD research involved tricyclic antidepressants, and a 2019 meta-analysis found that the last placebo-controlled adjunctive lithium trial for unipolar MDD was published in 2003 [Reference Undurraga, Sim and Tondo49]. Adjunctive lithium was also a treatment arm in a large sequential treatment algorithm study (STAR-D) for participants who failed two prior antidepressant treatments, but the results dampened the enthusiasm for lithium by finding that remission rates were modest for lithium and did not differ from the remission rate with triiodothyronine [Reference Nierenberg, Fava and Trivedi50]. The authors commented that the lower side effect burden and ease of use for triiodothyronine augmentation suggest that it has slight advantages over lithium augmentation in unipolar MDD patients who failed several medication trials [Reference Nierenberg, Fava and Trivedi50]. Nonetheless, despite the availability of SGA and glutamate based options that are effective and require less laboratory monitoring, a recent comparative review commented that adjunctive lithium was somewhat more effective and better tolerated than these other strategies for unipolar MDD, implying that lithium need not be relegated to the latter stages of the MDD treatment algorithm despite the limitations of the data [Reference Vázquez, Bahji and Undurraga51].
The extent of lithium’s anti-aggressive effects is another area where there are virtually no placebo-controlled prospective data, but a large volume of open-label, uncontrolled and retrospective studies, and several papers reporting a positive association between higher levels in drinking water and lower rates of violent crimes [Reference Muller-Oerlinghausen and Lewitzka52, Reference Giotakos53]. While not a panacea, the paucity of options that convincingly decrease risk of completed suicide pose a reasonable argument for consideration of a lithium trial in suicidal BD patients as noted above [Reference Katz, Rogers and Lew40]. A less convincing argument can be made for routine use of lithium to manage conduct disorder and aggression in non-bipolar children or adolescents [Reference Masi, Milone and Manfredi54, Reference Pringsheim, Hirsch and Gardner55], for management of disruptive behaviors in intellectually disabled individuals [Reference Deb, Chaplin and Sohanpal56, Reference Ji and Findling57] or to manage impulsivity in borderline personality disorder [Reference Stone58]. There are more strongly evidence based treatments for some of these clinical scenarios (e.g. SGAs for irritability associated with autistic disorder), and the evidence for lithium (to the extent that any exists) is of low quality.
Lithium has been studied for dozens of other clinical indications, both psychiatric and nonpsychiatric, some of which are no longer relevant, while others remain an important part of psychiatric practice. One example of the former is lithium’s prophylactic use for patients with cluster headache. Early studies indicated lithium was efficacious, with subsequent research linking this to partial agonist activity at serotonin 5HT1B receptors; however, lithium has been replaced by more effective options, including the potent 5HT1B and 5HT1D receptor agonist triptan class for abortive treatment, and by verapamil for prophylaxis [Reference Steiner, Hering and Couturier59, Reference Kwon, Han and Choi60]. The last double-blind, placebo-controlled trial for cluster headache was performed in 1997, but was stopped after the 27th patient was enrolled when a planned interim analysis did not reach the prespecified efficacy signal to differentiate lithium from placebo [Reference Steiner, Hering and Couturier59]. Neutrophilia is a known consequence of lithium therapy, and one that should be communicated to all providers to avoid subjecting patients to an unnecessary work-up for occult infection or a hematological disorder. One current psychiatric application for this property is the use of lithium to support clozapine prescribing [Reference Mattai, Fung and Bakalar61, Reference Nykiel, Henderson and Bhide62]. Lithium directly stimulates neutrophil production by increasing the levels of granulocyte colony stimulating factor [Reference Rothstein, Clarkson and Larsen63–Reference Petrini and Azzara65]. This is a niche but important use for lithium, and one that will likely persist until such time as a medication appears with clozapine’s efficacy and without its neutropenia risk.
In-Depth 1.4 Lithium’s Unique and Diverse Intracellular Mechanisms
That lithium is an agent with numerous and diverse properties is clear, leading to decades of research on lithium’s numerous intracellular mechanisms of action (MOAs), specifically those activities that convey its mood stabilizing, neuroprotective and anti-aggression/anti-suicide properties [Reference Phiel and Klein66–Reference Bellivier and Marie-Claire68]. One can practice psychiatric medicine effectively without understanding the biological hypotheses for lithium’s effectiveness, but an appreciation of certain well-studied pathways, such as that leading to GSK3-β inhibition, can inform practice by providing a molecular basis for lithium’s distinct spectrum of clinical activities. This preclinical research also sheds light on how agents with antimanic properties (e.g. antipsychotics, lithium, divalproex) are not necessarily interchangeable, why manic patients experience the effects of lithium and antipsychotics differently, and why SGA or divalproex monotherapy may not yield the same maintenance outcomes as lithium in BD-1 patients [Reference Wingård, Brandt and Bodén18]. These are very relevant talking points with BD-1 patients who want to pursue SGA maintenance monotherapy due to concerns about lithium, or to avoid its monitoring burden. In an ideal world, there would be clinical predictors and biomarkers of treatment response for lithium and non-lithium therapies to inform treatment choices. While biomarker research is an exciting area of study, it is not yet at the stage of clinical application [Reference Scott, Hidalgo-Mazzei and Strawbridge69]. Translating some of the research on clinical predictors of lithium response into patient-level decisions can also be problematic. Many of the features associated with inadequate lithium response (e.g. substance use, RC-BD, chronic course, anxiety) are also shared with non-lithium therapies, but many of the papers lack comparative data to put those findings into context [Reference Scott, Hidalgo-Mazzei and Strawbridge69–Reference Mishra, Ying and Luis75].
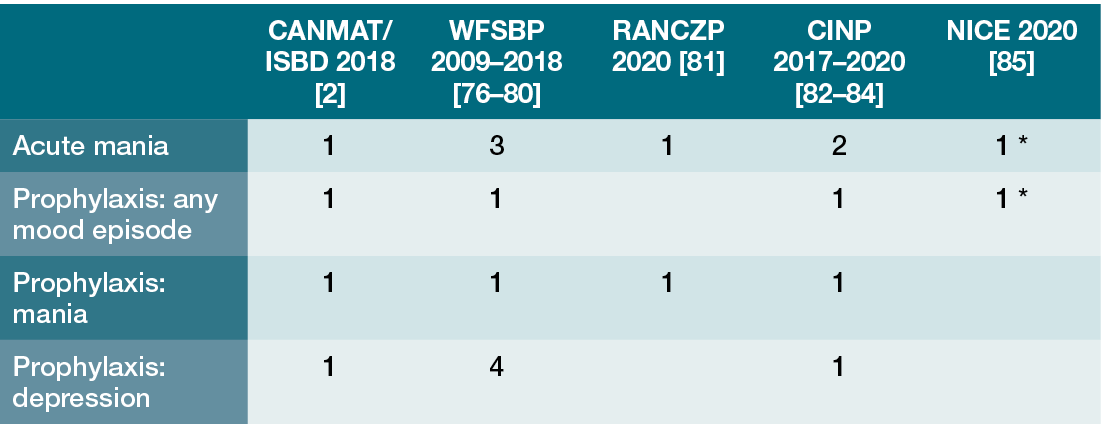
In the end, BD-1 is a difficult disorder to manage, and the finding that only 20% achieve durable remission on lithium monotherapy speaks more to the fact that a single mood stabilizing agent may be insufficient for many BD-1 patients, despite lithium’s unique efficacy spectrum [Reference Lin, Maihofer and Stapp74]. The consensus opinion that lithium is an unparalleled medication and the standard of care for BD-1 rests on the recognition that all treatments have limitations, yet lithium possesses comparative advantages that place it at the top of the treatment algorithm [Reference McIntyre, Berk and Brietzke3]. These relative advantages do not lie in the area of acute mania, BD-2 maintenance, acute bipolar depression or unipolar MDD antidepressant augmentation, but in BD-1 or SAD-BT maintenance, with the impact on suicide related deaths and dementia incidence as important differentiating factors. Those areas in particular where lithium presents a unique therapeutic option (e.g. reduced risk for completed suicide, reduction in dementia risk) are covered in greater length so clinicians can appreciate that conclusions about these properties rest primarily on retrospective analyses, despite attempts to study suicidality in RCTs [Reference Katz, Rogers and Lew40]. There are areas of medicine where certain assertions appear true from the breadth and extent of the retrospective data, but not provably true without performing a large, long-term RCT whose sheer scope might not be economically feasible. Clinical decisions must be made using all of the effectiveness data, even those which are imperfect. After three-quarters of a century, the weight of the data supports the special role of lithium for treatment of mood disorders, especially BD spectrum patients with a history of mania or suicidality, and for older BD-1 individuals (Table 1.2).
Table 1.2 The place of lithium in treatment guidelines updated since 2018 [Reference Fountoulakis, Tohen and Zarate4]
| CANMAT/ISBD 2018 [Reference Yatham, Kennedy and Parikh2] | WFSBP 2009–2018 [Reference Grunze, Vieta and Goodwin76–Reference Grunze, Vieta and Goodwin80] | RANCZP 2020 [Reference Malhi, Bell and Bassett81] | CINP 2017–2020 [Reference Fountoulakis, Grunze and Vieta82–Reference Fountoulakis, Yatham and Grunze84] | NICE 2020 [85] | |
|---|---|---|---|---|---|
| Acute mania | 1 | 3 | 1 | 2 | 1 Footnote * |
| Prophylaxis: any mood episode | 1 | 1 | 1 | 1 Footnote * | |
| Prophylaxis: mania | 1 | 1 | 1 | 1 | |
| Prophylaxis: depression | 1 | 4 | 1 |
* But not in primary care settings
A Acute Mania
What to Know: Acute Mania
In modern methodologically rigorous acute mania trials, lithium has comparable efficacy to the antipsychotic monotherapy options studied (aripiprazole, quetiapine) and also to divalproex/valproic acid. In clinical practice, lithium is rarely used as monotherapy for acute mania and is typically combined with an antipsychotic.
Newer consensus recommendations suggest lithium levels in the range of 1.00–1.20 mEq/l for acute mania treatment. Higher levels are no longer employed due to the potential adverse renal impact of 12 h trough levels > 1.20 mEq/l, and other tolerability concerns.
Once early publications in 1949–1954 demonstrated lithium’s acute antimanic properties [Reference Schou, Juel-Nielsen and Stromgren86], this was followed by papers noting robust prophylactic effectiveness, with reduction in mood relapses by as much as 90% in studies of various designs, including within-subject mirror-image studies utilizing periods on lithium or on placebo [Reference Schou87]. A 2022 meta-analysis and review of all adult BD trials noted that many of the early acute mania monotherapy studies were open-label, or possessed methodological issues in trial design or outcome reporting that prevent use of meta-analytic statistical methods. Among the 64 acute mania monotherapy studies examined, only five placebo-controlled trials published from 1994 to 2009 were of sufficient quality to merit inclusion in the review, all of which included other comparator arms (VPA, aripiprazole, quetiapine, topiramate) [Reference Fountoulakis, Tohen and Zarate4]. Based on change in the Young Mania Rating Scale (YMRS) total score, lithium monotherapy was clearly superior to placebo for acute mania at mean serum levels ranging from 0.76 to 1.20 mEq/l across those five trials. Superiority of lithium vs. placebo was also seen in the proportion of patients who achieved symptomatic response (≥ 50% reduction in YMRS) or remission (YMRS ≤ 12) at study endpoint [Reference Fountoulakis, Tohen and Zarate4]. For acute mania, lithium was comparable in efficacy to monotherapy SGA options (aripiprazole, quetiapine) and to VPA, and more effective than topiramate, an anticonvulsant whose use as a mood stabilizer has been abandoned. The most common lithium initiation method was to commence with 900 mg/d in divided doses (typically 3 times per day) for the first few days, with flexible dosing from days 3–5 onward based on response and tolerability, while maintaining 12 h trough levels within a target range (e.g. 0.60–1.20 mEq/l, 0.60–1.40 mEq/l, etc.) [Reference Bowden, Brugger and Swann88–Reference Keck, Orsulak and Cutler91]. With this dosing approach, efficacy was seen on average by day 7. These trials reported serum lithium level ranges and mean levels (± a standard deviation), but lacked granular patient-level information to discern what proportion had subtherapeutic levels, and to what extent subtherapeutic levels depressed aggregate lithium response. There was also no exploration of response characteristics (e.g. continuous or categorical response) by serum lithium level [Reference Fountoulakis, Tohen and Zarate4].
Lithium and VPA are the most commonly used mood stabilizing agents as monotherapy, but their efficacy has not been adequately studied in patients diagnosed with mania or hypomania with mixed features using DSM-5 criteria [Reference Rosenblat and McIntyre92]. The RCT literature on mixed BD states is composed exclusively of SGA trials. There are also no prospective RCT data for SAD-BT patients who present with acute mania, although BD-1 clinical trials report that lithium’s antimanic activity exists in patients with and without psychosis [Reference Fountoulakis, Tohen and Zarate4]. Tolerability data indicate that lithium has more adverse effects than placebo (e.g. somnolence, tremor, gastrointestinal complaints) [Reference Fountoulakis, Tohen and Zarate4, Reference McKnight and Chesney93], but a 2019 Cochrane review commented that adequate data on the incidence of adverse events vs. other agents were contained in too few studies to provide high certainty evidence of comparative tolerability [Reference McKnight and Chesney93]. It is worth noting that some acute mania studies allowed lithium levels as high as 1.40 mEq/l or 1.50 mEq/l, somewhat beyond the range used in current practice [Reference Bowden, Brugger and Swann88, Reference Bowden, Grunze and Mullen89].
In-Depth 1.5 The Evidence for Optimal Lithium Serum Levels in Acute Mania
Modern RCTs reinforce the observation from Cade’s 1949 case series that lithium is effective for mania, but the omission of lithium level subanalyses in recent studies did not provide further insight with respect to optimal levels during acute treatment [Reference Cade94]. The absence of modern RCTs randomly assigning acutely manic subjects to target serum level ranges (e.g. 0.80–1.20 mEq/l vs. 1.00–1.20 mEq/l) and the lack of nuanced data from modern double-blind, placebo-controlled RCTs means that any recommended serum level minimum (e.g. ≥ 1.00 mEq/l) or suggested maximum level (e.g. 1.20 mEq/l) during acute mania treatment is not supported by high-quality data. Nevertheless, consensus recommendations for use of higher lithium levels during acute mania treatment are clearly supported by the older literature, but not as strongly as one might surmise [Reference Yatham, Kennedy and Parikh2, Reference Fountoulakis, Yatham and Grunze83]. Achieving a serum level close to 1.00 mEq/l appears a reasonable inference from recent RCTs, while avoiding levels > 1.20 mEq/l is driven by three practical concerns: (1) lithium is rarely prescribed as monotherapy for acute mania, obviating to some extent the need to employ extremely high levels; (2) acute tolerability diminishes significantly at levels > 1.20 mEq/l, so patient exposure to higher levels increases the risk of adverse effects and lithium refusal; (3) evidence from a large retrospective outpatient study (n = 5751) published in 2016 indicated that a single lithium level exceeding 1.20 mEq/l was associated with increased risk of renal insufficiency (odds ratio 1.74, 95% CI 1.33–2.25) [Reference Castro, Roberson and McCoy95].
Supporting the common practice of lithium plus antipsychotic therapy for acute mania are the results of numerous trials showing the superiority of combination therapy over lithium monotherapy, with positive data specifically for haloperidol, asenapine, olanzapine, risperidone, quetiapine and carbamazepine [Reference Malhi, Bell and Bassett81]. Combined treatment also showed superiority over quetiapine monotherapy. The absence of prospective data on combined lithium plus divalproex therapy vs. either agent alone is a gap in the literature, but the few studies suggest additive benefit in acute mania consistent with the robust and comparable antimanic effect of each mood stabilizer as monotherapy [Reference Reischies, Hartikainen and Berghöfer96]. It is for this reason that patients displaying an inadequate mania response despite a lithium level of 1.20 mEq/l and concurrent antipsychotic therapy should be considered candidates to receive an additional first line mood stabilizer for optimal mood control during the acute and maintenance phases of treatment [Reference Wingård, Brandt and Bodén18, Reference Malhi, Bell and Bassett81, Reference Kishi, Ikuta and Matsuda97]. The inability to load carbamazepine and its numerous kinetic interactions with antipsychotics place divalproex in the position as the adjunctive mood stabilizer of choice in these more challenging cases [Reference Meyer, Brunton and Knollmann12]. For clinicians with limited experience in using lithium for acute mania, the modern RCT data convincingly demonstrate that lithium is effective as monotherapy or in combination treatment, and that efficacy is seen within the first week even when an evidence based initiation or loading regimen is not employed (see Info Box 4.3) [Reference Kook, Stimmel and Wilkins7].
B Rapid Cycling
What to Know: Rapid Cycling
The hallmark of rapid cycling bipolar disorder (RC-BD) is frequent depressive episodes of short duration. RC-BD patients will typically not respond completely to any mood stabilizer monotherapy and will require additional medications to manage recurrent bipolar depression.
Lithium is equally effective in decreasing the time spent ill and the number of manic/hypomanic and major depressive episodes in RC-BD patients and non-RC-BD patients; however, RC-BD patients will experience higher numbers of depressive recurrences than non-RC-BD peers, despite having equivalent periods of time without mood episodes.
The limited prospective data indicate that lithium is non-inferior to divalproex, and that the combination of divalproex and lithium is no more effective than lithium monotherapy.
As noted in the 2022 meta-analysis of adult lithium BD trials, “the widely believed concept among clinicians that divalproex is more effective than lithium in the long-term management of rapid-cycling BD was not supported” by the only clinical trial to examine this issue [Reference Calabrese, Shelton and Rapport33]. The current impression that lithium is not inferior to other mood stabilizers for RC-BD maintenance therapy is based on almost 50 years of research that characterized RC-BD as a difficult group to treat with any mood stabilizer monotherapy due to the frequency of depressive episodes [Reference Strawbridge, Kurana and Kerr-Gaffney31]. As of 2022, leading BD experts comment about lithium: “It is equally efficacious in rapid and non-rapid cycling patients” [Reference Fountoulakis, Tohen and Zarate4].
The concept of rapid cycling is a relatively recent one in the world of BD, first elaborated in a 1974 paper [Reference Dunner and Fieve98]. The DSM-5-TR definition requires the presence of at least four mood episodes in the prior 12 months that meet criteria for mania, hypomania or major depression, excluding substance-induced episodes (e.g. due to stimulants, steroids, antidepressants) [Reference Association99]. A 2004 paper provided one of the more complete characterizations of RC-BD patients by analyzing data from the first 500 subjects enrolled in a US National Institute of Mental Health (NIMH) study of BD depression (any BD subtype) for individuals age ≥ 15 years [Reference Sachs, Thase and Otto100, Reference Schneck, Miklowitz and Calabrese101]. This patient pool had a mean age of 41.7 years, with mean age of onset 17.5 years, and 59.4% were female. Of the 500 subjects, 483 could be classified as BD-1 or BD-2, and among the 456 individuals with data on episode frequency, 20% met DSM-IV criteria for rapid cycling in the prior 12 months [Reference Schneck, Miklowitz and Calabrese101]. As seen in Table 1.3, the prevalence of RC-BD was nearly identical in BD-1 and BD-2 patients, and comparable when broken down by gender. Prior to treatment, RC-BD patients had 8-fold higher rates of mood episodes compared with those without rapid cycling, and this was equally true for mania/hypomania as for depressive episodes.
Table 1.3 The clinical course of rapid cycling bipolar disorder (RC-BD) in comparison with BD patients without a history of rapid cycling (n = 500) [Reference Schneck, Miklowitz and Calabrese101]
| BD-1 | BD-2 | Female | Male | BD-1 + substance use disorder | BD-2 + substance use disorder | Age of 1st manic or hypomanic episode | Age of 1st major depressive episode | Number of mood episodes in the prior year: mania or hypomania | Number of mood episodes in the prior year: major depression | |
|---|---|---|---|---|---|---|---|---|---|---|
| RC-BD | 20.0% | 19.8% | 23% | 16% | 41% | 18% | 18.8 ± 9.5 | 16.7 ± 8.7 | 9.0 ± 13.1 | 8.1 ± 11.5 |
| Non-RC-BD | 80.0% | 80.2% | 77% | 84% | 36% | 36% | 22.1 ± 10.0 | 20.0 ± 8.5 | 0.8 ± 0.9 | 1.1 ± 0.9 |
The putative association with lower lithium response rates was first noted in that 1974 paper, and this set the tone for years of misplaced conclusions about lithium’s efficacy by reporting that 9 of 11 (82%) RC-BD patients experienced a mood relapse during follow-up, compared with 18 of 44 (41%) of non-RC-BD individuals [Reference Dunner and Fieve98]. The lack of a comparator arm was one limiting factor in placing the findings in the context of other therapeutic monotherapy options, and much of the subsequent literature was either naturalistic or consisted of post-hoc analyses of an RC-BD subgroup enrolled in other bipolar studies [Reference Strawbridge, Kurana and Kerr-Gaffney31]. As of this writing, RC-BD remains understudied, with only six randomized, controlled prospective studies specifically for RC-BD, many of which are small, statistically underpowered or focus only on those with a specific mood state (e.g. depression) [Reference Fountoulakis, Kontis and Gonda102, Reference Kohler, Friedel and Stamm103].
In-Depth 1.6 Naturalistic Data Supporting Lithium’s Efficacy in Rapid Cycling Bipolar Disorder (RC-BD)
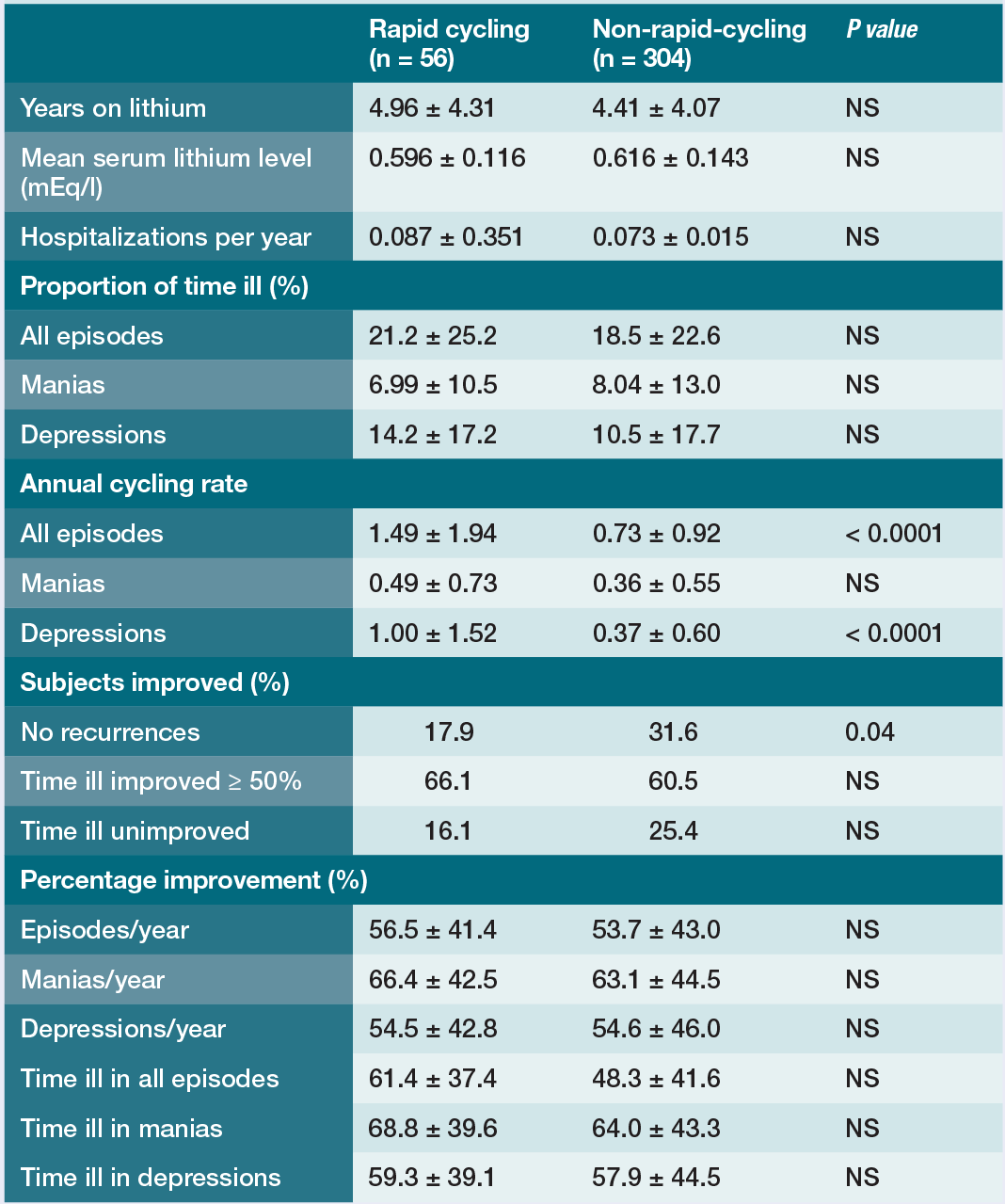
By the year 2000, there was an inkling that any issues with lithium response in RC-BD lay in the phenomenology of the disorder itself, based on a study of naturalistic outcomes with lithium treatment in RC-BD and non-RC-BD adults [Reference Baldessarini, Tondo and Floris32]. The subjects of this analysis were 360 BD-1 or BD-2 adults followed from 1974 to 1998 in a Stanley Foundation Network study in Sardinia, which excluded from the analysis any individual who used other mood agents for 8 or more weeks at any time. The total sample had the following characteristics: BD-1: 60.6%; BD-2: 39.4%; 63.6% female. There was a mean of 8.83 ± 8.38 years of historical mood information available for the subjects prior to study entry, and a mean 4.49 ± 4.10 years of follow-up data on lithium [Reference Baldessarini, Tondo and Floris32]. Among the sample of 360 subjects, 15.6% had a lifetime RC-BD diagnosis based on ≥ 4 mood episodes in any year, with 30.4% averaging ≥ 4 mood episodes per year [Reference Baldessarini, Tondo and Floris32]. As seen in Table 1.4, clinical outcomes of the RC-BD and non-RC-BD groups on lithium were comparable, including the proportion of time spent ill, the annual rate of mania, the annual number of hospitalizations, and the percentage improvement in time spent ill [Reference Baldessarini, Tondo and Floris32]. Among all subjects, the percentage of time spent ill on lithium did not correlate with the pre-lithium cycling rate, and for the RC-BD cohort the percentage of time spent ill did not correlate with RC-BD status (i.e. the prior 12 months vs. historical), or pre-lithium mood episode frequency. For those with ≥ 3.5 episodes/year, 23.0 ± 27.9% of the time was spent ill on lithium compared with 18.6 ± 22.7% for those with fewer annual episodes (p = 0.762). However, lithium treated RC-BD patients had 3 times more depressive episodes per year, and fewer RC-BD patients had zero mood recurrences during follow-up compared with the non-RC-BD group (17.9% vs. 31.6%, p = 0.04).
Table 1.4 Comparison of RC-BD and non-RC-BD outcomes on lithium during routine long-term treatment [Reference Baldessarini, Tondo and Floris32]
| Rapid cycling (n = 56) | Non-rapid-cycling (n = 304) | P value | |
|---|---|---|---|
| Years on lithium | 4.96 ± 4.31 | 4.41 ± 4.07 | NS |
| Mean serum lithium level (mEq/l) | 0.596 ± 0.116 | 0.616 ± 0.143 | NS |
| Hospitalizations per year | 0.087 ± 0.351 | 0.073 ± 0.015 | NS |
| Proportion of time ill (%) | |||
| All episodes | 21.2 ± 25.2 | 18.5 ± 22.6 | NS |
| Manias | 6.99 ± 10.5 | 8.04 ± 13.0 | NS |
| Depressions | 14.2 ± 17.2 | 10.5 ± 17.7 | NS |
| Annual cycling rate | |||
| All episodes | 1.49 ± 1.94 | 0.73 ± 0.92 | < 0.0001 |
| Manias | 0.49 ± 0.73 | 0.36 ± 0.55 | NS |
| Depressions | 1.00 ± 1.52 | 0.37 ± 0.60 | < 0.0001 |
| Subjects improved (%) | |||
| No recurrences | 17.9 | 31.6 | 0.04 |
| Time ill improved ≥ 50% | 66.1 | 60.5 | NS |
| Time ill unimproved | 16.1 | 25.4 | NS |
| Percentage improvement (%) | |||
| Episodes/year | 56.5 ± 41.4 | 53.7 ± 43.0 | NS |
| Manias/year | 66.4 ± 42.5 | 63.1 ± 44.5 | NS |
| Depressions/year | 54.5 ± 42.8 | 54.6 ± 46.0 | NS |
| Time ill in all episodes | 61.4 ± 37.4 | 48.3 ± 41.6 | NS |
| Time ill in manias | 68.8 ± 39.6 | 64.0 ± 43.3 | NS |
| Time ill in depressions | 59.3 ± 39.1 | 57.9 ± 44.5 | NS |
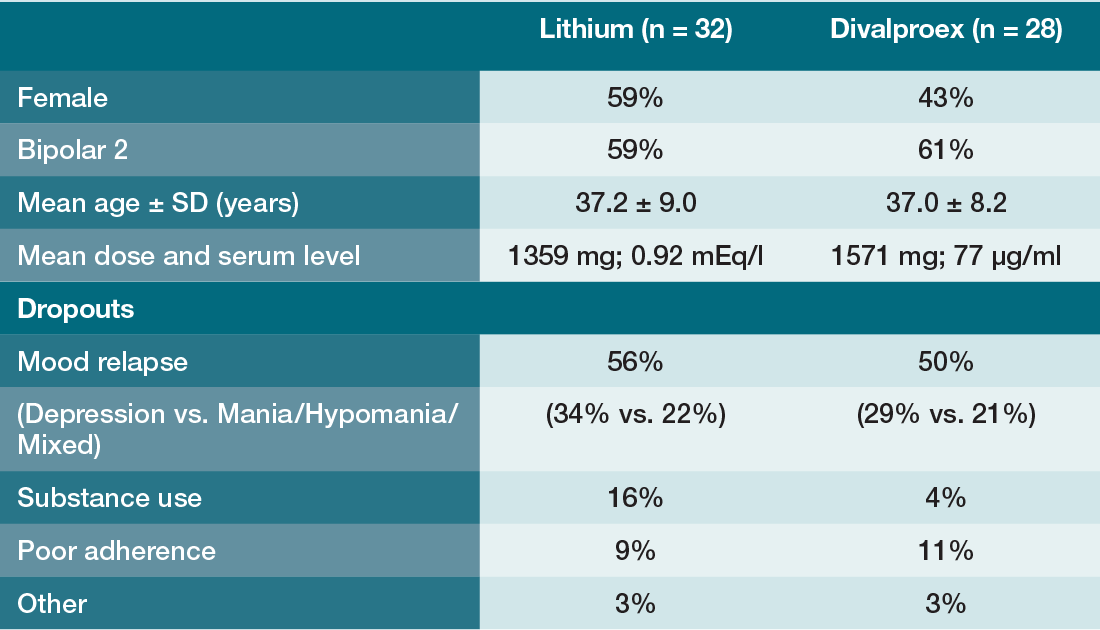
Nonetheless, well-designed prospective studies have provided the necessary comparative data to indicate that lithium is noninferior to divalproex monotherapy for RC-BD patients, and that the combination of lithium and divalproex is no more effective for these patients than lithium monotherapy. The first study was a 20-month, double-blind maintenance trial of lithium vs. divalproex in RC-BD disorder that enrolled 254 RC-BD adults with BD-1 or BD-2, with rapid cycling defined as a history of ≥ 4 episodes in the past 12 months, and at least one episode of mania or hypomania or a mixed episode in the 3 months prior to study entry [Reference Calabrese, Shelton and Rapport33]. Study exclusions included a prior history of combined lithium and divalproex use, history of intolerance to a lithium level 0.80 mEq/l or to a VPA level of 50 µg/ml, substance dependence criteria for alcohol or drugs in the prior 6 months, and patients who were on steroids or were pregnant or planning to become pregnant. The 2-phase study design included an open-label stabilization phase in which subjects were initially titrated on lithium to a target level of 0.80 mEq/l over 4–6 weeks, then divalproex was added to a target level of 50 µg/ml over 4–6 weeks. During this phase, 28% were lost due to poor adherence, 26% were lost due to symptom nonresponse (19% depression, 7% mania/hypomania/mixed), and 19% dropped out due to adverse effects. Subjects who maintained stability for 4 consecutive weeks were entered into the double-blind maintenance phase based on having a Hamilton Depression Scale (HAM-D24) score ≤ 20, a YMRS score ≤ 12, and serum drug levels at or above the target levels. Only 24% (n = 60) met these criteria and were randomized to lithium or divalproex, stratified by BD-1 or BD-2 subtype [Reference Calabrese, Shelton and Rapport33]. As seen in Table 1.5, there were no-between group differences in time to treatment for a mood episode or time to discontinuation for any reason, nor was there any impact of BD-1 or BD-2 subtype diagnosis. The authors’ conclusion is worth repeating verbatim: “The hypothesis that divalproex is more effective than lithium in the long-term management of rapid-cycling bipolar disorder is not supported by these data. Preliminary data suggest highly recurrent refractory depression may be the hallmark of rapid-cycling bipolar disorder” [Reference Calabrese, Shelton and Rapport33].
Table 1.5 Outcomes from the double-blind maintenance phase of a 20-month RC-BD trial [Reference Calabrese, Shelton and Rapport33]
| Lithium (n = 32) | Divalproex (n = 28) | |
|---|---|---|
| Female | 59% | 43% |
| Bipolar 2 | 59% | 61% |
| Mean age ± SD (years) | 37.2 ± 9.0 | 37.0 ± 8.2 |
| Mean dose and serum level | 1359 mg; 0.92 mEq/l | 1571 mg; 77 µg/ml |
| Dropouts | ||
| Mood relapse | 56% | 50% |
| (Depression vs. Mania/Hypomania/Mixed) | (34% vs. 22%) | (29% vs. 21%) |
| Substance use | 16% | 4% |
| Poor adherence | 9% | 11% |
| Other | 3% | 3% |
In-Depth 1.7 The Combination of Divalproex and Lithium is No More Effective than Lithium Monotherapy in RC-BD Patients with Substance Use Disorders
The second well-designed prospective RC-BD study was a 6-month, double-blind, maintenance trial of lithium monotherapy vs. the combination of lithium and divalproex in RC-BD patients with co-occurring substance abuse or dependence [Reference Kemp, Gao and Ganocy34]. The exclusions and methods were identical to the prior 2-phase monotherapy RC-BD study with the only exception that subjects must have had alcohol, cocaine or cannabis abuse within the prior 3 months, or dependence within the prior 6 months by DSM-IV criteria. In the open-label stabilization phase 149 patients were enrolled, and 42% were lost due to poor adherence, 25% lost for inadequate symptom nonresponse (13% depression, 12% mania/hypomania/mixed), and 10% dropped out due to adverse effects. Only 21% (n = 31) of the sample met stability criteria and were subsequently randomized in the double-blind maintenance phase to lithium monotherapy or lithium and divalproex combination therapy, stratified by BD-1 or BD-2 subtype. This trial found no between-group differences in the time to treatment for a mood episode, time to discontinuation for any reason, nor was there any impact of BD-1 vs. BD-2 diagnosis (Table 1.6) [Reference Kemp, Gao and Ganocy34]. While the small sample size in the double-blind phase increases the likelihood of type II error, this study illustrates the challenges in treating RC-BD patients with substance use comorbidity while providing controlled data suggesting that adding divalproex to lithium does not markedly enhance lithium’s effectiveness in these patients.
Table 1.6 Data from the double-blind maintenance phase of a trial comparing lithium monotherapy vs. the combination of lithium and divalproex for RC-BD patients with co-occurring substance abuse or dependence [Reference Kemp, Gao and Ganocy34]
| Lithium (n = 16) | Lithium + divalproex (n = 15) | |
|---|---|---|
| Female | 25% | 40% |
| Bipolar 2 | 19% | 13% |
| Mean age ± SD (years) | 40.0 ± 10.6 | 37.1 ± 10.9 |
| Mean dose and serum level | 1440 mg; 0.88 mEq/l |
|
| Dropouts | ||
| Mood relapse (Depression vs. Mania/Hypomania/Mixed) |
|
|
| Poor adherence | 12% | 13% |
| Other | 12% | 0% |
One small maintenance study noted that adding carbamazepine to lithium may be more effective than lithium monotherapy in RC-BD patients, and a trial of quetiapine added to lithium or divalproex in RC-BD-1 patients found that these combinations were effective and well tolerated [Reference Fountoulakis, Tohen and Zarate4]. Given quetiapine’s monotherapy indication for BD-1 and BD-2 depression, that result outlines a rational pharmacological approach to long-term RC-BD management, emphasizing the need to use combination therapy, and especially a combination with lithium that adds an agent to address the highly recurrent and difficult to treat depressive phases of the illness. That RC-BD is a predictor of inadequate response to lithium monotherapy can now be understood in the context of these trials – no monotherapy is likely to be effective in this population, but the available data indicate that lithium treated RC-BD patients will fare no worse than RC-BD patients on other monotherapies [Reference Strawbridge, Kurana and Kerr-Gaffney31, Reference Nunes, Ardau and Berghofer104].
C Acute Bipolar Depression and Bipolar II Disorder (BD-2)
What to Know: Acute Bipolar Depression and Bipolar II Disorder (BD-2)
Lithium reduces depressive mood recurrence, but modern data do not strongly support its efficacy when used for acute bipolar depression.
The treatment of BD-2 is nuanced. In those who require mood stabilization, lithium is the preferred agent at trough levels of 0.60–0.80 mEq/l, and possibly in the range of 0.40–0.60 mEq/l given tolerability concerns seen in a trial with a target lithium level of 0.80 mEq/l.
Some BD-2 patients may not require a mood stabilizer and both tolerate and respond to traditional antidepressants.
Lithium possesses antidepressant properties, but the question is to what extent lithium is a proven effective option in acute BD depression. This is a question of relevance to the treatment of BD-1/SAD-BT and BD-2 patients for two reasons: (1) lithium utilization is so low across the BD spectrum that lithium emerges as an available adjunctive option to be considered for acutely depressed BD patients [Reference Poranen, Koistinaho and Tanskanen5]; (2) when experiencing a mood episode, BD-2 patients spend a disproportionate amount of time depressed compared with that in hypomania or a mixed state, so any use of lithium is likely to be for an acute depressive episode (Figure 1.2) [Reference Judd, Akiskal and Schettler27, Reference Judd, Akiskal and Schettler28]. Despite the extensive use of lithium during decades when no other mood stabilizing option existed, the 10 older studies of lithium monotherapy for acute bipolar depression were not conducted using modern RCT methods, thus limiting their interpretability [Reference Fountoulakis, Tohen and Zarate4]. There is a recent RCT published in 2010 that reported outcomes from a double-blind, 8-week trial which randomized 802 acutely depressed BD subjects (BD-1, n = 499; BD-2, n = 303) to one of 4 treatment arms: quetiapine 300 mg/d (n = 265), quetiapine 600 mg/d (n = 268), lithium 600–1800 mg/d (n = 136) or placebo (n = 133) [Reference Young, McElroy and Bauer38]. The mean age was 42.2 years, and 59.3% of patients were female. While the efficacy results were positive for quetiapine, they were not for lithium treated subjects (mean serum level 0.61 mEq/l). As 34.9% of those in the lithium cohort had levels < 0.60 mEq/l, secondary analyses were performed for those with lithium levels > 0.80 mEq/l and for lithium treated study completers, but the findings were also negative, suggesting lithium is not effective for acute bipolar depression regardless of level or treatment duration [Reference Young, McElroy and Bauer38]. Traditional antidepressants present a considerable risk when administered to BD-1 or SAD-BT patients due to possible switching into a hypomanic, mixed or manic episode [Reference Allain, Leven and Falissard105], so other options are preferable for acute bipolar depression in those patients: cariprazine, lumateperone, lurasidone, and possibly quetiapine or the olanzapine/fluoxetine combination, although the latter two choices are eschewed due to significant weight gain, metabolic dysfunction and sedation [Reference Meyer, Brunton and Knollmann12, Reference Doane, Bessonova and Friedler106].
In-Depth 1.8 Bipolar II Depression and Antidepressant Use
The approach to BD-2 depression is qualitatively different than for BD-1/SAD-BT patients as the risk of antidepressant related switching is lower, though not absent [Reference Allain, Leven and Falissard105, Reference Leverich, Altshuler and Frye107]. Recent evidence for this assertion comes from two double-blind RCTs that examined the comparative efficacy of venlafaxine or sertraline vs. lithium in acute BD-2 depression. The first was a randomized, double-blind, 12-week study of adult outpatients in which lithium treated subjects (n = 64) experienced lower response rates than those randomized to venlafaxine (n = 65) (34.4% vs. 67.7% respectively; p < 0.001), and lower remission rates (28.1% vs. 58.5% respectively; p < 0.001), with no significant between-group differences in the emergence of hypomania symptoms [Reference Amsterdam, Lorenzo-Luaces and Soeller29]. The second study was a 16-week, double-blind trial in which 142 adults with BD-2 depression were randomly assigned to lithium monotherapy (n = 49), sertraline monotherapy (n = 45) or combination treatment with lithium and sertraline (n = 48) [Reference Altshuler, Sugar and McElroy108]. The treatment response rate for the overall sample was 62.7% without significant between-group differences after accounting for dropouts. The lithium + sertraline combination cohort also experienced a significantly greater dropout rate than the monotherapy arms but without any efficacy benefit as measured by the extent of response or the time to response. Although 20 subjects (14%) did switch into hypomania, the switch rates did not differ between the 3 treatment arms even after accounting for dropouts, and no patient had a manic switch or was hospitalized for a switch [Reference Altshuler, Sugar and McElroy108]. From the limited data, one can conclude that BD-2 patients should consider options other than lithium for acute depression if unable to tolerate antidepressants due to switching. It is worth noting that two of the agents approved for BD-1 depression also have indications for BD-2 depression: quetiapine (monotherapy) and lumateperone (monotherapy or adjunctive to lithium or divalproex) [Reference Meyer, Brunton and Knollmann12].
A certain proportion of BD-2 patients will not tolerate traditional antidepressants due to the emergence of hypomania or a mixed state, and thus function best when chronically mood stabilized (see In-Depth 1.8); however, there are no double-blind BD-2 maintenance RCTs involving lithium, although there are two open-label studies. In one long-term study published in 1999, lithium and carbamazepine maintenance monotherapies were compared over 2.5 years in 57 patients with BD-2 or BD not otherwise specified (using DSM-IV terminology and criteria) [Reference Greil and Kleindienst109]. This trial found no significant differences between lithium and carbamazepine in rates of mood recurrences, subclinical mood episodes, psychiatric hospitalizations, need for concomitant medications or severe adverse effects [Reference Greil and Kleindienst109]. A 2021 single-blind 20-week study enrolled 44 subjects with newly diagnosed BD-2 and randomly assigned them to lithium (target serum level 0.80 mEq/l) or lamotrigine (target dose 200 mg/d) [Reference Parker, Ricciardi and Tavella22]. This study was terminated early due to greater rates of adverse effects in the lithium arm, although several subjects assigned to lamotrigine experienced psychosis. Analyses of study completer data for 28 participants suggested comparable efficacy of both medications [Reference Parker, Ricciardi and Tavella22]. Should lithium be used for BD-2 maintenance, strong consideration should be given to use of levels at the low end of the maintenance range (0.60–0.80 mEq/l), and possibly even to levels in the range of 0.40–0.60 mEq/l given the tolerability concerns raised in a BD-2 trial employing a target lithium level of 0.80 mEq/l [Reference Parker, Ricciardi and Tavella22].
In-Depth 1.9 Lithium Discontinuation and the Risk for Psychiatric Hospitalization in BD-1 vs. BD-2: A Retrospective Study
A Swedish group retrospectively examined psychiatric outcomes in 194 lithium treated individuals who had clinical data 2 years before and 2 years after lithium discontinuation, with the data broken down by BD subtype [Reference Öhlund, Ott and Bergqvist21]. In the 2 years after lithium discontinuation, 51% of patients with BD-I/SAD-BT (n = 100) and 46% with BD-2 / other BD (n = 94) were on an alternative mood stabilizer. Using the primary outcome measure of psychiatric hospitalization, the BD-1/SAD-BT patient cohort experienced a significant increase in the percentage who were admitted and in total number of admissions, but the BD-2 /other BD cohort did not experience a significant change in those outcomes after lithium discontinuation [Reference Öhlund, Ott and Bergqvist21]. Unfortunately, the use of psychiatric hospitalization as the only metric for mood recurrence obscures the extent and severity of mood relapses for the BD-2 group since they are less commonly hospitalized, so the true impact of lithium discontinuation on any BD-2 patient who requires mood stabilization is not easily quantifiable from the literature.
In-Depth 1.10 Newer Concerns About Lamotrigine’s Safety
Lamotrigine lacks lithium’s monitoring burdens and has therefore become a more popular option for BD patients in general over the past two decades, despite the fact that it is only approved for BD-1 maintenance [Reference Poranen, Koistinaho and Tanskanen5]. Lamotrigine has its own safety concerns, including the risk of Stevens–Johnson Syndrome/toxic epidermal necrolysis, aseptic meningitis, hemophagocytic lymphohistiocytosis, and recent warnings issued in 2021 based on in vitro testing showing that it possesses class IB antiarrhythmic activity at therapeutic concentrations [110]. While QRS widening has not been observed in healthy individuals, the concern was that lamotrigine could slow ventricular conduction leading to arrhythmias and possible sudden death in patients with significant heart disease, including conduction system disorders, a history of ventricular arrhythmias, cardiac channelopathies (e.g. Brugada syndrome), ischemic heart disease or multiple coronary artery disease risk factors [110]. The clinical data informing this issue are limited as none of the 26 studies involving lamotrigine (n = 2326) examined risks in people with pre-existing cardiac conditions, so there is insufficient evidence to support or refute any association of lamotrigine with sudden death or ECG changes [Reference Bunschoten, Husein and Devinsky111].
D Bipolar Disorder Maintenance and Response Prediction
What to Know: Bipolar Disorder Maintenance and Response Prediction
Randomized trials document lithium’s efficacy for BD-1 maintenance, but modern studies often incorporate preferential responders to other agents (e.g. lamotrigine, quetiapine), limiting the ability to make comparative statements about lithium's efficacy.
Real world data sets do support the concept that BD-1 patients have superior outcomes on lithium compared to monotherapy with an SGA or valproate.
Certain clinical features such as substance use, personality disorder, illness chronicity, rapid cycling or inadequate social support limit response to treatment in general, and are not necessarily lithium specific. Patients with these clinical characteristics should not be deprived of a lithium trial because they are not “ideal candidates.”
1 Maintenance Studies
The 2022 meta-analysis of adult lithium BD trials found 21 monotherapy maintenance studies, but the use of obsolete study designs and other methodological issues in older literature limited their analysis to 4 modern RCTs [Reference Fountoulakis, Tohen and Zarate4]. One of these studies was a negative study in which 372 adult BD-1 patients who met recovery criteria within 3 months of the onset of a manic episode were randomized to 12 months of maintenance treatment with divalproex, lithium or placebo in a 2:1:1 ratio [Reference Bowden, Calabrese and McElroy112]. Despite the larger sample size for the divalproex arm, the divalproex group did not differ significantly from the placebo group in time to any mood episode, and the same was true for the lithium cohort [Reference Bowden, Calabrese and McElroy112]. In 2003, two subsequent papers were published which separately reported positive outcomes from placebo-controlled 18-month maintenance studies of lamotrigine and lithium maintenance treatment in BD-1 patients who were recently manic/hypomanic [Reference Bowden, Calabrese and Sachs113], or recently depressed [Reference Calabrese, Bowden and Sachs39]. As these were industry sponsored studies pursuing BD-1 maintenance indications for lamotrigine, patients began each study with an 8- to 16-week open-label phase during which lamotrigine was initiated and other psychotropics discontinued. Stable patients on lamotrigine monotherapy were subsequently randomized to lamotrigine (50, 200 or 400 mg/d if the most recent episode was depressed, 100–400 mg/d if the most recent episode was manic/hypomanic), lithium (0.80–1.10 mEq/l) or placebo as double-blind maintenance treatment for as long as 18 months. In the trial where the most recent mood episode was mania/hypomania, 349 patients entered the open-label phase, 175 met stabilization criteria and were randomized to lamotrigine (n = 59), lithium (n = 46) or placebo (n = 70) [Reference Bowden, Calabrese and Sachs113]. Although the study was performed in lamotrigine responders, both lamotrigine and lithium were superior to placebo at prolonging the time to intervention for any mood episode (lamotrigine vs. placebo, p = 0.02; lithium vs. placebo, p = 0.006). Lamotrigine was superior to placebo at prolonging the time to a depressive episode (p = 0.02), while lithium was superior to placebo at prolonging the time to a manic, hypomanic or mixed episode (p = 0.006) [Reference Bowden, Calabrese and Sachs113]. In the trial where the most recent mood episode was depression, 966 BD-1 patients entered the open-label phase, 463 met stabilization criteria and were randomized to lamotrigine (n = 221), lithium (n = 121) or placebo (n = 121) [Reference Calabrese, Bowden and Sachs39]. The time to intervention for any mood episode was statistically superior (p = 0.029) for both lamotrigine and lithium compared with placebo, and the median survival times were 200, 170, and 93 days, respectively. Lamotrigine was superior to placebo at prolonging the time to intervention for a depressive episode (p = 0.047), but the proportions of patients who were intervention-free for depression at 1 year were not significantly different between the three arms: lamotrigine 57%, lithium 46%, and placebo 45%. Lithium was statistically superior to placebo at prolonging the time to intervention for a manic or hypomanic episode (p = 0.026) [Reference Calabrese, Bowden and Sachs39].
There was also one trial involving continuation of quetiapine vs. switching to placebo or lithium for maintenance treatment of BD-1 patients [Reference Weisler, Nolen and Neijber37]. That trial design involved stabilizing adult patients experiencing any recent mood episode (mania, mixed, depressive) on open-label quetiapine (300–800 mg/d) for 4–24 weeks, with those achieving stabilization then randomized in a double-blind manner to continue quetiapine or to switch to placebo or lithium (0.60–1.20 mEq/L) for up to 104 weeks [Reference Weisler, Nolen and Neijber37]. Only 50% of the initial 2438 patients could be stabilized and randomized to double-blind treatment (n = 1172). Quetiapine and lithium significantly increased the time to recurrence of manic events (quetiapine HR 0.29; 95% CI 0.21–0.40; p < 0.0001; lithium HR 0.37; 95% CI 0.27–0.53; p < 0.0001) and depressive events (quetiapine HR 0.30; 95% CI 0.20–0.44; p < 0.0001; lithium HR 0.59; 95% CI 0.42–0.84; p < 0.004), compared with placebo [Reference Weisler, Nolen and Neijber37]. That the study used a pool of patients who were quetiapine responders limits generalizability, as does the fact that 50% of the sample was lost during the stabilization phase. The indisputable fact is that quetiapine is better than placebo in BD-1 patients who respond to it as monotherapy, but in modern practice the use of quetiapine as BD-1 monotherapy is an unlikely scenario.
In-Depth 1.11 What Is Propensity Score Matching ?
As only one maintenance RCT provided an SGA comparator, and that study used quetiapine responders, clinicians might wonder whether there are any other data to provide relevant comparisons between lithium and maintenance SGA use, especially for BD-1 patients. Real world data sets present a naturalistic picture of medication outcomes, and modern statistical methods permit analyses that remove biases for or against prescribing a particular treatment by employing propensity score matching. (The details of this method are discussed extensively in Info Box 7.6, as is the use of propensity score matching in analyses of major congenital malformation rates with 1st trimester psychotropic exposure.) There are numerous reasons why clinicians choose a particular medication for a patient, but when retrospectively examining a set of new medication prescriptions, one can construct a statistical model based on the pattern of usage in that population that describes the likelihood a particular patient might have been prescribed a specific medication. From this logistic regression model, one can then take the characteristics of any individual subject and calculate what their propensity would have been to receive a specific treatment on a scale of 0 to 1.0. Essentially, this propensity score represents the probability that an individual would be assigned to a treatment based on their demographics and comorbidities present at that time [Reference Deb, Austin and Tu114]. Not uncommonly, two individuals can have identical propensity scores for receiving a treatment (e.g. lithium), yet one was given this medication and one was not. One can therefore match exposed and unexposed individuals by their propensity scores, and in doing so balance the treatment cohorts for their likelihood to have received a treatment in the manner that a prospective trial balances this likelihood (e.g. by using a 1:1:1 randomization scheme).
In-Depth 1.12 Lithium vs. Second Generation Antipsychotics for Maintenance Therapy in BD-1 Patients: Real World Outcomes Using Propensity Score Matching
Using a propensity score matched analysis, a population based cohort study was performed from electronic health records of 5089 UK BD patients prescribed lithium (n = 1505), VPA (n = 1173), olanzapine (n = 1366) or quetiapine (n = 1075) as monotherapy [Reference Hayes, Marston and Walters115]. Treatment failure was defined as time to stopping medication or the need to add another mood stabilizer, antipsychotic, antidepressant or benzodiazepine. In unadjusted analyses, the duration of successful monotherapy was longest for lithium treated patients, with treatment failure not occurring in 75% of those prescribed lithium for 2.05 years (95% CI 1.63–2.51), vs. 1.13 years for olanzapine (95% CI: 1.00–1.31), 0.98 years for VPA (95% CI 0.84–1.18), and 0.76 years (95% CI 0.64–0.84) for quetiapine (Figure 1.3) [Reference Hayes, Marston and Walters115]. Lithium’s superiority remained in the propensity score matched analysis, and in sensitivity analyses where treatment failure was defined strictly as stopping the medication or adding a mood stabilizer or antipsychotic, or when treatment failure was restricted to more than 3 months after commencing the particular medication.

Figure 1.3 Time to treatment failure (defined as treatment discontinuation, or the need to add a mood stabilizer, antipsychotic, antidepressant or benzodiazepine) among 5089 British adults with BD prescribed lithium (n = 1505), valproate (n = 1173), olanzapine (n = 1366) or quetiapine (n = 1075) as monotherapy. [115]
Another method of defining treatment failure is rehospitalization, and this outcome was tracked in 18,018 Finnish patients previously hospitalized for BD, from 1996 to 2012 [Reference Lahteenvuo, Tanskanen and Taipale6]. As mentioned in the chapter introduction, this study performed a within-individual analysis to examine hospitalization risk during periods on or off various treatments, with each patient serving as his or her own control. Over a mean follow-up of 7.2 years, lithium was the most effective mood stabilizer in preventing psychiatric rehospitalization (Table 1.1), but efficacy was not seen for VPA or for any anticonvulsant other than carbamazepine [Reference Lahteenvuo, Tanskanen and Taipale6].
As many BD-1 patients are placed on SGAs during an acute manic/mixed episode, a Swedish group examined long-term naturalistic outcomes following a hospitalization for mania among those on monotherapy with a mood stabilizer or SGA, and for those on combination treatment [Reference Wingård, Brandt and Bodén18]. This study used data from 3772 adults aged 18–75 with a primary diagnosis of a manic episode (ICD-10 F30.1–F30.9, and F31.1–F31.2) who were discharged from psychiatric inpatient care from July 1, 2006 to December 31, 2014. Compared with lithium monotherapy, VPA monotherapy had a higher rate of medication discontinuation, while all SGA monotherapies were associated with higher rates of all-cause treatment failure and failure due to medication switching (Figure 1.4) [Reference Wingård, Brandt and Bodén18]. Speaking to the challenges in treating BD-1 patients, the risks for overall treatment failure were significantly lower for combination therapy, but only the combination of lithium + VPA + quetiapine was associated with a significantly lower rehospitalization risk during ongoing treatment compared with lithium monotherapy (AHR 0.57, 95% CI 0.32–0.99). Importantly, use of antidepressants in the prior year for these BD-1 patients increased risk of treatment failure (adjusted hazard ratio [AHR] 1.24, 95% CI 1.16–1.33), but use of a depot antipsychotic in combination lowered risk of treatment failure (AHR 0.79, 95% CI 0.68–0.93), as did a long index hospitalization exceeding 42 days (AHR 0.81, 95% CI 0.76–0.88) [Reference Wingård, Brandt and Bodén18]. These real world studies from three different countries reinforce the notion that lithium is the preferred maintenance treatment for BD, especially for BD-1 patients, with clinical outcomes superior to SGA or VPA monotherapy using varying definitions of treatment failure.

Figure 1.4 Time to treatment failure after hospitalization for mania among various treatment options for BD-1 using lithium (dark blue line) as the comparator treatment [18]
In-Depth 1.13 Detailed Methods of the Swedish Study Examining Naturalistic Outcomes during Post-Mania Treatment with Psychotropic Monotherapy or Combinations [18]
Dementia, or those with schizophrenia or SAD-BT diagnoses, were excluded from the analysis, and patients hospitalized for mania multiple times were examined following each hospitalization, with hospitalizations for mania less than 7 days apart linked and counted as one episode. (Among the sample of 3772 patients, 1041 individuals contributed two or more hospitalizations.) After each hospitalization for mania, active treatment periods of lithium, VPA, olanzapine, quetiapine or aripiprazole, alone or in combination, were recorded. Each active treatment period was defined as starting on the day of a prescription fill of any of the medications, or the day of discharge if the patient filled a prescription during the index hospitalization. Patients who filled prescriptions of more than one drug within 2 weeks were considered to use combination therapy. Follow-up started on day 14 of the first active treatment period and ended after 365 days or upon the earliest of any of the following events: treatment failure, emigration, death or the end of the study period (December 31, 2014). In this study, treatment failure was defined as medication discontinuation or switching, or being readmitted to inpatient psychiatric care during an active treatment period. This study did not use propensity score matching but did examine an extensive list of covariates related to sociodemographic variables, severity of the index hospitalization, psychiatric history and comorbidities, history of self-harm and use of other psychotropics [Reference Wingård, Brandt and Bodén18]. 17.6% of subjects were under 30 years of age, 24.5% were aged 30–44 years, and 57.9% were age 45 or older, and 57.1% of the sample was female. Most parameters were evenly distributed, but aripiprazole monotherapy patients were younger, while those with a first manic episode or who were naïve to antimanic drugs were overrepresented in the olanzapine group. The total follow-up time comprised 1773 patient-years, and treatment failure within 1 year was seen in 85.3% of patients. Of these, 2667 switched treatment, 1108 discontinued treatment and 1096 were rehospitalized despite ongoing treatment.
2 The Search for Response Predictors
As discussed extensively in Chapters 2 and 4, the perception of lithium’s long-term renal risks has shifted significantly based on two realizations: (1) some of the risks for renal dysfunction were related to prior prescribing practices, such as use of high maintenance lithium levels and multiple daily dosing; and (2) the absence of systematic laboratory monitoring protocols [Reference Aiff, Attman and Aurell116]. Modern treatment guidelines emphasize regular monitoring and the use of more modest maintenance levels [Reference Nolen, Licht and Young117, Reference Schoot, Molmans and Grootens118], with the result that recent studies show that mean annual declines in estimated glomerular filtration rate (eGFR) are predicted primarily by medical comorbidities that increase chronic kidney disease (CKD) risk, exposure to nephrotoxic drugs and episodes of lithium toxicity, but not necessarily duration of lithium exposure [Reference Castro, Roberson and McCoy95, Reference Clos, Rauchhaus and Severn119–Reference Fransson, Werneke and Harju121].
Nonetheless, concerns over lithium’s safety were often a driver for studies that aimed to define “ideal” lithium candidates, with the goal of sparing individuals a lithium trial where the benefits might be outweighed by the risks. While the development of robust response predictors to drug therapy is the holy grail of psychiatric practice, a significant proportion of the lithium related clinical research was confined to monotherapy analyses, despite the recognition that many BD spectrum patients require combination therapy, especially to manage or prevent depressive episodes [Reference Wingård, Brandt and Bodén18, Reference Calabrese, Shelton and Rapport33, Reference Lin, Maihofer and Stapp74, Reference Kessing, Hellmund and Andersen122]. Moreover, the finding that certain clinical features – such as substance use, personality disorder, illness chronicity, rapid cycling or inadequate social support – might negatively impact lithium response relates to aspects of BD patients that limit response to treatment in general, and are not necessarily lithium specific [Reference Malhi, Gessler and Outhred1, Reference Hui, Kandola and Shen30, Reference Lin, Maihofer and Stapp74, Reference Nunes, Ardau and Berghofer104, Reference Grillault Laroche, Etain and Severus123, Reference Scott, Bellivier and Manchia124]. Unfortunately, the absence of a comparator arm often paints a dismal portrait of the chances for lithium success [Reference Kessing, Hellmund and Andersen122]; however, as discussed in the section on RC-BD, when studies are designed to examine response in challenging patient cohorts, the picture that emerges is not lithium’s lack of efficacy, but the limited efficacy of any monotherapy [Reference Calabrese, Shelton and Rapport33, Reference Kemp, Gao and Ganocy34, Reference Calabrese, Suppes and Bowden125]. The presence of comorbidities that limit adherence with specific aspects of treatment (e.g. laboratory monitoring) will certainly factor into the decision to use lithium, yet current recommendations no longer focus on restricting lithium to ideal candidates for excellent monotherapy response, but on employing lithium as the preferred foundational mood stabilizer in any patient with a history of mania, and for BD-2 patients who require mood stabilization [Reference Malhi, Bell and Bassett81]. Alcohol use disorders, personality disorders, higher number of psychiatric admissions and rapid cycling are negative prognostic indicators of lithium monotherapy response, but patients should not be deprived of a lithium trial a priori due to the presence of these factors, especially where the data do not suggest superior outcomes for other medications in BD spectrum patients with these clinical features. Ideally, the database on clinical response predictors will enlarge over time to provide comparable analyses for divalproex and SGA monotherapies that mirror the approaches to predicting lithium monotherapy response.
In-Depth 1.14 Biomarker Studies of Lithium Response
Biomarker studies represent another important avenue of research that might provide insights into the biosignatures of lithium response and tolerability. Investigators are using a variety of avenues to tackle these issues, including polygenic risk scores, individual genetic markers, imaging findings, and novel methods such as the association between circadian rhythms in cultured patient neurons and lithium response [Reference Hou, Heilbronner and Degenhardt70, Reference McCarthy, Wei and Nievergelt73, Reference Mishra, Ying and Luis75]. One hopes that this research will mature sufficiently to provide robust predictors for a variety of mood stabilizing and other biological therapies employed in the management of BD, but at the present time we must rely on the evidence based indications for lithium to inform our decision to start lithium, especially given the extent of RCT and real world studies demonstrating comparative advantages over other medication options.
The role of treatment delay in lithium response is a subject of debate covered more extensively in Chapter 4. It is worth noting that examining longitudinal effects of any specific medication is challenging due to the episodic nature of BD and periods of spontaneous remission [Reference Baldessarini, Tondo and Baethge126]. Nonetheless, a 2003 meta-analysis of 28 studies concluded that there was no association between treatment latency and lithium response [Reference Bratti, Baldessarini and Baethge127], a finding echoed by a 2007 European study that noted treatment delay had little association with subsequent morbidity during mood stabilizer maintenance therapy [Reference Baldessarini, Tondo and Baethge126]. A 2014 Danish analysis came to a different conclusion by examining psychiatric rehospitalization rates in a group of lithium treated BD-1 patients who, following a 6-month lithium stabilization period, continued on lithium as monotherapy [Reference Kessing, Vradi and Andersen128]. Patients who started on lithium earlier (e.g. at the time of their first manic/mixed episode or psychiatric contact with BD-1 diagnosis) had lower rates of psychiatric rehospitalization during follow-up; however, generalizing this finding is difficult as BD-1 is not often treated with monotherapy, and clinicians have no a priori method of deciding who will be an excellent lithium monotherapy responder even with patients whose clinical features suggest greater likelihood of lithium response [Reference Kessing, Vradi and Andersen128].
E Unipolar MDD
What to Know: Adjunctive Lithium for Unipolar MDD
The accumulated data indicate that lithium is an effective adjunctive option for inadequate responders to antidepressant therapy, with comparable response when added to tricyclic antidepressants or selective serotonin reuptake inhibitors.
There are methodological concerns about older studies in this area, so the place of adjunctive lithium in the treatment algorithm of unipolar MDD, and the characteristics of preferential lithium responders, remains to be elucidated.
The RCT literature is sufficient to cement lithium’s reputation for efficacy in acute mania and for BD prophylaxis, but there are areas where the presence of multiple RCTs has not eliminated controversy, and this is true for discussions about lithium’s place in the unipolar MDD treatment algorithm [Reference Undurraga, Sim and Tondo49]. A 2019 review of 12 controlled trials found that adjunctive lithium was superior to placebo for acute unipolar MDD when the data were pooled, but only 4 of the 12 individual studies were positive, the last of which was published in 1996 [Reference Undurraga, Sim and Tondo49]. One concern is that the antidepressant was not optimized in many of the older studies prior to consideration of an adjunctive strategy with lithium [Reference Vázquez, Bahji and Undurraga51]. Moreover, only two of the studies included more than 50 subjects, with the largest trial, a 2003 multicenter study that randomized 149 patients, finding no benefit at the week 6 endpoint for adjunctive lithium over placebo when added to clomipramine nonresponders [Reference Januel, Poirier and D’Alche-Biree129]. Certain authors have postulated that lithium might appear more useful when added to less potent serotonin reuptake inhibitors (e.g. tricyclic antidepressants [TCAs]) based on the idea that lithium’s potentiation of serotonergic neurotransmission might be less effective when added to a selective serotonin reuptake inhibitor (SSRI) [Reference Chenu and Bourin130]; however, the clinical trials data do not support this contention, as comparable response is seen in TCA and SSRI trials [Reference Nelson, Baumann and Delucchi131]. Although SGA augmentation is widespread due to perceived convenience, efficacy and safety advantages over lithium, a large 2020 propensity score matched study of 39,582 US adult unipolar MDD patients (mean age 44.5 years) who initiated augmentation with an SGA (n = 22,410; quetiapine 40%, risperidone 21%, aripiprazole 17%, olanzapine 16%) or with a second antidepressant (n = 17,172) noted increased mortality risk from SGA augmentation [Reference Gerhard, Stroup and Correll132]. In this context, a 2021 review commented that adjunctive lithium was effective and might be better tolerated than SGA augmentation due to lithium’s lack of D2 related adverse effects (e.g. akathisia, parkinsonism), its limited effects on weight, and absence of any impact on serum glucose or lipid levels. Despite the paucity of recent RCTs, the authors implied that lithium is a relevant part of the unipolar MDD treatment algorithm [Reference Vázquez, Bahji and Undurraga51]. Where lithium should fall within the current MDD treatment paradigm, and whether lithium’s benefits accrue primarily to certain patients with mixed features or other BD characteristics, are important questions that hopefully will be addressed in future studies [Reference Undurraga, Sim and Tondo49]. For the present, one must consider lithium as one of many viable adjunctive options for unipolar MDD therapy.
F Suicidality
What to Know: Lithium and Suicidality
The retrospective literature strongly supports that lithium use reduces rates of completed suicide and serious suicidal acts, but that this effect might accrue slowly and require exposures > 16 months to be evident.
Retrospective studies consistently demonstrate lithium’s superiority to valproic acid or SGAs on rates of completed suicide and serious suicidal acts. In certain analyses, valproic acid has no effect on suicidal behavior.
The low rates of completed suicides or serious suicidal acts has limited the ability to document lithium’s effects on these outcomes in prospective randomized clinical trials. Conclusions about lithium’s unique effects on these outcomes rest on the extensive retrospective literature.
January 2022 saw publication of results from a multicenter trial conducted at 29 US Veterans Affairs (VA) hospitals with the goal of determining whether lithium augmentation of usual care for BD or unipolar MDD reduces rates of suicide related events in patients who survived a recent event [Reference Katz, Rogers and Lew40]. The primary outcome was time to any suicide related event, defined as a suicide attempt, interrupted attempt, hospitalization specifically to prevent suicide, or death from suicide. Among the exclusion criteria were a diagnosis of schizophrenia, use of lithium within the prior 6 months, a history of lithium intolerance or ≥ 6 previous lifetime suicide attempts. The last criterion was chosen based on VA analyses showing that reattempts plateaued at 25% to 30% for those with ≥ 6 attempts, but none died from suicide within the next 2 years, so any association between suicidal behavior and risk of suicide death was attenuated in those individuals and this might blunt lithium’s efficacy signal [Reference Katz, Rogers and Lew40, Reference Katz, Ferguson and Liang133]. Participants were randomized in a double-blind manner to receive extended-release lithium carbonate beginning at 600 mg/d or placebo, with a target level between 0.60 and 0.80 mEq/l. Placebo lithium levels were reported in that arm. If participants could not tolerate a dose needed to achieve the target level, they took their maximum tolerated dose, but that dose had to be at least 300 mg/d. The subjects were predominantly male (84.2%), mean age 42.8 ± 12.4 years, and 84.6% had unipolar MDD, 15.4% were diagnosed with BD, and the subject pool had high rates of posttraumatic stress disorder (59.7%), alcohol use disorders (48.4%) and other substance use disorders (36.4%) [Reference Katz, Rogers and Lew40]. The important finding was that the trial was stopped for futility after 519 subjects were randomized due to the absence of significant between-group differences in repeated suicide related events (HR 1.10; 95% CI, 0.77–1.55). Mean treatment exposure was 6.7 ± 4.5 months for unipolar MDD subjects, 5.6 ± 4.6 months for the BD cohort, and mean lithium levels at 3 months were 0.46 ± 0.30 mEq/l for unipolar MDD patients and 0.54 ± 0.25 mEq/l for BD patients [Reference Katz, Rogers and Lew40].
In-Depth 1.15 Discussion about the 2022 US VA Lithium Augmentation Trial for Suicidality
Following publication of the results, correspondence in the journal commented on certain aspects of the study, including: the fact that most of the subjects had unipolar MDD and lithium’s anti-suicide effects may devolve more to BD patients; that mean treatment exposure was relatively brief (38.4 weeks) with only 56% of lithium treated subjects and 47% of placebo treated subjects retained for 1 year; and that there was evidence of functional unblinding as 68% of those on lithium correctly guessed their treatment assignment [Reference Baldessarini and Tondo36]. Moreover, the high rates of psychiatric comorbidity, and use of other medication or psychosocial treatments (which were not specified in the paper) might limit the chances of detecting any lithium effects on the outcome measures. In the end, while the goal of many RCTs is to examine the risk of completed suicide or serious attempts, the low frequency of suicide attempts and suicides even in large trials forces investigators to employ surrogate markers of risk (e.g. the need to intervene to avoid suicide, any self-injury), based on the assumption that they are comparable indicators of risk for completed suicide [Reference Baldessarini and Tondo36]. Unfortunately, that assumption, while reasonable, is “largely untested” according to one commentary, and this highlights a fundamental problem for this area of research: documenting that lithium decreases rates of completed suicide or serious suicide attempts might be impossible in the context of any RCT, as the sample sizes required and duration are beyond what is feasible [Reference Katz, Ferguson and Liang133]. Clinicians must, therefore, make treatment decisions based on the large body of retrospective data, while simultaneously acknowledging the limitations of this literature and the lack of comparable evidence of any type of suicide risk reduction for non-lithium therapies [Reference Baldessarini, Tondo and Davis41].
Lithium’s effect on suicidal behavior had been known for decades through case series, clinical trials of variable quality, and numerous studies reporting an association between higher lithium levels in drinking water and decreased regional suicide rates [Reference Baldessarini, Tondo and Davis41, Reference Tondo, Hennen and Baldessarini134–Reference Liaugaudaite, Raskauskiene and Naginiene139]. Despite this wealth of data, the extent of any risk reduction effect was not well quantified until the publication of two review papers in 2001 and 2006 by Professor Ross Baldessarini, a psychopharmacologist associated for decades with Harvard Medical School and McLean Hospital (Belmont, Massachusetts). As discussed in Info Box 1.1, the 2006 update covered 85,229 person-years of risk exposure from 31 papers providing data on attempted and completed suicides, after excluding 14 other studies that reported zero events in both the lithium and non-lithium arms [Reference Baldessarini, Tondo and Davis41]. The important finding was that the risk reduction appeared consistent across diagnostic categories with 5-fold higher risk in the non-lithium groups, and the effect of lithium was somewhat greater in BD patients compared with those with other major affective disorders. As noted in Table 1.7, the differential impact of BD diagnosis was seen for the primary outcome of attempted and completed suicide. A secondary analysis also examined the ratio of attempts to completed suicides, with higher values indicating reduced lethality of suicidal acts. Using this ratio, lethality decreased during lithium treatment by 2.5-fold across all studies, but the reduction was 2.9-fold when examined for BD patients specifically [Reference Baldessarini, Tondo and Davis41]. While the potential greater effect of lithium in those with a BD diagnosis was noted as one issue in the large VA study, another finding in the 2006 meta-analysis was that studies of shorter duration with mean length 1.41 years (primarily RCTs) saw lesser effects from lithium than those of longer duration (mean 7.77 years). From this finding, one might hypothesize that the anti-suicide impact of lithium might not be instantaneous, but one which accrues over months and years of exposure. This might partially explain the negative result in the VA study where mean treatment exposure was 38.4 weeks, compared with 18 months in the 2006 meta-analysis; however, if this is a biological reality, it might be impossible to test within the confines of an RCT as enormous sample sizes would be needed to retain sufficient numbers for an extended length of time. The 2006 meta-analysis contains limitations, particularly the absence of propensity score matching to balance out clinical features (e.g. history of prior suicide attempts as measured by emergency room visits or psychiatric hospitalizations) that influence real world prescribing practices. Nonetheless, the data indicate lithium has effects on risk for completed suicides, and attempts, not seen with non-lithium therapies.
Info Box 1.1 The Impact of Lithium Therapy on Risk of Suicidal Acts, Attempted and Completed Suicide from a Meta-analysis of 31 Studies Comprising 85,229 Person-Years of Risk Exposure [41]
a. Issue: There was recognition that lithium might reduce the risk of completed suicides, but the extent was not well quantified in the literature prior to 2000. To address this, a large meta-analysis was published in 2001 and then updated in 2006 to cover all trials published through August 2005 [Reference Baldessarini, Tondo and Davis41]. The 2006 paper also performed analyses not previously explored, including the impact of lithium on attempted vs. completed suicide; the differential effects of lithium on BD vs. other major affective disorders; the impact of open clinical studies vs. RCT study design; and outcomes in studies with higher vs. lower quality ratings. Study quality was based on four factors: (1) the presence of subjects observed both with and without lithium treatment (1 point); (2) randomized treatment assignment and blind clinical assessments (1 or 2 points); (3) n ≥ 100 subjects per treatment arm (1 or 2 points); and (4) duration ≥ 1 year per treatment arm (1 or 2 points).
b. Method: For inclusion in the meta-analysis, the source papers must have provided data on attempted and completed suicides. From an initial pool of 45 studies, 14 were excluded from the final statistical calculations as being noninformative since they recorded zero events in both the lithium and non-lithium treatment arms [Reference Baldessarini, Tondo and Davis41].
c. Results: 31 papers comprising 85,229 person-years of risk exposure were analyzed. Subjects received lithium treatment on average for 18 months.
d. Comments: All of the RCTs had zero events in the lithium arm and were of much shorter duration than the open-label studies. Exposure times in studies rated as having higher quality (including RCTs) were 5.5 times shorter than in open-label clinical studies (1.41 ± 1.09 years vs. 7.77 ± 6.54 years).
e. Conclusions: Overall, there is significant consistency among the increased RR values for suicide attempts or completed suicides in non-lithium vs. lithium treated conditions across a variety of affective disorders, bearing in mind that real world prescribing patterns might result in preferential assignment of lithium treatment to those at highest risk, and thus potentially inflate RR estimates for non-lithium arms. The lower RR among higher-quality studies (RR 3.92) might be the product of removing biases in lower-quality studies. The lower RR in RCTs may also relate to the significantly shorter exposure duration compared with open-label studies, and possibly the impact of greater clinical scrutiny during RCTs than in routine clinical care (e.g. more frequent study visits and contact with study personnel) that might alter risk for all treatment arms.
Table 1.7 The risk ratio (RR) of suicide related outcomes in non-lithium vs. lithium conditions
| Studies (n) | Risk ratio | RR 95% CI | p | |
|---|---|---|---|---|
| 1. All two-armed studies | 31 | 4.91 | 3.82–6.31 | < 0.0001 |
| 2. Omitting Goodwin et al. (2003)Footnote a | 30 | 5.34 | 4.27–6.68 | < 0.0001 |
| 3. Open clinical studies | 26 | 3.41 | 2.61–4.46 | < 0.0001 |
| 4. Randomized controlled trials | 5 | 1.76 | 1.65–1.88 | 0.001 |
| 5. Suicides only | 24 | 4.86 | 3.36–7.02 | < 0.0001 |
| 6. Attempts only | 17 | 4.98 | 3.56–6.96 | < 0.0001 |
| 7. Bipolar disorder | 14 | 5.34 | 3.59–7.93 | < 0.0001 |
| 17 | 4.66 | 3.43–6.33 | < 0.0001 |
| 9. Quality score ≥ 50% | 16 | 3.92 | 2.94–5.23 | < 0.0001 |
| 10. Quality score < 50% | 15 | 5.56 | 3.98–7.76 | < 0.0001 |
a Results after the data from Goodwin et al. (2003) were omitted indicated that this very large study did not exert a misleading influence on the overall findings.
As certain questions about lithium may be unanswerable by an RCT, subsequent investigators employed other analytic methods to examine its effects on suicidal behavior. As discussed in the section on maintenance treatment, a British group performed a propensity score matched, population based cohort study using electronic health records for 5089 UK BD patients prescribed lithium (n = 1505), VPA (n = 1173), olanzapine (n = 1366) or quetiapine (n = 1075) with an initial goal of examining the differential rates of treatment failure [Reference Hayes, Marston and Walters115]. In a follow-up to that paper, the investigators performed a secondary analysis of this data set to examine lithium’s comparative effects on self-harm, with the primary outcome defined as any emergency room or primary care visit for self-harm during the period of drug exposure and up to 3 months afterward [Reference Hayes, Pitman and Marston140]. The propensity score methods, subject exclusions and definitions of drug treatment periods were identical to the prior study. After propensity score adjustment and matching, the hazard ratio (HR) for the primary outcome of self-harm among the three non-lithium therapies combined (VPA, olanzapine, quetiapine) vs. lithium was 1.51 (95% CI 1.21–1.88) (Figure 1.5). The specific comparison between VPA and lithium yielded a slightly lower value (HR 1.31, 95% CI 1.01–1.70), although this result was also statistically significant [Reference Hayes, Pitman and Marston140]. The authors performed another analysis for the outcome of unintentional injury, and, after propensity score adjustment and matching, the HR for the three non-lithium therapies combined (VPA, olanzapine, quetiapine) vs. lithium was again significant (HR 1.19, 95% CI 1.01–1.41), as was the specific comparison between VPA and lithium (HR 1.34, 95% CI 1.09–1.65). Although this analysis might have captured behavior that was parasuicidal without suicidal intent, the use of propensity score matching mitigates some of the prescribing bias and supports the conclusions of lithium’s superior impact on dimensions of suicidal behavior [Reference Hayes, Pitman and Marston140].

Figure 1.5 Cumulative self-harm rate among British BD patients aged ≥ 16 years prescribed monotherapy with lithium or non-lithium therapies (valproate, olanzapine or quetiapine) [140]
Another approach to exploring lithium’s relative effects vs. other treatments was employed in a within-individual 8-year study of suicidal behavior in BD patients on lithium or VPA treatment [Reference Song, Sjolander and Joas141]. This study used the Swedish national registry of 51,535 BD patients followed from 2005 to 2013 receiving treatment with lithium or VPA to estimate the HR of suicide related events during treated periods compared with untreated periods [Reference Song, Sjolander and Joas141]. In this large data set, there were 10,403 suicide related events that occurred in 4405 individuals [Reference Song, Sjolander and Joas141]. The rate was significantly decreased by 14% during periods with lithium treatment (HR 0.86, 95% CI 0.78–0.95) but not during VPA exposure (HR 1.02, 95% CI 0.89–1.15), and this HR difference was statistically significant (p = 0.038). None of the sensitivity analyses showed any substantive difference from the main results, and analyses for the combination of lithium and VPA yielded no substantial difference from lithium alone, indicating a lack of benefit on suicidal behavior for VPA. Additionally, patients had an increased rate of suicidal behavior within 30 days of lithium discontinuation (HR 1.33, 95% CI 1.09–1.61) [Reference Song, Sjolander and Joas141]. Another interesting finding was that the majority of suicidal events occurred in those with comorbid substance use (7976 events in 15,927 patients), and lithium use was also associated with reduced events even in this group (HR 0.84, 95% CI 0.75–0.94). The authors concluded that VPA offered no protective effect for suicide related events, and that there was a significant difference between lithium and VPA in the effects on suicidal behavior [Reference Song, Sjolander and Joas141]. The paper also estimated that 12% (95% CI 4%–20%) of suicide related events could have been avoided if patients had taken lithium during the entire follow-up.
In-Depth 1.16 Detailed Methods of Swedish Registry Study on Lithium and Suicidality
Suicidal behavior was defined as attempted or completed suicide by specific diagnostic codes (ICD-10: X60–X84, Y10–Y34) that potentially included events with undetermined intent. A medication period was defined as a sequence of at least two prescriptions, with no more than 3 months (92 days) between any two consecutive prescriptions. Sensitivity analyses examined a number of parameters that might influence the outcome (the impact of year of diagnosis, use of concomitant medications, varying definitions of bipolar disorder, mixed vs. nonmixed episodes, starting lithium within 1 year of the initial BD diagnosis, varying definitions of suicidal events), but specifically addressed two crucial issues: bias in starting lithium due to recent suicidality, and whether monotherapy of either mood stabilizer was superior to the combination of lithium and VPA [Reference Song, Sjolander and Joas141]. To test whether lithium use was biased toward those with a recent suicide history, the main analysis was repeated excluding periods containing a switch to lithium within 7, 14 or 30 days after a suicide attempt. To test the relative effects of mood stabilizer monotherapy or combinations, the main analysis was repeated by defining medication periods with lithium alone, VPA alone, and lithium plus VPA. As patients on lithium monotherapy might be different from patients who have switched between lithium and VPA, the analysis was repeated for the subgroup on lithium monotherapy [Reference Song, Sjolander and Joas141].
All retrospective studies have limitations, and even the attempt to remove biases toward lithium use in the Swedish registry study might have been insufficient as clinicians might be influenced by suicidal events that occurred more than 30 days in the past, especially with a pattern of suicidal behavior or a serious past event. Nonetheless, this paper adds to other literature in this area pointing to an effect of lithium on risk of attempted or completed suicide, an effect not seen to the same extent with other mood stabilizers such as VPA. As discussed in Info Box 1.2, clinicians must be aware that these conclusions are based on retrospective analyses; however, in the absence of convincing data on suicidality reduction for any other medication used in BD, lithium remains unique among the options available to manage BD spectrum patients at risk for completed suicide, and possibly in those with unipolar MDD.
Info Box 1.2 Issues in Weighing Lithium’s Anti-Suicide Effects
a. What have we learned from retrospective analyses? Bearing in mind the prescribing bias toward preferential use of lithium in patients with prior suicidal behavior [Reference Katz, Ferguson and Liang133], studies consistently find lower risk of completed suicides and suicide attempts among lithium users, without comparable effects for non-lithium therapies [Reference Baldessarini, Tondo and Davis41, Reference Hayes, Pitman and Marston140, Reference Song, Sjolander and Joas141]. These effects from lithium may be greater among BD spectrum patients than in those with other disorders (e.g. unipolar MDD) [Reference Baldessarini, Tondo and Davis41]. As more retrospective studies employ propensity score matching to eliminate as much as possible prescribing biases, future analyses will hopefully yield more refined estimates of lithium’s anti-suicide effects relative to other medications in real world usage [Reference Katz, Ferguson and Liang133].
b. Limitations of the retrospective data: There is no compelling evidence that lithium directly impacts suicidal ideation, with modest data to suggest an impact on all acts of self-harm and unintentional injury in BD spectrum patients [Reference Hayes, Pitman and Marston140]. The minimum duration necessary to achieve lithium’s anti-suicidal effects is unknown, but 18 months or more of exposure may be required based on the smaller effect size seen in patients with shorter vs. longer periods of use in one large meta-analysis (1.41 ± 1.09 years vs. 7.77 ± 6.54 years) [Reference Baldessarini, Tondo and Davis41]. Clinicians should not assume the effect is instantaneous upon starting lithium.
c. Randomized clinical trials (RCTs): While evidence from RCTs is the gold standard for proving an efficacy claim, the infrequency of suicide attempts and completed suicides in prospective clinical trials has led to negative results when examining those outcomes. For this reason, most studies are forced to include additional surrogate measures of suicidal behavior (e.g. need for intervention to prevent suicide or self-harm), but those outcomes may not be comparable indicators of suicide risk [Reference Baldessarini and Tondo36]. Due to the low rates of suicide deaths or serious attempts, enormous sample sizes and an extended duration of follow-up would be necessary to study those particular outcomes in an RCT, and that presents an economic and feasibility barrier to such studies [Reference Katz, Ferguson and Liang133].
d. Conclusions: It might not be possible within the context of an RCT to prove that lithium reduces risk of suicide attempts and completed suicides, so clinicians must acknowledge the limitations of the data, but also the absence of robust data for any non-lithium therapy. Lithium should not be viewed as a panacea for all parasuicidal and suicidal behavior, but as a tool with significant value over the lifetime of a patient, especially those individuals with BD spectrum diagnoses who have a history of suicidality.
G Neuroprotection
What to Know: Lithium and Neuroprotection
Bipolar spectrum patients have 3-fold higher risk for dementia. Lifestyle factors (e.g. smoking), cardiovascular comorbidity and mood relapses, especially episodes of mania and hypomania, all contribute to dementia risk.
Use of lithium for at least 10 months in older bipolar patients reduces dementia risk by 23%, and longer-term use decreases this risk by 49%. There is no impact of non-lithium therapies on dementia risk.
The neuroprotective properties of lithium were also evident in a 24-month trial of individuals without bipolar disorder who were diagnosed with mild cognitive impairment.
Lithium’s multiple neuroprotective mechanisms relate to decreases in intracellular inositol triphosphate (IP3) levels, inhibition of GSK3-β activity, and mitigation of telomere shortening.
1 Clinical and Preclinical Evidence for Lithium’s Neuroprotective Properties
Lithium’s neuroprotective properties have been studied for decades, with preclinical studies appearing more abundantly in the late 1990s that documented lithium’s ability to limit the effects of ischemia, and to reduce apoptosis and excitotoxic cellular damage from a variety of toxic insults [Reference Calabresi, Pisani and Mercuri142–Reference Nonaka, Katsube and Chuang145]. Animal stroke models proved especially useful for exploring the range of lithium’s neuroprotective effects, as ischemic and hemorrhagic strokes present different forms of cellular injury and patterns of recovery [Reference Almeida, Singulani and Ford146]. In these studies, the neuroprotective effects of lithium were seen in the form of reduced infarct volume, reduced postischemic excitotoxicity, improved poststroke recovery, antiapoptotic effects, decreased expression of inflammatory markers, reduced oxidative stress, and activation of immune mediated responses involved in the restoration of blood–brain barrier integrity [Reference Almeida, Singulani and Ford146]. This array of early animal data on lithium’s ability to reduce cellular injury from acute insults (e.g. ischemic, toxic) stimulated interest in lithium’s long-term effects on neurodegenerative disorders, especially in transgenic mouse models of Alzheimer’s disease [Reference Nunes, Schowe and Monteiro-Silva147, Reference Morris and Berk148]. Preclinical animal findings are not always mirrored by human clinical outcomes, and, despite robust data from stroke models, the human data remain inconclusive regarding lithium’s ability to limit damage or facilitate recovery following stroke [Reference Almeida, Singulani and Ford146, Reference Haupt, Bahr and Doeppner149]. The opposite is true for lithium’s impact on cognitive decline and dementia risk, with both retrospective and prospective studies illustrating this effect in patients with BD, and in those without mood disorders experiencing mild cognitive impairment (MCI) [Reference Velosa, Delgado and Finger44, Reference Forlenza, Radanovic and Talib48, Reference Rybakowski150–Reference Chen, Underwood and Jones154]. The majority of these data come from BD spectrum patients, but the estimated reduction in dementia incidence of 40%–50% across multiple studies presents one of the most convincing reasons for clinicians to master the use of lithium in older BD-1 patients (see Chapter 4), and to appreciate that the medical burden of lithium use in older BD-1 patients is not significantly different than for VPA (see Chapter 7) [Reference Rej, Yu and Shulman155].
The other rationale for preferentially using lithium in older BD patients relates to the significantly higher dementia risk in this population, with mood relapses and disproportionate rates of smoking and cardiometabolic disorders contributing to this inflated figure [Reference Velosa, Delgado and Finger44]. A 2020 meta-analysis provided an estimate of dementia risk in BD patients by analyzing the odds of dementia vs. demographically matched controls in 10 studies that had adequate data for meta-analysis: 4 cohort studies (range of follow-up 3–17 years), and 6 studies with case-control designs. The total sample sizes were 6859 for the BD subjects and 487,966 for the controls. All but one of the studies indicated that a BD diagnosis increased dementia risk, and the pooled odds ratio indicated that this risk is 3-fold greater in BD patients compared with controls (OR 2.96, 95% CI 2.09–4.18, p < 0.001) [Reference Velosa, Delgado and Finger44]. There were two other findings of note: (1) The number of mood episodes in BD patients predicted dementia risk, with some studies suggesting that the risk was more attributable to periods of hypomania/mania than periods of depression [Reference Velosa, Delgado and Finger44]; (2) Dementia risk was greater for BD than for unipolar MDD patients based on a subset of studies that included both diagnostic groups, a finding consistent with data indicating a somewhat lower 1.65- to 2-fold increased risk for unipolar MDD [Reference Velosa, Delgado and Finger44].
In-Depth 1.17 The Impact of Manic and Hypomanic Episodes on Cognitive Decline
A 2020 publication provided confirmatory data on the effect of hypomania/mania based on results of a prospective structural magnetic resonance imaging (MRI) study in BD patients and healthy control (HC) subjects. 206 subjects underwent imaging at baseline (123 BD, 83 HC) and 151 were available for repeat imaging 6 years later (90 BD patients, 61 HC) [Reference Abé, Liberg and Song156]. Over the 6 years of follow-up, BD patients showed abnormal cortical thinning of temporal cortices; moreover, those who experienced hypomanic or manic episodes showed abnormal thinning in inferior frontal cortices. Cortical changes did not differ between BD-1 and BD-2 subtypes – the effect was related to periods of hypomania or mania [Reference Abé, Liberg and Song156]. A 2021 study reinforced the differential effects of depression and hypomania/mania on brain function by combining demographic and illness history with results of a 13-part neuropsychological battery performed in 172 BD patients of mean age 66.0 years residing in Amsterdam, 56.4% with BD-1, and 43.6% BD-2 [Reference Beunders, Kemp and Korten157]. After controlling for age and education level, the final multivariable model explained 43.0% of the variance in composite cognitive score [Reference Beunders, Kemp and Korten157]. Two variables predicted relatively better cognitive performance, number of depressive episodes and onset at age ≥ 50 years, while five or more psychiatric admissions and use of benzodiazepines were associated with worse cognitive performance [Reference Beunders, Kemp and Korten157]. As BD-1 patients are disproportionately admitted for mania, this is another analysis demonstrating the cumulative deleterious effects of mania on cognition. It is worth noting that the association with the number of hypomanic/manic episodes fell just short of statistical significance (p = 0.065). Treatment related information was based on patient interview, so one hypothesis is that the number of prior psychiatric admissions is likely to be recalled more accurately in patients who are 66 years old than number of lifetime mood episodes.
In-Depth 1.18 Brain Age Gap in Bipolar Disorder vs. Unipolar Major Depression
The impact of hypomania or mania for the brain health of BD patients can also be explored by looking at brain aging in BD patients compared to those with unipolar MDD. In 2022, a meta-analysis was published comprising 18 studies which used neuroimaging data to calculate the brain age gap between psychiatric patients and age-matched controls [Reference Ballester, Romano and de Azevedo Cardoso158]. As the three diagnostic groups consisted of patients diagnosed with schizophrenia, BD or unipolar MDD, one can compare the relative illness effects of these disorders on brain aging [Reference Ballester, Romano and de Azevedo Cardoso158]. The random-effects model found a significantly increased neuroimaging-derived brain age gap relative to age-matched controls for all three cohorts, with schizophrenia having the largest gap (Δ 3.08 years; 95% CI 2.32–3.85 years; p < 0.01), followed by BD (Δ 1.93 years, 95% CI 0.53–3.34 years; p < 0.01) and then by unipolar MDD (Δ 1.12 years, 95% CI 0.41–1.83 years; p < 0.01) [Reference Ballester, Romano and de Azevedo Cardoso158]. The clinical manifestation of accelerated brain aging found on imaging is also readily seen in neuropsychological performance. A cross-sectional trial compared the results of 113 BD-1 patients and 64 healthy adults aged 18–87 on measures of processing speed, attention, executive functioning and verbal fluency to explore the interrelationships of age, clinical variables and cognitive functioning [Reference Lewandowski, Sperry and Malloy159]. In the linear regression models, BD-1 patients performed significantly worse than the comparison group on all neuropsychological measures [Reference Lewandowski, Sperry and Malloy159]. Older age was also associated with poorer performance on Trails A in BD-1 patients but not in the healthy adults, further evidence of brain aging associated with the BD-1 diagnosis. It is important to appreciate that the effects of mood relapses on brain function, especially hypomania or mania, accrue over long periods of time. In minimally symptomatic stable BD outpatients, mood state at the time of neuropsychological testing and cognitive performance are generally unrelated, implying that any cognitive dysfunction seen at the time of testing is the product of longitudinal effects associated with the mood disorder [Reference Easter, Ryan and Estabrook160]. This was confirmed by results of a large study of community dwelling BD adults (n = 773) with mean age 39.57 ± 13.61 years and a mean of 15.22 ± 2.19 years of education, whose baseline scores on the HAM-D and YMRS indicated full remission of mania and mild (subthreshold) depressive symptoms [Reference Easter, Ryan and Estabrook160]. When the investigators compared neuropsychological battery results and mood assessments at baseline and after 1 year of follow-up, they found that baseline cognition significantly predicted cognitive ability after 1 year, with almost no influence from mood symptoms [Reference Easter, Ryan and Estabrook160]. The authors concluded that any cognitive dysfunction seen in stable outpatients is not due to subtle mood symptoms at that time, but is either a trait effect of the BD diagnosis itself or a consequence of the disorder.
Multiple studies have examined lithium’s cognitive effects in BD patients, but the 2020 meta-analysis that estimated BD dementia risk provided the most accurate assessment of this effect [Reference Velosa, Delgado and Finger44]. Five cohort studies and one case-control design were found that looked at the correlation between lithium exposure and dementia risk, but one of the cohort studies provided insufficient data for the meta-analysis. Most of the papers were rated as having good-quality designs using the Newcastle–Ottawa Quality Assessment Scale, and four of the five analyzable studies showed a preventative effect of lithium exposure on dementia risk. Overall, there were 6483 BD spectrum patients and 43,396 control individuals in the final analysis. As seen in Figure 1.6, lithium use in BD patients significantly and robustly reduced dementia risk by almost 50% (OR 0.51, 95% CI 0.36–0.72, p < 0.0001) [Reference Velosa, Delgado and Finger44].

Figure 1.6 Results from a 2020 meta-analysis of 6483 lithium treated bipolar disorder patients noting a 49% reduction in the risk of dementia [44]
A cohort study appeared in the literature shortly after the 2020 meta-analysis was published providing further evidence for the robust association between lithium use and reduced dementia risk. The investigators used electronic clinical records of secondary care mental health services from the Cambridgeshire and Peterborough UK NHS Foundation to identify 548 lithium treated patients and 29,070 individuals not receiving lithium, mean age 73.9 years [Reference Chen, Underwood and Jones154]. After controlling for sociodemographic factors, medications, other psychiatric and somatic comorbidities and smoking status, lithium use was associated with a 44% lower risk of any dementia diagnosis (HR 0.56, 95% CI 0.40–0.78, p = 0.0006), a 45% reduction for dementia of the Alzheimer type (HR 0.55, 95% CI 0.37–0.82), and a 64% reduction for vascular dementia (HR 0.36, 95% CI 0.1– 0.69) (Figure 1.7) [Reference Chen, Underwood and Jones154]. In addition to finding that lithium reduces risk for the two most common forms of dementia, the UK analysis also noted that lithium’s protective effect was seen within 1 year of exposure [Reference Chen, Underwood and Jones154].

Figure 1.7 Cumulative risk of dementia in lithium users (n = 548) vs. non-users (29,070) (mean 73.9 years) with at least 1 year of mental health follow-up during 2005–2019 at the Cambridgeshire and Peterborough NHS Foundation Trust [154]
In-Depth 1.19 Lithium, but Not Anticonvulsant Mood Stabilizers, Reduces Dementia Risk: Evidence
The results of a large US cohort study that examined future dementia risk by duration of lithium use (0, 1–60, 61–300 and 301–365 days) in 6900 lithium treated BD patients age ≥ 50 years without a dementia diagnosis not only confirmed lithium’s protective effect, but the absence of such effects from other mood stabilizers used as a control arm [Reference Gerhard, Devanand and Huang161]. The data set employed for this analysis was a Medicaid extract for the years 2001–2004 from eight large US states, with anticonvulsants commonly used as mood stabilizers serving as the negative control (n = 20,778), and the results of both medication cohorts compared with the dementia incidence among 18,119 BD patients not on lithium or an anticonvulsant [Reference Gerhard, Devanand and Huang161]. In this sample of mean age 60.4 years, 301–365 days of lithium exposure was associated with significantly reduced dementia risk (HR = 0.77, 95% CI 0.60–0.99) when compared with non-use of lithium. No corresponding association was observed for shorter lithium exposures (HR = 1.04, 95% CI 0.83–1.31 for 61–300 days; HR = 1.07, 95% CI 0.67–1.71 for 1–60 days) or for any exposure to anticonvulsants [Reference Gerhard, Devanand and Huang161]. That as little as 10 months of lithium exposure can reduce dementia incidence in older BD patients by 23%, and that prolonged use reduces this risk by as much as 50%, places the onus on every clinician to justify withholding or discontinuing lithium in older BD patients who can comply with the necessary monitoring frequency based on their eGFR and CKD risk factors (Chapter 4). As reviewed in detail in Chapter 7, it is the unmonitored addition of a kinetically interacting medication that presents the greatest risk for lithium toxicity in older patients, not age itself [Reference Juurlink, Mamdani and Kopp162, Reference Heath, Billups and Gaughan163]. Moreover, it is CKD risk factors which have the more significant impact on eGFR trends in older adults, not lithium itself when it is prescribed according to modern dosing precepts and patients are not subjected to periods of lithium toxicity [Reference Clos, Rauchhaus and Severn119, Reference Golic, Aiff and Attman164].
There are other sources that support these findings, including one study of dementia incidence based on drinking water lithium levels [Reference Kessing, Gerds and Knudsen151], and numerous cross-sectional studies noting superior cognitive performance in BD patients on lithium vs. lithium non-users [Reference Rybakowski150, Reference Wingo, Wingo and Harvey165–Reference Forlenza, Hajek and Almeida168]. As BD patients have 3-fold higher dementia risk than age-matched peers due to the combined effects of hypomania/mania and medical comorbidities, an intriguing question is to what extent lithium’s neuroprotective effect might be seen in non-BD patients. The preclinical data from Alzheimer’s disease models were considered compelling enough to pursue a prospective trial in 61 community-dwelling, healthy older adults with MCI (mean age 72.6 ± 4.8 years), randomized in a double-blind manner to lithium or placebo for 2 years, with an additional 24 months of single-blinded follow-up [Reference Forlenza, Radanovic and Talib48]. The target lithium level range was 0.25–0.50 mEq/l. Over the initial 24 months of the study, subjects in the placebo arm displayed cognitive and functional decline, while the lithium treated patients remained stable. Five subjects in the lithium group (16%) and nine in the placebo group (30%) converted from MCI to dementia during follow-up, but this fell just short of statistical significance for this difference (p = 0.06). Not only was lithium exposure associated with better performance on memory and attention tests after 24 months, there was also a significant increase in cerebrospinal fluid (CSF) amyloid-β peptide (Aβ1–42) levels after 36 months among those with higher intracerebral Aβ1–42 burden at baseline. The Aβ1–42 fragment is the main component of amyloid plaques found in the brains of people with Alzheimer’s disease, and these aggregates incite inflammatory changes that contribute to cellular damage and death. The finding of higher CSF Aβ1–42 levels suggests that long-term lithium treatment promotes cerebral clearance of Aβ1–42 [Reference Forlenza, Radanovic and Talib48]. While lithium has long been touted as a possible agent for patients with Alzheimer’s disease [Reference Nunes, Schowe and Monteiro-Silva147–Reference Haupt, Bahr and Doeppner149, Reference Patra169], MCI patients have greater preservation of cognitive function and lower amyloid plaque burden, and thus might be a more suitable target for future lithium trials. Hopefully, other investigators will replicate the results of the 24-month study in larger samples and thus establish lithium as an evidence based option to forestall MCI progression [Reference Haupt, Bahr and Doeppner149].
2 Intracellular Mechanisms that Underlie Lithium’s Neuroprotective Properties
Lithium has numerous and complex interactions with intracellular pathways, each of which may contribute individually or synergistically to its neuroprotective effects (see Figure 1.8) [Reference Puglisi-Allegra, Ruggieri and Fornai170]. Lithium’s neuroprotective properties can thus be viewed on both the micro and macro level given that the effects are seen with in vitro and in vivo models of acute injury, as well as with chronic exposure in human beings with and without BD [Reference Ochoa171]. On the cellular level, lithium increases the production of nerve growth factors, mitigates the effects of inflammation and oxidative stress on mitochondrial function, and modulates autophagy and apoptosis [Reference Ochoa171]. As discussed below, lithium’s mood stabilizing properties are especially ascribed to effects on pathways involving two primary targets: inositol monophosphatase (IMPase) and GSK3-β [Reference Pasquali, Busceti and Fulceri67], with emerging evidence that the neuroprotective mechanisms in BD patients are the epiphenomenon of those same processes that maintain mood stability and limit episodes of hypomania and mania [Reference Ochoa171]. While certain aspects of research on lithium’s neuroprotective properties and potential are still being developed, the clinical findings of reduced dementia risk in BD patients should provide sufficient impetus to consider lithium as the mood stabilizer of choice for older BD patients with a history of mania (e.g. BD-1, SAD-BT).
Legend
1. Inhibition of inositol reuptake
2. Depletion of intracellular inositol triphosphate (IP3)
3. Decreased IP3 levels minimize stimulation of endoplasmic reticulum (ER) calcium (Ca++) release and downstream processes that induce mitochondrial damage
4. Impact on IP3 levels also mitigates impaired stress related apoptosis regulation
5. Direct impact on Ca++ release from ER also lessens stimulation of protein kinase C (PKC) and its promotion of GSK3-β activity
6. Direct inhibition of GSK3-β activity, with the net result being less oxidative stress and less impaired autophagy
7. Direct inhibition of GSK3-β activity also promotes neurotrophic, neuroprotective and antioxidant gene expression

Figure 1.8 Multiple mechanisms that underlie lithium’s neuroprotective effects [170]
In-Depth 1.20 Lithium’s Effects on Telomere Shortening
That lithium delays cognitive decline in non-BD patients with MCI is a convincing argument that some of its neuroprotective properties exist outside of the domain of any mood related impact, and that mood stabilization is the result of these homeostatic effects [Reference Pasquali, Busceti and Fulceri67]. One neuroprotective effect recently identified that may not relate to mood stabilization is the impact of lithium on a marker of cellular aging: the telomere length [Reference Coutts, Palmos and Duarte172]. Telomeres are stretches of TTAGGG nucleotide repeats at the ends of chromosomes, and these telomeric nucleotides protect coding DNA from being lost during replication by allowing portions of the telomeric sequence to be shed each time a cell divides; however, when the telomere shortens beyond a critical length, the cell loses its ability to divide [Reference Coutts, Palmos and Duarte172]. As we age, this process of telomere shortening gradually limits the ability to replace older cells, setting the stage for age-related disease. Multiple studies thus indicate a strong association between genetic determinants of telomere length and the risk for age-related diseases and mortality [Reference Coutts, Palmos and Duarte172]. Since 2013, papers have emerged documenting shorter telomere length in leukocytes of BD patients, although these findings are not seen in all studies [Reference Martinsson, Wei and Xu173, Reference Powell, Dima and Frangou174]. Similarly, there is a parallel literature describing a protective effect of lithium on telomere shortening that appears to correlate with duration of exposure [Reference Squassina, Pisanu and Congiu175, Reference Lundberg, Biernacka and Lavebratt176]. One recent example is a 2019 cross-sectional analysis of specimens from 384 BD patients which found that chronic lithium treatment was associated with longer telomeres compared with lithium non-users (p = 0.03) [Reference Coutts, Palmos and Duarte172]. Moreover, polygenic risk scores associated with telomere length explained more of the variance in telomere length in lithium users compared with non-users, suggesting that lithium is promoting certain endogenous mechanisms that support telomere lengthening up to the genetically determined limit for that individual’s telomere maintenance capacity [Reference Coutts, Palmos and Duarte172]. One hypothesis for this telomere lengthening effect relates to evidence that lithium induces expression of telomere reverse transcriptase (TERT) [Reference Lundberg, Biernacka and Lavebratt176]. Telomere shortening can be counteracted by the activation of telomerase, a complex consisting of telomerase RNA component, an RNA template used for telomere synthesis, and TERT, the catalytic subunit. The function of telomerase is to lengthen telomeres in the nucleus, preserving the integrity of end DNA sequences and promoting cellular repair and cellular survival [Reference Lundberg, Biernacka and Lavebratt176]. Using leukocytes from 100 BD-1 patients and 100 healthy controls, investigators from the Karolinska Institute (Stockholm, Sweden) and the Mayo Clinic (Rochester) found that TERT expression was significantly and positively correlated with duration of lithium treatment in patients treated with lithium for ≥ 24 months; however, they did not find any significant effect of lithium on telomere length, nor did they find a significant difference in telomere length between BD-1 patients and controls [Reference Lundberg, Biernacka and Lavebratt176]. From these data, the authors hypothesized that lithium related increases in TERT expression contribute to both mood stabilizing and neuroprotective properties by improving mitochondrial function and decreasing oxidative stress, but indicated that this is an area that deserves further study.
H Aggressive or Impulsive Behavior in Child/Adolescent Patients with Conduct Disorder, Borderline Personality Disorder (BPD) and Intellectual Disability
What to Know: Impact of Lithium on Aggression and Impulsivity
Most of the literature in this area is of poor quality or consists of single site trials that have not been replicated.
The literature does not strongly support lithium’s efficacy for conduct disorder, or for impulsive-behavioral dyscontrol in borderline personality disorder. There are somewhat more compelling data for management of disruptive behaviors in intellectually disabled individuals, but more effective options exist and should be tried initially.
Any use of lithium to manage aggression or impulsivity in non-bipolar patients should be relegated to the latter stages of any algorithm, with lithium used at modest levels and withdrawn if robust effects are not seen after 1–2 months.
Animal models support the concept that lithium possesses anti-aggression properties [Reference Muller-Oerlinghausen and Lewitzka52], but this is an area where the human data are not compelling enough to justify routine clinical use. Nonetheless, suicide and aggression are conceptualized as having overlapping neurobiological bases, and one hypothesis for lithium’s impact on suicide related mortality rests in its anti-aggression effects [Reference Muller-Oerlinghausen and Lewitzka52]. Supporting this idea are findings from epidemiological studies that correlate higher lithium levels in municipal drinking water supplies with lower regional rates of homicide and other violent crimes [Reference Giotakos53, Reference Schrauzer and Shrestha177–Reference Giotakos, Tsouvelas and Nisianakis179]. Aggression is not a unitary concept, and studies among patients with severe mental disorders recognize three categories of acts: those due to uncontrolled psychosis or mania, those related to impulsivity, and those which are planned and engaged in to achieve an outcome such as intimidation or retribution (i.e. instrumental) [Reference Quanbeck, McDermott and Lam180–Reference Brown, Larkin and Sengupta182]. In those without active psychosis or mania, any anti-aggressive effect of lithium is presumed related to decreased impulsivity, and this has been the basis for exploratory trials across a broad range of populations including some without obvious mental disorders (e.g. prisoners) [Reference Muller-Oerlinghausen and Lewitzka52]. Unfortunately, most of the literature in this area consists of open-label studies and case series, or individual double-blind, placebo-controlled trials that have not been replicated or that possessed methodological limitations. For example, the placebo-controlled literature on use of lithium for conduct disorder in children or adolescents consists of two trials, one of which employed unacceptably high mean lithium levels (1.20 mEq/l), and with no studies published since 2000 [Reference Campbell, Adams and Small183, Reference Malone, Delaney and Luebbert184]. A 2010 Cochrane review of pharmacological interventions for borderline personality disorder noted some beneficial effects with SGAs, mood stabilizers (lithium or divalproex) and dietary supplementation by omega-3 fatty acids, but mostly from single studies. Moreover, overall illness severity was not significantly influenced by any medication, and medications do not address the core borderline personality disorder symptoms of emptiness, identity disturbance and abandonment [Reference Stoffers, Völlm and Rücker185]. In addition to high dropout rates, variable study length, and widely divergent proportions of patients in psychotherapy (0–100%) or with comorbid mood disorders (0–100%), there are no long-term studies in borderline personality disorder, and most studies excluded patients with alcohol and substance use disorders, limiting the ability to generalize any findings to usual clinical practice [Reference Mercer, Douglass and Links186]. A 2011 review did not include lithium among the list of agents proven useful to treat affective symptoms and impulsive-behavioral dyscontrol in borderline personality disorder patients [Reference Bellino, Rinaldi and Bozzatello187], although a 2022 review comments that a mood stabilizer such as lithium or lamotrigine may be beneficial where family history suggests a genetic link to BD [Reference Stone58]. The idea that any benefit of lithium for impulsivity in borderline personality disorder relates to subtle forms of a BD diathesis in certain patients is based on the concept that there are qualitatively different types of affective variability in BD and borderline personality disorder individuals [Reference Pulcu, Saunders and Harmer188]. Patients with BD note more prolonged periods of raised or lowered affect, while those with borderline personality disorder report a higher frequency of transient affective variation. A conceptualization of these differences relates to divergent causes of affective variability: volatility, which leads to persistent changes in affect as seen in BD, and noise, which leads to transient changes as seen in borderline personality disorder. A 2022 prospective study showed that lithium is very effective for improving prolonged affective volatility, but is not generally effective in reducing affective noise for borderline personality disorder patients [Reference Pulcu, Saunders and Harmer188].
While the preclinical and available clinical data suggest some potential to manage conduct disorder and aggression in non-bipolar children or adolescents [Reference Masi, Milone and Manfredi54, Reference Pringsheim, Hirsch and Gardner55], to lessen disruptive behaviors in intellectually disabled individuals, or to curtail impulsivity in borderline personality disorder, lithium’s use should be relegated to the latter stages of any treatment algorithm for several reasons: there are more strongly evidence based treatments for certain clinical scenarios (dialectical behavioral therapy for borderline personality disorder, SGAs for irritability in autistic disorder), there are no long-term studies, and the evidence for lithium is generally uneven and of low quality. There are also safety concerns when high serum lithium levels (e.g. > 1.00 mEq/l) are employed [Reference Campbell, Adams and Small183], especially in patients with intellectual disability [Reference Deb, Chaplin and Sohanpal56, Reference Ji and Findling57, Reference Janowsky, Soares and Hatch189, Reference Janowsky, Buneviciute and Hu190]. Lithium can be used safely in intellectually disabled patients with careful monitoring [Reference Yuan, Song and Zhu191], but clinicians should acknowledge the lack of methodologically strong controlled data for this patient population. Regardless of the application, certain aggressive or impulsive behaviors wax or wane based on dynamic factors [Reference Oliver-Africano, Dickens and Ahmed192], so any change associated with a lithium trial may be spurious. It is the clinician’s responsibility to taper off lithium if the response has not been particularly robust, and to consider a taper after prolonged use where other interventions or factors may have contributed to a reduction in problematic behaviors [Reference Oliver-Africano, Dickens and Ahmed192]; moreover, as the benefits are largely unquantifiable, any clinician who uses lithium for these purposes must transparently communicate to patients and/or caregivers that the effect might be minimal, and employ prescribing and monitoring practices that emphasize patient safety. The use of lithium in these clinical situations is not inherently unreasonable once other options have been exhausted, but management of risk and periodic reassessment of efficacy are important guiding principles where the evidence base is limited.
I Neutrophilia
What to Know: How Lithium Increases Neutrophil Counts
Lithium directly stimulates production of granulocyte colony stimulating factor (G-CSF), and thereby stimulates production of neutrophils. The concept that lithium only causes demargination of neutrophils in bone marrow reserves is incorrect.
All clinicians should be aware that lithium may increase neutrophil counts starting 1–2 weeks after initiation to obviate any unnecessary work-up for occult sources of infection.
Lithium has been used by hematologists to manage neutropenia since the 1970s, and by the psychiatric profession to manage neutropenia prior to or during clozapine therapy for over 30 years.
The association between lithium and neutrophilia has been known for over 50 years, and by 1978 it was shown that lithium-induced granulocytosis reflects enlargement of the total circulating neutrophil mass due to accelerated neutrophil production [Reference Rothstein, Clarkson and Larsen63, Reference Focosi, Azzara and Kast64]. Lithium’s association with neutrophilia is occasionally misrepresented as the result of neutrophil demargination, but animal and human studies convincingly demonstrate that lithium exposure increases bone marrow organ cellularity, a fact proven in the 1970s and valued by hematologists to manage chemotherapy related neutropenia and to assist with stem cell mobilization prior to bone marrow transplantation [Reference Rothstein, Clarkson and Larsen63, Reference Focosi, Azzara and Kast64]. Multiple placebo-controlled trials reported lithium’s effects for hematology uses in the 1970s and 1980s, and these findings led psychiatric providers to employ lithium for management of mild or moderate neutropenia during clozapine therapy, or to bolster low neutrophil counts prior to clozapine initiation [Reference Mattai, Fung and Bakalar61, Reference Nykiel, Henderson and Bhide62]. The underlying mechanism relates to lithium’s ability to enhance production of granulocyte colony stimulating factor (G-CSF), and thereby stimulate proliferation of pluripotential stem cells resulting in increased bone marrow colony-forming units and bone marrow organ cellularity [Reference Petrini and Azzara65]. This effect occurs reproducibly in animal and human studies, and exhibits a dose dependency within the serum range of 0.30–1.00 mEq/l (0.30–1.00 mmol/l) [Reference Focosi, Azzara and Kast64]. Higher serum levels in animal models did not generate greater effects, and very high levels that would be toxic in humans (5.00 mEq/l or 5.00 mmol/l) cause bone marrow toxicity. At therapeutic doses of 900–1200 mg/day, the mean increase in absolute neutrophil count (ANC) averaged 88% in one small trial, and the effect was seen in the first week after lithium was initiated, although peak ANC values may not occur until week 2 or 3 [Reference Ballin, Lehman and Sirota193]. This property also represents a unique advantage of lithium over VPA when managing clozapine treated patients who require mood stabilization since VPA is associated with a dose dependent risk for neutropenia [Reference Acharya and Bussel194]. A case–control study that examined risk factors for neutropenia during clozapine treatment (n = 272) found that concurrent use of VPA more than doubled the risk for neutropenia (OR 2.28, 95% CI 1.27–4.11, p = 0.006) [Reference Malik, Lally and Ajnakina195]. While lithium induced neutrophilia can be exploited therapeutically, for the majority of patients it is an incidental laboratory finding of no consequence, but one that should be mentioned to patients and other health-care providers to avoid unnecessary alarm, and especially to obviate work-up for infection or for a hematological disorder.
J Lithium’s Mechanisms of Action
Lithium’s dense and interconnected cellular activities continue to be explored in an attempt to understand the biological underpinnings of BD and to develop novel treatments for this mood disorder [Reference Jones, Rong and Shariq196–Reference Tye, Borreggine and Price198]. Decades of research have established that lithium’s mechanisms of action relate to modulation of signal transduction pathways, especially those regulated by inositol monophosphatase (IMPase) and GSK3-β, but also involving numerous other kinases and signaling proteins (e.g. protein kinase C [PKC], phospholipase A2, molecular target of rapamycin [mTOR], Wnt, ErbB, MAP kinase, and vascular endothelial growth factor [VEGF] pathways) [Reference Rapoport199, Reference Akkouh, Skrede and Holmgren200]. Certain mechanisms (e.g. GSK3-β inhibition) overlap with those of antipsychotics and mood stabilizers, but in vitro and in vivo research shows that lithium exhibits distinct properties via direct and indirect effects that result in comparatively greater GSK3-β inhibition [Reference Pasquali, Busceti and Fulceri67]. These basic science findings have led to human trials probing the antimanic effects of IMPase inhibitors such as ebselen, an organoselenium compound developed as an antioxidant [Reference Sharpley, Williams and Holder201], and PKC inhibitors such as tamoxifen, a molecule primarily used as an estrogen receptor modulator [Reference Valvassori, Cararo and Peper-Nascimento202]. The fact that lithium acts on numerous pathways simultaneously implies that it might be difficult to find any single molecule that replicates lithium’s clinical profile, especially the combination of its mood stabilizing, anti-suicide and neuroprotective effects.
Part of lithium’s uniqueness relates to it being a cation ion with similar ionic radius to magnesium (lithium 0.60 Å, magnesium 0.65 Å), thus allowing lithium to compete for binding sites at magnesium-dependent enzymes and other substrates [Reference Pasquali, Busceti and Fulceri67]. Due to their similar radii, lithium’s competition for low affinity magnesium binding sites is independent of the substrate; moreover, this type of interference is not seen with other Group I ions (e.g. potassium, sodium) as their larger size precludes interaction with the magnesium binding site [Reference Pasquali, Busceti and Fulceri67]. The direct relevance of this finding for lithium’s mood stabilizing properties can be seen with in vitro studies, especially those focused on lithium’s core targets, IMPase and GSK3-β. In mammals, IMPase (and several other phosphomonoesterases) are magnesium dependent, and lithium thus inhibits IMPase activity by binding uncompetitively to one of its magnesium sites [Reference Pasquali, Busceti and Fulceri67]. Lithium’s direct inhibitory effect on GSK3-β also arises via competition at magnesium binding sites, with lithium binding resulting in impaired enzyme catalytic activity. It is difficult to predict the extent of lithium’s in vivo direct inhibition of GSK3-β based on in vitro studies, as lithium’s actions will depend on local conditions. Intracellular concentrations of free unbound magnesium range from 0.6 to 1.2 mmol/l, while lithium’s ability to inhibit GSK3-β activity by 50% (IC50) occurs at 2 mmol/l. By keeping cellular magnesium concentration low during in vitro assays, more magnesium binding sites are available, thus decreasing the IC50 for lithium’s GSK3-β inhibition to under 0.8 mmol/l [Reference Pasquali, Busceti and Fulceri67]. This artificial environment provides only limited guidance on the extent of lithium’s GSK3-β inhibition during therapeutic use, but underscores the concept that lithium has direct effects on GSK3-β activity due to its ionic structure, a property that differentiates lithium from other psychotropics used for mood stabilization.
Many of lithium’s actions are hypothesized to be downstream effects of IMPase inhibition and the central role played by the phosphophatidylinositol signaling pathway in regulating multiple cellular functions, including apoptosis and cell growth. Stimulation of certain G-protein coupled receptors results in activation of phospholipase C, an enzyme that hydrolyzes phosphatidylinositol biphosphate (PIP2) to produce diacylglycerol and inositol triphosphate (IP3), both of which have 2nd messenger activities (Figure 1.9) [Reference Pasquali, Busceti and Fulceri67]. It is worth noting that PIP2 is not only a precursor to these signaling molecules, it can also be phosphorylated to become PIP3, which is itself involved in cell movement, proliferation and apoptosis [Reference Pasquali, Busceti and Fulceri67]. Among the two products of PIP2 hydrolysis, diacylglycerol activates several protein kinases such as PKC, while IP3 induces release of calcium stores from endoplasmic reticulum into the cytoplasm. Both of these processes create significant downstream signals. At the neuronal level, the combined effects of diacylglycerol and IP3 impinge on fundamental processes such as plasticity and long-term potentiation, and one regulator of PIP2 availability is the enzyme IMPase. This enzyme catalyzes the final step in converting IP3 to produce PIP2 by dephosphorylating inositol 1-monophosphate to produce inorganic phosphate and inositol, the precursor to PIP2. Lithium inhibits both IMPase and inositol polyphosphate phosphatase (IPP) thereby reducing the intracellular availability of free inositol and limiting the formation of PIP2 and IP3 [Reference Pasquali, Busceti and Fulceri67]. Among the cellular processes highly correlated with these actions is autophagy, the normal process by which cells remove old or degraded elements via lysosomes. Animal models demonstrate that lithium related stimulation of autophagy counteracts those forces inducing neurodegeneration, and this may be crucial for lithium’s effects on mood and cognition [Reference Pasquali, Busceti and Fulceri67]. Another result of IPP inhibition is increased intracellular levels of inositol 1-monophosphate, the substrate of IMPase. Higher levels of inositol 1-monophosphate further reduce IMPase activity by limiting the amount of unbound enzyme available to catalyze inositol 1-monophosphate dephosphorylation. In addition to autophagy induction, multiple G-protein coupled receptor pathways are also regulated in a PIP2 dependent manner, including specific muscarinic cholinergic, serotonergic and dopaminergic receptors. These effects may also be part of lithium’s mood related properties.

Figure 1.9 How lithium interacts with the phosphatidylinositol pathway by inhibiting the conversion of inositol triphosphate (IP3) to free inositol [67]
As mentioned in the Introduction, lithium moderates the downstream signal from dopamine D2 receptor stimulation, and this is considered an important aspect of its antimanic actions [Reference Beaulieu, Gainetdinov and Caron203, Reference Beaulieu, Del’guidice and Sotnikova204]. Activation of postsynaptic D2 receptors by direct agonists or presynaptic dopamine releasing agents (e.g. amphetamine) induces effects on G-protein dependent and non-G-protein pathways (Figure 1.10), each of which moderate different behaviors. The hyperlocomotion induced by D2 receptor agonists or amphetamines is associated with actions on a pathway that involves a scaffolding protein, β-arrestin2, and the net increase in GSK3-β activity. Binding of dopamine to D2 (and other G-protein coupled receptors) recruits β-arrestin2 and supports formation of the stable complex of β-arrestin2, protein phosphatase 2A (PP2A) and the kinase Akt. Formation of this complex allows PP2A to phosphorylate and inactivate Akt. Inactivated Akt is no longer able to phosphorylate GSK3-β on its serine 9 residue, with the result that GSK3-β remains active. Not surprisingly, in blocking dopamine D2 binding, antipsychotics inhibit β-arrestin2 recruitment and subsequent formation of the Akt/β-arrestin2/PP2A complex, thus allowing Akt to remain more active and inhibit GSK3-β [Reference Beaulieu, Del’guidice and Sotnikova204, Reference Beaulieu, Marion and Rodriguiz205]. At concentrations that overlap with clinically effective serum levels (0.50–1.00 mEq/l), lithium destabilizes formation of the Akt/β-arrestin2/PP2A complex, leading to increased levels of activated Akt, and therefore greater inactivation of GSK3-β [Reference Del’ Guidice and Beaulieu13]. This destabilizing property, which indirectly reduces GSK3-β activity, is shared with lamotrigine and valproate, but what distinguishes lithium is its additional direct actions on GSK3-β through binding at the magnesium site [Reference Pasquali, Busceti and Fulceri67]. The net result is greater GSK3-β inhibition, a factor that may be relevant to mood stabilization, but also to lithium’s neuroprotective properties. Increased GSK3-β activity induces apoptosis in neurons, while decreasing GSK3-β activity either with lithium or other methods counteracts these effects. The protective properties from GSK3-β inhibition are in part mediated by effects on β-catenin. Inactive GSK3-β allows the active nonphosphorylated form of β-catenin to enter the nucleus, form a complex with the DNA-binding protein T-cell factor and activate transcription of a wide variety of genes, particularly growth promoting genes such as VEGF and other growth factors [Reference Pasquali, Busceti and Fulceri67]. The more robust inhibition of GSK3-β activity by lithium than that by other mood stabilizers is postulated to be a contributing factor in lithium’s neuroprotective effects (e.g. reduced dementia rates), clinical effects not seen with anticonvulsant mood stabilizers. Lithium indeed has complex actions that are still being understood, but the molecular evidence points to an array of actions that act synergistically to generate lithium’s unique signature of clinical benefits.

Figure 1.10 How dopamine D2 receptor agonists recruit β-arrestin2, resulting in decreased Akt activity and increased GSK3-β activity, manifested as hyperlocomotion [13, 203, 204]
Summary Points
a. Lithium has significant efficacy data for acute mania, and is considered the gold standard for maintenance treatment in patients with a history of mania (BD-1, SAD-BT). Older age or a history of rapid cycling are not reasons to eschew lithium – it is no less effective than other options. Lithium can be used for BD-2 patients who require mood stabilization, but is not demonstrably superior to other options.
b. Lithium’s impact on suicide attempts and risk of completed suicide cannot be proven in the context of randomized clinical trials; however, the retrospective data are largely consistent that these are unique properties of lithium not seen to the same extent with other mood stabilizers. This effect may also be greater with BD spectrum patients than for other psychiatric diagnoses. Lithium does not have data supporting use for acute bipolar depression, but is effective as an adjunct to antidepressants for unipolar major depression. Lithium’s prospective anti-aggression data are not of high quality and it is not routinely used to manage conduct disorder in children/adolescents, with limited data to support its value for impulsive behavior in those with intellectual disability or borderline personality disorder.
c. Lithium has extensive preclinical and clinical evidence demonstrating its neuroprotective properties. BD spectrum patients have 3-fold higher risk of dementia, and multiple studies indicate that use of lithium in older BD patients reduces this risk by 50%. This is one of the most compelling reasons to continue lithium therapy in older patients.
d. Lithium stimulates neutrophil production by increasing levels of granulocyte colony stimulating factor. Patients should be advised of this to avoid unnecessary medical work-up for other causes. This property is commonly exploited in the management of clozapine treated patients as a means to boost absolute neutrophil counts.
e. Lithium impacts numerous intracellular pathways, and these mechanisms differentially contribute to its mood stabilizing, anti-suicide and neuroprotective clinical profile. In animal models, lithium interferes with amphetamine induced hyperlocomotion from striatal dopamine D2 receptor stimulation by destabilizing β-arrestin2 complex formation and decreasing GSK3-β activity. This property is considered central to lithium’s antimanic activity. No single medication replicates all of lithium’s 2nd messenger effects and its clinical profile.