



The 2019 novel coronavirus (2019-nCoV) was discovered in Wuhan in December 2019, and the disease spread rapidly in other provinces in China, Reference Hui, Azhar and Madani1 which was subsequently named novel coronavirus disease 2019 (COVID-19). According to data released by the National Health Commission of China, as of March 10, 2020, the number of confirmed cases in mainland China has increased to 80,778, with a total of 3158 deaths. 2 In addition, human-to-human transmission has also occurred in many countries and regions outside mainland China. Reference Rothe, Schunk and Sothmann3 As of March 12, there were 114 countries in the world with hundreds of thousands of people infected with the disease and WHO defines it was a global pandemic. 4 The 2019-nCoV was also known as severe acute respiratory syndrome coronavirus (SARS-CoV-2), which was mainly transmitted by means of respiratory droplets and contact, and the population was generally more susceptible than the SARS virus that broke out in 2003. Reference Lu, Liu and Jia5 The clinical symptoms of COVID-19 include headache, fever, cough, muscle pain, dyspnea, hemoptysis fatigue, and diarrhea. Reference Huang, Wang and Li6 Due to the lack of targeted and effective treatments, the best way to deal with the novel coronavirus pneumonia pandemic is to control the source of infection, cut off the transmission route, and protect vulnerable populations. Specific strategies include strengthening hand hygiene and wearing masks, avoiding large gatherings, tracking the health of company employees, disinfecting the workplace, stopping the use of central air conditioning and enhancing indoor ventilation, encouraging people to exercise regularly, and ensuring adequate rest. Reference Tan, Hao and McIntyre7 People’s knowledge of disease-related prevention and control COVID-19 would affect the effectiveness of self-protection measures to a certain extent.
Since the outbreak of the COVID-19 epidemic, the Chinese government has quickly adopted response measures and has taken travel-restrictive actions in many provinces and cities to curb the spread of the virus. Reference Wu and McGoogan8 Many people isolated themselves at home to prevent infection, and some people gradually developed panic symptoms, depression, anxiety, stress, posttraumatic stress symptoms, and insomnia. Reference Wang, Pan and Wan9-Reference Wang, Pan and Wan11 Because the COVID-19 epidemic has no specific vaccine and can only be treated symptomatically, this has become a major source of stress for diagnosed patients with COVID-19. Previous studies have shown that patients with large infectious diseases, such as SARS, can produce varying degrees of anxiety, depression, stress, and posttraumatic stress disorder, which severely affect patients’ rehabilitation and quality of life. Reference Wu, Chan and Ma12,Reference Mak, Chu and Pan13
Disease-related knowledge is very important for patients, it can improve treatment compliance and mental health. Reference Molenaar, Sprangers and Rutgers14,Reference Yoo, Cho and Cha15 Previous studies have shown that lack of knowledge or health information related to COVID-19 can increased patients’ anxiety and depression, and severely reduce their mental health. Reference Wang, Pan and Wan9,Reference Tran, Dang and Thai16 Improving disease-related knowledge would reduce patient anxiety, improve treatment compliance and satisfaction, and reduce treatment costs. Reference Wang, Pan and Wan9,Reference Molenaar, Sprangers and Rutgers14 Obtaining appropriate disease-related knowledge could enable patients to effectively cope with themselves before they visit a doctor. Reference Casellas, Fontanet and Borruel17 Illness perception is the patient’s view of the current disease. It affected the patient’s emotions, coping strategies, treatment compliance, and disease outcomes. Reference Bassi, Grobberio and Negri18,Reference Velez-Velez and Bosch19 Previous studies have shown that illness perception was constrained by multiple factors, such as the cause of the disease, clinical symptoms, and prognosis. Reference Velez-Velez and Bosch19
The ongoing COVID-19 epidemic is spreading globally, and maintaining the healthy mental health of patients is an urgent need for society. However, few studies have been conducted on disease-related knowledge and its effects on illness perception and mental state in patients with COVID-19. The purpose of this study was to assess the current status of disease-related knowledge of patients with COVID-19 and to analyze its relationship among the general condition, illness perception, and psychological status of patients. This study may provide a good reference for government agencies and health-care professionals in China and other countries or regions to effectively protect the mental health of diagnosed patients and other people in the face of the expanding COVID-19 epidemic.
Methods
Setting and Participants
This study was a cross-sectional design. A total of 118 inpatients with COVID-19 at the designated hospitals in Hunan Province in February 2020 were selected for this study. Inclusion criteria: (1) patients diagnosed according to the COVID-19 diagnosis and treatment plan (Trial Version-5); (2) over 18 y of age; (3) normal reading and writing ability, understand the questionnaire content; (4) can use WeChat-related functions correctly; (5) informed consent, and voluntarily participated in this study. Exclusion criteria: (1) patients with severe mental disorders; (2) patients with organic brain lesions and malignant tumors.
Procedure
Due to the highly contagious nature of COVID-19, to avoid spreading the virus during the filling and recycling of paper questionnaires, this study used on-site recruitment and guidance, and filled out the questionnaires online for data collection. All patients used WeChat to scan the quick response (QR) code on the website and filled out the survey form. Each participant completed this cross-sectional survey with the help of 2 trained research nurses. The questionnaire was completed in accordance with uniform guidelines. A total of 118 questionnaires were distributed, and all of them were recovered in this study. The effective recovery rate was 100%.
Ethical Considerations
This study was approved by the Medical Ethics Committee of the Second Xiangya Hospital of Central South University (Approval Number: 2020015), which was consistent with the principles embodied in the Declaration of Helsinki. Researchers explained the purpose and significance of the study to patients before the survey. All participants provided informed consent.
Measurements
General Information Questionnaire
It was designed by the researcher, including sociodemographic data (age, gender, education, occupation, marital status, etc.) and the general condition of the patient (self-care ability, appetite, endurance of activity, sleep, mood condition, negative effects of disease, etc.).
Disease-Related Knowledge Questionnaire of COVID-19
The questionnaire (see supplementary material) was designed by researchers based on the COVID-19 diagnosis and treatment plan (Trial Version-5). There were 25 items in the questionnaire, of which 13 items were diagnosis and treatment knowledge (etiological characteristics, epidemiological characteristics, clinical manifestations and classification, diagnosis, treatment, nursing, prognosis, and discharge criteria of the disease, etc.) and 12 items of prevention and control knowledge (How to do home isolation, personal protection, daily cleaning and sanitation, environmental and article cleaning management, etc.). Each item was designed as a single-choice question. The correct answer was 4 points, and the incorrect answer was not counted. The highest score on the questionnaire was 100 points. The higher the score, the better the knowledge level. In this study, the overall questionnaire Cronbach’s α was 0.767, the Cronbach’s α of diagnosis and treatment knowledge dimension was 0.638, and the Cronbach’s α of prevention and control knowledge dimension was 0.632. The overall reliability was good.
Illness Perception Questionnaire
The Illness Perception Question (IPQ) was developed by Weinman et al. Reference Weinman, Petrie and Moss-Morris20 and revised by Moss-Morris et al. Reference Moss-Morris, Weinman and Petrie21 The Chinese version designed by Xiong et al. Reference Xiong, Wei and Hong22 was used to investigate the illness perception in this study. The scale was divided into 3 parts: symptoms identity, illness representation, and causes. In this study, only the illness representation part was selected to evaluate COVID-19 patients. It included 7 dimensions, including course of disease, volatility, consequences, personal control, treatment control, disease coherence, and emotional statement, with a total of 38 items. All items were scored on a 5-point Likert scale (1 = strongly disagree; 5 = strongly agree). The Cronbach’s α of each factor of the illness representation questionnaire fluctuated from 0.80 to 0.91, and the reliability and validity were good. Reference Xiong, Wei and Hong22
Profile of Mood States
The POMS was developed by McNair in 1971, Reference Perciavalle, Blandini and Fecarotta23 and the Chinese version was translated and revised by Zhu. Reference Zhu24 There were 40 items on the scale, which were divided into 7 dimensions of tension, anger, fatigue, depression, vigor, confusion, and self-esteem. Each item is scored on a scale of 0 to 4 (0 = never; 4 = almost always), the higher the energy and self-esteem dimensions, the better the emotional state, and the higher scores in the other 5 dimensions, the worse the emotional state. Total Mood Disturbance (TMD) = total negative emotion score (tension, anger, fatigue, depression, confusion)-total positive emotion score (vigor, self-esteem) +100. A higher TMD score indicated a more negative emotional state. The scale had good reliability and validity, and can accurately reflect the psychological state of the subjects. Reference Loh, Kleckner and Lin25
Statistical Analysis
SPSS 20.0 software was adopted to analyze the data. Count data were expressed by frequency and percentage, measurement data were described by mean and standard deviation (¯x ± SD), and analysis of variance (ANOVA) was used to compare the differences in disease-related knowledge among patients in different groups; Spearman correlation analysis was used to explore the correlation between disease-related knowledge and illness perception and psychological status. The level of statistical significance was P < 0.05.
Results
Current Status of Disease-Related Knowledge in Patients With COVID-19
Overall Status of COVID-19 Disease-Related Knowledge Scores
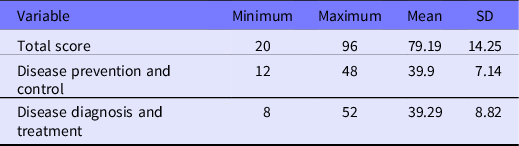
The disease diagnosis and treatment knowledge of patients with COVID-19 was (39.29 ± 8.82), the score of disease prevention and control knowledge was (39.90 ± 7.14), and the total score of disease-related knowledge was (79.19 ± 14.25), which was at a moderately high level. However, there were still some patients with low level of knowledge, manifested as a minimum of 20 points for the total score of disease-related knowledge, 12 points for prevention and control knowledge, and 8 points for disease diagnosis and treatment. The results were shown in Table 1.
Table 1. Score of disease-related knowledge of COVID-19 (n = 118)
Disease-Related Knowledge of COVID-19 in Different Demographic Characteristics
ANOVA analysis showed that in terms of disease diagnosis and treatment knowledge, there were significant differences in the COVID-19 patients of different age (F = 8.681; P = 0.000), the self-conceived possibility of being infected before see the doctor (F = 4.627; P = 0.002), education level (F = 7.984; P = 0.000), and monthly income (F = 2.747; P = 0.022). In terms of disease prevention and control knowledge, there were significant differences in the COVID-19 patients of different age (F = 4.659; P = 0.004), the self-conceived possibility of being-infected before see the doctor (F = 3.504; P = 0.010), and the attention to the publicity of COVID-19 (F = 3.373; P = 0.038). In terms of the total score of disease-related knowledge, there were significant differences in the COVID-19 patients of different age (F = 8.548; P = 0.000), the self-conceived possibility of being-infected before see the doctor (F = 4.887; P = 0.001), education level (F = 4.964; P = 0.003), monthly income (F = 2.940; P = 0.016), and the attention to the publicity of COVID-19 (F = 3.107; P = 0.049).
The SNK analysis showed that patients who were 31 to 45 y old and who had a high self-conceived possibility of being-infected before see the doctor have higher scores in disease diagnosis and treatment knowledge, disease prevention and control knowledge, and total disease-related knowledge than those in other groups (P < 0.01). Patients with a bachelor’s degree or above and a better monthly income showed higher scores in disease diagnosis and treatment knowledge and total disease-related knowledge (P < 0.01). Patients with higher attention to the publicity of COVID-19 have showed better scores in disease prevention and control knowledge and total disease-related knowledge (P < 0.05) (Table 2).
Table 2. Characteristics and disease-related knowledge in COVID-19 patients (n = 118)
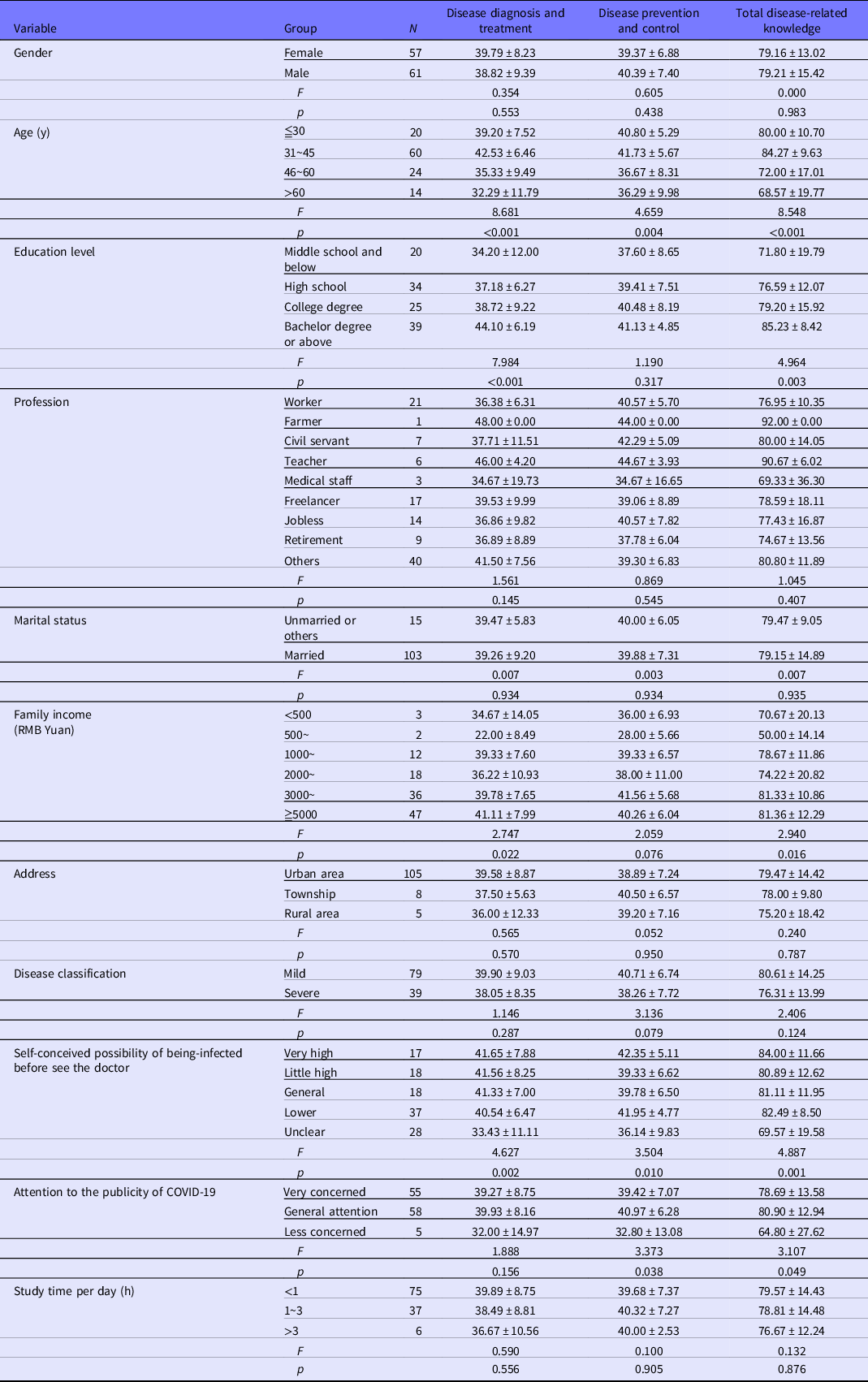
Note: ANOVA analysis was used to compare the mean score of disease-related knowledge among different groups of COVID-19 patients.
Correlation Between Disease-Related Knowledge and General Status
Spearman correlation analysis showed that the self-care situation was positively correlated with disease prevention and control knowledge (r = 0.265; P = 0.004) and total score of disease-related knowledge (r = 0.206; P = 0.025); the degree of anxiety was negatively correlated with the disease diagnosis and treatment knowledge (r = −0.182; P = 0.049) (Table 3).
Table 3. Correlation among disease-related knowledge, general status, illness perception, and psychological status (n = 118)
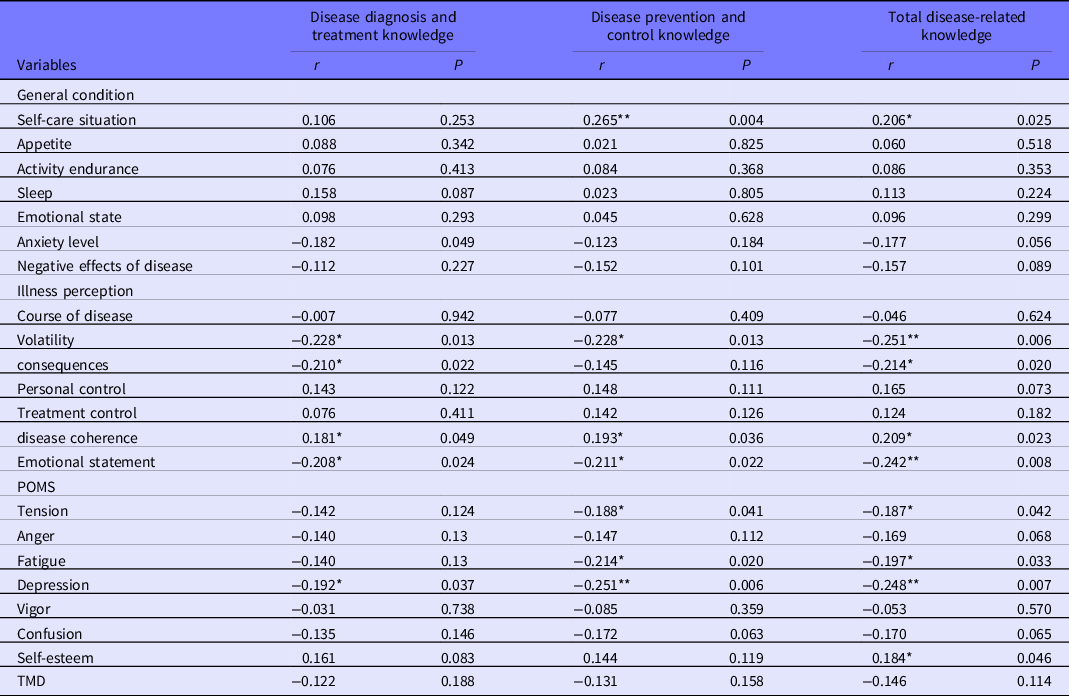
Note: Spearman correlation was used to analyze the correlation among the study variables.
* P < 0.05 (2-tailed).
** P < 0.01 (2-tailed).
Correlation Between Disease-Related Knowledge and Illness Perception
Spearman correlation analysis showed that the volatility, emotional statements were negatively correlated with the disease diagnosis and treatment knowledge, disease prevention and control knowledge, and total disease-related knowledge (P < 0.05). The disease coherence was positively correlated with the disease diagnosis and treatment knowledge, disease prevention and control knowledge, and total disease-related knowledge (P < 0.05). The consequences were negatively correlated with the disease diagnosis and treatment knowledge and the total score of disease-related knowledge (P < 0.05) (Table 3).
Correlation Between Disease-Related Knowledge and Psychological Status
Spearman correlation analysis has shown that tension and fatigue were negatively correlated with the disease prevention and control knowledge and total score of disease-related knowledge (P < 0.05). Depression was negatively correlated with the disease diagnosis and treatment knowledge, disease prevention and control knowledge, and total score of disease-related knowledge (P < 0.05). Self-esteem was positively correlated with total score of disease-related knowledge (P < 0.05) (Table 3).
Discussion
Our study confirmed that the disease diagnosis and treatment knowledge, disease prevention and control knowledge, and total disease-related knowledge of COVID-19 patients were at a upper-middle level, but there were still some patients who did not know enough about the COVID-19, and the score of disease diagnosis and treatment knowledge was lower than the disease prevention and control knowledge. This was consistent with the current situation. Before the outbreak of novel coronavirus pneumonia, the general public had no idea about the disease. After the epidemic broke out in January 2020, to control the situation as soon as possible, the Chinese government focused on the promotion of COVID-19 prevention and control knowledge online and offline nationwide, Reference Ye, Wang and Mao26 including the use of TV media for all-day broadcast. Meanwhile, the communities and government staff carried out the publicity education from door to door, Reference Liu, Yue and Tchounwou27 which had increased the coverage and popularity of disease-related knowledge.
At the same time, with the exponential growth of confirmed cases in the early stages of the outbreak, people were generally willing to actively seek disease-related knowledge to protect themselves. Under the influence of multiple factors, the overall level of disease-related knowledge of COVID-19 patients was better. However, because these propaganda contents were mainly disease prevention and control, and the diagnosis and treatment plan had been continuously explored and improved, the level of disease diagnosis and treatment knowledge was lower than the disease prevention and control knowledge in this study. As there were some patients who still had a low level of disease-related knowledge, it was recommended to strengthen the health education for COVID-19 patients based on the existing situation, and increase the content of diagnosis and treatment of COVID-19 and self-care methods in the follow-up nursing process.
It was found that patients with higher family incomes and education levels, and those from 31 to 45 y of age had higher levels of disease-related knowledge than others, which were similar with the previous findings. Reference Yoo, Cho and Cha15,Reference Tran, Vu and Latkin28 This might be because young and middle-aged people and those with higher education and monthly income are more concerned about their health, have more access to disease-related knowledge, and have better understanding and memory of disease-related knowledge.
In addition, patients who have a high self-conceived possibility of being-infected before they see the doctor also have shown better disease-related knowledge. This might be because such patients have a clearer understanding of the disease infectiousness and pathogenicity based on their own conditions, and will more actively seek disease-related knowledge. Studies have also shown that people who pay close attention to the publicity of COVID-19 have higher levels of disease-related knowledge. The above results suggested that, when conducting health education in the future, medical staff should pay more attention to the elderly, low-education, and low-income patients, timely collect their feedback of training and education content, and effectively improve the patient’s disease-related knowledge level.
It was also shown that the higher the level of disease-related knowledge, the better the ability of self-care, and the lower the level of anxiety, which was consistent with previous results. Reference Molenaar, Sprangers and Rutgers14,Reference Song and Karako29 This illustrated the importance of disease-related knowledge for COVID-19 patients during epidemic prevention and control. Anxiety is a manifestation of psychological stress. When the degree of uncontrollable and unpredictable incidents perceived by an individual is higher, the individual’s fear and anxiety will increase, causing irrational anxiety. Reference Wang, Pan and Wan11 As a public health emergency, COVID-19 is a major source of stress for patients. Reference Lu, Liu and Jia5 After patients acquire disease-related knowledge, they will consider the COVID-19 is preventable and controllable, which will help them to reduce anxiety and maintain rational behavior. This will also improve their treatment compliance and self-care ability, and increase their awareness of health, so that they can master the 7-step hand-washing method, wearing a mask, and daily disinfection methods to protect themselves and others from being infected. This result indicates that medical staff should promptly inform patients of the new progress of the current diagnosis and treatment, reduce negative emotion, and promote the cooperation and support of patients in treatment, nursing care, and self-isolation.
This study indicated that the more disease-related knowledge a patient had, the lower the disease-related negative cognition (volatility, consequences, and emotional statements), and the better the disease-related positive cognition (disease coherence). The positive cognition skills can be incorporated into cognitive behavior therapy, which was found to be effective to treat psychiatric conditions during the COVID-19 pandemic. Reference Ho, Chee and Ho30 Volatility and consequences refer to the repetitiveness and severity of the patient’s own disease and the extent to which the disease affects the patient’s physical and social functions; the emotional statement reflects the psychological pressure of the disease on the patient; the sense of disease agreement reflects the patients’ understanding of their disease. Reference Bassi, Grobberio and Negri18,Reference Mosleh and Almalik31
In previous studies, disease awareness was able to predict disease-related coping behaviors, such as seeking medical help and treatment compliance. Reference Velez-Velez and Bosch19,Reference Mosleh and Almalik31 Therefore, improving COVID-19 patients’ awareness of the disease can enhance their symptom recognition ability, enhance self-protection ability, and enable them to better cooperate with the hospital’s treatment and isolation protocols. While improving disease-related knowledge, it is recommended to carry out interventions based on the theory of knowledge-attitude-practice to improve patients’ and the general population’s awareness of the disease, thereby promoting healthy behaviors to achieve the purpose of controlling the source of infection, cutting off the route of transmission, and protecting vulnerable populations.
This study indicates that, as patients gain more disease-related knowledge, the fewer negative emotions they have, including tension, fatigue, and depression. Studies have shown that survivors of the SARS epidemic in 2003 suffered a series of emotional stresses such as anxiety, anger, nervousness, and depression. Reference Lee, Wong and McAlonan32 Under the stimulation of this emotional response and stressors, people will also form corresponding self-defensive mechanisms, Reference Cramer33,Reference Babl, Grosse Holtforth and Perry34 such as denial mechanisms (denying illness, not cooperating with treatment), transfer mechanisms (not understanding isolation measures, anger at medical care), which can alleviate psychological pain to a certain extent, but they can prevent rational thinking and problem solving. Reference Liang35 As a public health emergency of the same type as SARS, the psychological state and defense mechanisms of COVID-19 patients are similar. Therefore, to reduce the impact of poor psychological defense mechanisms on patients, it is possible to enhance patients’ awareness of diseases by strengthening education on disease-related knowledge.
Strengths and Limitations of the Study
Our research had some limitations. First, like all cross-sectional studies, this study could not explain the relationship between disease-related knowledge and the long-term effects of mental state and disease perception. It would be better to conduct a prospective study on these participants later. However, the ethical requirements of anonymity and confidentiality did not allow us to collect personal information of research participants, so this prospective study could not be conducted. Second, all demographic and main assessment indicators of the psychological states were reported by the patients themselves, which might lead to reporting bias. In addition, this study was conducted only in Hunan, China, and might not be representative of all COVID-19 patients. In future studies, it was necessary to expand the sample size and research sites to reduce these deviations. Notwithstanding the above limitations, our results provided valuable information for the relationship between disease-related knowledge, psychological status, and illness perception of COVID-19 patients. Most importantly, our findings could directly guide psychological cognition interventions, which could minimize the negative psychological impact and improve the knowledge of disease prevention and treatment and treatment of patients and ordinary people to maintain physical and mental health during the COVID-19 pandemic.
Conclusions
COVID-19 is a public health emergency that poses a huge threat to people’s lives, health, and safety. With the joint efforts of the Chinese government and individuals, the current disease-related knowledge of COVID-19 patients was at a moderately high level. Universal health education still needs to be further strengthened, especially paying attention to the elderly and low-income groups, and the content should also increase the knowledge of diseases diagnosis and treatment and self-care. Based on the strong correlation between disease-related knowledge and the patient’s general condition, illness perception, and psychological status, future research can carry out interventions based on the theory of knowledge-attitude-practice to improve patients and the general population’s awareness of the disease. At the same time, the role of cognitive behavioral intervention and psychotherapy in reducing the psychological stress response can be explored to continuously promote the comprehensive physical and psychological recovery of the patients with COVID-19.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/dmp.2021.33
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank all the researchers and participants in this study.
Author Contributions
The study was designed by H.J., Y.M., Q.T., and L.Y. Data collection was performed by H.J., Y.M., X.C., C.Y., and Z.J. Data analysis was performed by Y.M., C.S., L.X., and M.R. The first draft of the manuscript was written by Y.M., C.S., L.X., and H.J. The manuscript was reviewed and revised by L.Y., Z.H., and C.Q. All authors commented on previous versions of the manuscript. All authors have read and approved the final version of the manuscript. Drs. Man Ye and Shi-hao Chen contributed equally to this work.
Funding
This study was supported by the Special Funds of Hunan Innovative Province Construction, China (grant number: 2020SK3003).
Conflicts of Interest
The authors confirm that there are no conflicts of interest to declare.






 Open access
Open access