



Introduction
Epistaxis is the second most common ENT presentation to the hospital (following sore throat), affecting roughly 60 per cent of the population at least once over a lifetime.Reference Barnes, Spielmann and White1,Reference Mehta, Stevens, Smith, Williams, Ellis and Hardman2 There are approximately 25 000 acute epistaxis presentations to the emergency department each year.3 If poorly managed, epistaxis can lead to massive bleeding and, in rare cases, death. More often, it can have a significant impact on a patient's quality of life and involve frequent attendance to the emergency department. Epistaxis normally arises from the anterior septum known as Little's area, also known as Kiesselbach's plexus, which is a vascular network of the anterior ethmoidal, posterior ethmoidal, sphenopalatine, greater palatine and septal branch of the superior labial artery.Reference Pope and Hobbs4 Causes of bleeding can be local or systemic.Reference Clark, Berry, Martin, Harris, Sprecher and Olitsky5,Reference Parajuli6
The 2017 ‘Integrate’ National ENT Trainee Research Network consensus, however, established that recommendations regarding use of first aid techniques remain absent or low quality.7 If first aid is delivered appropriately, this can quickly resolve the issue and prevent emergency department attendance.
In the majority of cases, simple conservative first aid methods can stop the bleeding.Reference Tunkel, Anne, Payne, Ishman, Rosenfeld and Abramson8,Reference Ho and Chan9 The accepted first aid methods supported by the National Institute for Health and Care Excellence (NICE) are: (1) compression performed over the ala nasi for approximately 15 minutes to compress the septum;Reference Kucik and Clenney10 and (2) tilting the head forward to stop blood from passing posteriorly in order to prevent aspiration and allow blood to be spat out (Figure 1).Reference Schlosser11

Fig. 1. Demonstration of correct first aid method in epistaxis.
Other common advice includes the use of ice to vasoconstrict the nasal blood vessels. The most widely published technique is to apply ice over the nose, although this has been challenged by studies showing that ice in the mouth is superior in reducing nasal blood flow.Reference Mulla, Prowse, Sanders and Nix12–Reference Porter15 If first aid fails, then attendance to emergency services can be arranged for consideration of cauterisation, anterior or posterior nasal packing, or radiological or surgical intervention.Reference Newton, Lasso, Petrcich and Kilty16,Reference Kitamura, Takenaka, Takeda, Oya, Ashida and Shimizu17
The authors’ experience is that patients are often incorrectly advised by medical professionals regarding the first aid technique to be used. Studies have evidenced the need for further education of healthcare workers in these methods.3,7 Thus, we wanted to compare epistaxis management knowledge between those who had received medical training and those who had not. We wanted to compare knowledge amongst subspecialty groups of healthcare workers who commonly have to deal with epistaxis. Our primary aim was to determine whether NICE guidance is correctly being recommended and actioned: (1) is the correct part of the nose being compressed?; and (2) is the head being tilted to the correct position?
Our secondary aim was to identify knowledge amongst these groups regarding additional adjunct treatments, specifically ice use. If ice use was recommended as an adjunct treatment, we wanted to determine whether this referred to ice over the nose, ice in the mouth or site unspecified. This was to identify whether there had been a shift in the site of ice use being recommended, as studies have shown that nasal temperature and vasoconstriction are influenced by ice in the mouth rather than ice on the nasal dorsum.Reference Manjaly, Konieczny and Holland13,Reference Porter15
Methods
A cross-sectional study was conducted involving healthcare workers and adult members of the public at a London teaching hospital. We selected the subspecialties of healthcare workers most likely to provide epistaxis first aid management: emergency department doctors, emergency department nurses (including advanced nurse practitioners), hospital ward doctors, hospital ward nurses and general practitioners.
Participants were invited to complete an anonymised questionnaire (Figure 2) on Google Forms survey administration software between 1 December 2020 and 1 March 2021. The questionnaire collected data on the participants’ occupation (specifically whether a healthcare worker, and, if so, their specialty, or whether a member of the general public). We stopped data collection when we had approximately 100 healthcare workers and 100 members of the general public. We questioned the ideal site of nose-pinching and ideal head positioning. Free text was selected to collect responses about the use of adjunct treatments to avoid a leading question. Adjunct treatment was categorised as: (1) no mention of ice; (2) ice on the nose; (3) ice in the mouth; and (4) ice use recommended but site not mentioned.

Fig. 2. Questionnaire given to participants. ED = emergency department; GP = general practitioner
Data were recorded using the Google Sheets spreadsheet program. Statistical analysis was carried out using Fisher's exact test.
Results
Of the healthcare workers, 100 individuals completed the survey. These consisted of 20 emergency department doctors, 20 emergency department nurses, 20 hospital ward doctors, 20 hospital ward nurses and 20 general practitioners. A total of 103 members of the general public completed the survey (Table 1).
Table 1. Summary of participants’ questionnaire answers

Data represent numbers (and percentages) of respondents. ED = emergency department; GP = general practitioner
Primary outcomes
We first asked where the nose should be pinched during epistaxis to stem bleeding. Five options were given with regard to pinching the nose (Figure 2). Overall, 24 per cent of healthcare workers answered correctly, pinching the ala nasi, whilst 25.2 per cent of the public reported they would pinch this same site. Within the healthcare worker subspecialties, 30 per cent of emergency department doctors, 15 per cent of emergency department nurses, 25 per cent of ward doctors, 15 per cent of ward nurses and 35 per cent of general practitioners answered this question correctly (Figure 3).

Fig. 3. Graphical representation of site of nasal pinching advice given by healthcare workers and non-healthcare workers during epistaxis management. ED = emergency department; GP = general practitioner
Sixty-eight per cent of healthcare workers correctly said that they would tilt the head forward compared with the 37.9 per cent of the public who reported the same answer. Amongst healthcare workers, 75 per cent of emergency department doctors, 60 per cent of emergency department nurses, 85 per cent of ward doctors, 70 per cent of ward nurses and 50 per cent of general practitioners answered that they would tilt the head forward (Figure 4).
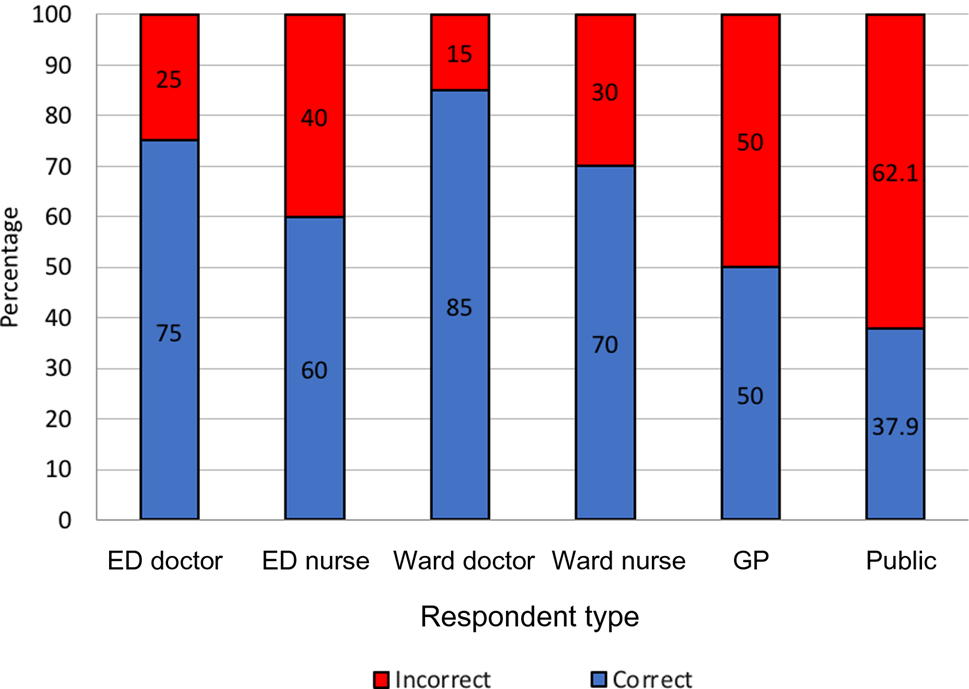
Fig. 4. Graphical representation of head positioning advice given by healthcare workers and non-healthcare workers during epistaxis management. ED = emergency department; GP = general practitioner
Fisher's exact test revealed no statistically significant difference between the knowledge of healthcare workers and of the general public regarding nasal pinching position (p = 0.87). There was, however, a statistically significant difference between the two groups regarding head position (p < 0.001).
Secondary outcome – adjunct use
In order to analyse adjunct treatment use, free text answers were categorised into: (1) no mention of ice; (2) ice on the nose; (3) ice in the mouth; or (4) ice use recommended but site not mentioned. Twenty-eight healthcare workers (28 per cent) compared with five members of the public (4.9 per cent) mentioned ice use as an adjunct treatment. Twenty-four per cent of healthcare workers mentioned ice use as an adjunct treatment but without mentioning the site, 2 per cent stated ice use on the nose and another 2 per cent reported ice use in the mouth. In contrast, amongst the general public, 4.9 per cent reported ice use with no mention of site, whilst no member of the public mentioned using ice on either the nose or in the mouth to treat bleeding. When the healthcare workers were divided into subspecialties, 25 per cent of emergency department doctors, 20 per cent of emergency department nurses, 20 per cent of ward doctors, 20 per cent of ward nurses and 25 per cent of general practitioners mentioned ice use without specifying a site. Only 5 per cent of emergency department doctors and 5 per cent of general practitioners specified ice use on the nose, whilst this figure was 0 per cent for emergency department nurses, ward doctors and ward nurses. Similarly, only 5 per cent of emergency department doctors and 5 per cent of ward nurses mentioned ice use in the mouth. Of each of the remaining groups, 0 per cent reported ice use in the mouth as an adjunct treatment (Figure 5).

Fig. 5. Graphical representation of adjunct treatment advice given by healthcare workers and non-healthcare workers during epistaxis management. ED = emergency department; GP = general practitioner
Analysis revealed no significant difference between healthcare workers and the public when comparing those who reported ice use on the nose (p = 0.24) and ice use in the mouth (p = 0.24) as an adjunct treatment. When comparing those who reported recommending ice use but without mentioning site, there was a statistically significant difference between the two groups (p < 0.001).
Discussion
A previous study conducted in 1998 surveying the general public's knowledge of epistaxis identified a high level of ignorance amongst the public, with only 35 per cent choosing the correct nasal pinching site and 36 per cent choosing the correct head position.Reference Strachan and England18 A more recent study corroborated ongoing poor patient understanding, with 68 per cent of the patient cohort incorrectly identifying the hard bony portion as the site of nasal pinching to control epistaxis.Reference Fishman, Brooks and Banfield19 Unfortunately, from our study, little improvement was identified amongst the public, with 25.2 per cent and 37.9 per cent correctly answering the nasal pinching site and head position questions, respectively.
Studies on various frontline healthcare workers have also confirmed poor knowledge of epistaxis management. A previous survey of emergency staff, conducted in 1993, highlighted an overall correct response rate of 36 per cent amongst clinical staff when asked to demonstrate the correct nasal pinching technique.Reference McGarry and Moulton20 Another study, examining knowledge of epistaxis management amongst advanced nurse practitioners and senior nursing staff, identified that only 12 per cent and 14 per cent, respectively, knew the correct management approach entirely.Reference Hakim, Mummadi, Jolly, Dawson and Darr21 We show that healthcare workers were able to reasonably give advice about positioning the patient forward compared with the public, with a statistically significant difference (68 per cent vs 37.9 per cent, p < 0.001). Pinching the nose correctly is essential to provide tamponade to stop the bleeding, yet only 24 per cent of healthcare workers did so correctly. This is a low proportion and is comparable to the 25.2 per cent of the public with no formal medical training (p = 0.87).
Examining different subcategories of healthcare workers reveals some variation in their levels of knowledge on the management of epistaxis. Thirty-five per cent of general practitioners and 30 per cent of emergency department doctors correctly identified the optimal site of nasal pinching, contrasting with only 15 per cent of emergency department and ward nurses. Although not statistically significant, this variation may be explained by the fact that general practitioners and emergency department doctors are often the first responders to epistaxis. Correct head positioning advice also varied between healthcare workers, with 85 per cent of ward doctors but only 50 per cent of general practitioners identifying the correct head position. Despite these findings, the small sample size used to represent each cohort ultimately limits this study and may not be completely representative of true subspecialty knowledge. Likewise, the survey questions on both nasal pinching and head position were both multiple choice, promoting leading amongst the subspecialties surveyed and possibly conflating the results.
Our secondary outcomes yielded interesting results with regard to knowledge about the use of ice as an adjunct treatment. Twenty-eight healthcare workers (28 per cent) compared with five members of the public (4.9 per cent) mentioned any use of ice as an adjunct treatment, which shows that medical staff are more aware of the use of ice. The most widely accepted technique has been to apply ice over the nose.Reference Mulla, Prowse, Sanders and Nix12,Reference Porter, Marais and Tolley14 We found that despite studies demonstrating that ice in the mouth is superior to ice on the nasal dorsum to cause vasoconstriction, this approach was not widely recommended, with only 2 out of 203 of all respondents recommending this specifically.Reference Manjaly, Konieczny and Holland13,Reference Porter15 Careful consideration needs to be given to these findings, given the small sample size and the use of free text in the survey to input answers, which may not accurately capture true knowledge of adjunct treatment use.
• Epistaxis can be a life-threatening condition; proper first aid management techniques and patient education on these methods are imperative
• This study shows that both healthcare workers and the general public lack knowledge on correct first aid management methods
• There was no statistically significant difference between the knowledge of these two groups in multiple domains
• Lack of healthcare worker knowledge indicates ongoing poor epistaxis first aid management methods and dissemination of incorrect methods to patients
• Systemic focused education on first aid management methods is required, targeting frontline healthcare professionals and the general public
This study demonstrates a lack of knowledge in epistaxis management both amongst the public and healthcare workers. Whilst ignorance amongst the public may be expected, a significant lack of healthcare worker knowledge, indistinguishable from that of the general public, can lead to the dissemination and circulation of incorrect management methods. One explanation for this could be the reduced ENT-specific training in undergraduate years for healthcare workers. Recent examination of medical school curricula identified minimal teaching on common ENT presentations, with wide variability between schools.Reference Mayer, Smith and Carrie22 Subsequently, graduates lack confidence with common ENT presentations like epistaxis.Reference Powell, Cooles, Carrie and Paleri23 Our results highlight the need for improved education at a grassroots level to ensure that healthcare workers continue to treat and advise patients correctly on managing this common but potentially life-threatening condition.
Conclusion
Overall, both healthcare workers and the general public lack knowledge of first aid management methods of epistaxis. The findings suggest that, if unaddressed, there remains ongoing poor epistaxis control by patients themselves and subsequent poor management by healthcare workers, leading to an impact on patient quality of life and emergency department attendances. Therefore, systemic focused education on first aid management methods is required, targeting frontline healthcare professionals and the general public alike.
Competing interests
None declared






