



Introduction
Accumulating evidence indicates that more than two-thirds of natural disaster survivors experienced a wide range of mental and physical health consequences at some point in their life. Reference Galea, Nandi and Vlahov1–Reference Gigantesco, Mirante and Granchelli3 The victims of earthquakes who were buried under the rubble undergo tremendous psychological consequences that may result in posttraumatic stress disorder (PTSD). The presence of recurrent, intrusive distressing memories, dreams, dissociative reactions such as flashbacks, and reactions to internal or external cues that symbolize or resemble an aspect of a traumatic event experienced by an individual are features of this mental disturbance. Reference Møller, Meisner, Søgaard, Elklit and Simonsen4 Burial is considered as a risk factor Reference Zhou, Kang and Sun5 for acute stress disorder that can result into chronic PTSD.
Anxiety and pain management should be considered the most important objective during the first rescue maneuvers, especially in case of extrication of buried people from under the rubble.
Among the various options for preventing post-traumatic psychological sequelae, several pharmacological approaches have been investigated. Early repeated injection of sedative agents (SAs) in the acute trauma phase may directly or indirectly interfere with neural processes of memory consolidation of the traumatic event, thus avoiding PTSD.
Early sedation during a natural disaster may influence the neurocognitive processes responsible for the autobiographical memories (AMs) that have been shown to be altered in individuals with PTSD, Reference Rahman and Brown6 even after a long time from the acute phase of trauma.
Nevertheless, more comprehensive studies are required to investigate whether early sedation directly in the disaster setting may promote the prophylaxis and reduce the risk of developing trauma-related disorders (TRDs) on the buried victims of a major natural disaster. Reference Astill Wright, Sijbrandij, Sinnerton, Lewis, Roberts and Bisson7
Thus, this study aimed to analyze the physical and psychological status reported by the buried victims of the earthquake in Amatrice (August 24, 2016; Italy) according to the type of SAs administered during the extrication maneuvers.
Methods
On August 24, 2016, an earthquake measuring 6.2 (SD = 0.016) on the moment magnitude scale hit Central Italy, destroying the city of Amatrice and the nearby villages.
This was an observational study on data from patients directly rescued under the rubble during the earthquake in Amatrice (Italy) on August 24, 2016, as reported in a previous study Reference Blasetti, Petrucci and Cofini8 and approved by Medical Committee for Cave Rescue (MCCR) of Italian National Alpine and Cave Rescue (NACR; Italy) – Protocol ID: 05/01/2017, n.12. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement was respected.
After three years, the survivors treated with SAs during the extrication were contacted by phone by the doctor responsible for the rescue team. After obtaining a verbal consent, survivors were invited to schedule an interview in order to obtain information regarding their health status. Thus, the present research was focused to analyze data regarding physical and psychological health status, while taking into account the type of SAs administrated at moment of extrication (Figure 1). The MCCR was informed and approved.
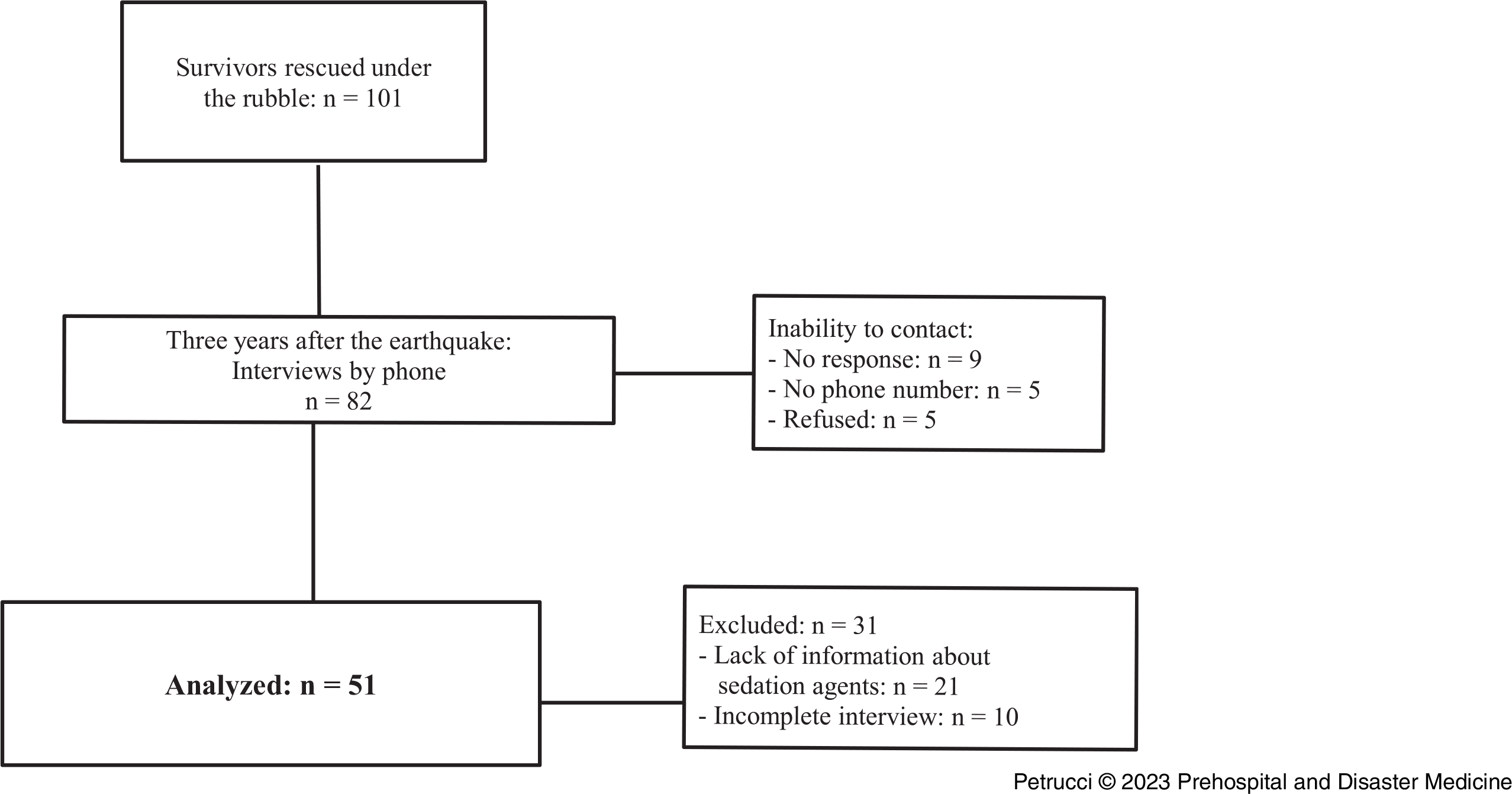
Figure 1. Flow Diagram.
At the time of the disaster, the rescue procedures were managed by the Italian National Civil Defense Service (NCDS; Italy). Italian NACR, as a part of the NCDS, performed specialized technical and medical assistance to those who were buried and trapped under the rubble. The rescue team was the first to arrive in Amatrice and consisted of two anesthesiologists and four nurses. Reference Blasetti, Petrucci and Cofini8 After arrival in the disaster zone, and along with the other rescue workers, the team identified, extricated, and rescued the victims by respecting the disaster and mass-casualty triage. Reference Clarkson and Williams9
During extrication maneuvers, a moderate sedation was achieved in the buried victims by titrating the SAs administration with respect of the Richmond Agitation and Sedation Scale (RASS). Reference Sessler, Gosnell and Grap10 Thus, sedation strategy consisted of repeated injection of ketamine (0.3-0.5mg/kg) Reference Gorlin, Rosenfeld and Ramakrishna11 or morphine (0.1-0.15mg/kg) Reference Aubrun, Maxoit and Riou12,Reference Birnbaum, Esses, Bijur, Holden and Gallagher13 intravenously or via intraosseous access administered. At the moment of the disaster, the rescue team did not have other SAs. Because of the emergency setting, the choice between the two drugs depended on availability at the moment of extrication from the rubble. The bolus of the two SAs was repeated every 30 minutes, or by necessity, to maintain RASS between -2 and -3. The extrication was considered completed when the victim was completely outside from the rubble, and then was recovered in the Advanced Medical Presidium (AMP). The AMP was a medical location similar to an emergency room; it was constituted by a light, pneumatic tent-type structure, provided by NCDS, where medical rescuers operated. Reference Angeletti, Guetti and Papola14
After three years, the survivors were interviewed by phone about their perceived health status and perceived stress with a questionnaire consisting of 17 items:
-
The standard four-item set of healthy days core questions (CDC HRQOL-4); Reference Moriarty, Zack and Kobau15–Reference Gigantesco, D’Argenio, Cofini, Mancini and Minardi17
-
The 12-item General Health Questionnaire (GHQ-12) Reference Piccinelli, Bisoffi, Bon, Cunico and Tansella18 – the perceived stress was analyzed considering moderate stress if the score was from 15 to 20 and pathological stress if the score was >20;
-
And in addition, they were asked if they had a diagnosis for anxiety, depression, and for PTSD by a specialist Reference Hyland, Shevlin, Fyvie and Karatzias19 or other psychiatric problems.
The aims of this study were to analyze: (1) the physical and psychological health status after three years from the earthquake; and (2) the relation between the psychological sequelae reported three years later from the earthquake’s trauma (perceived stress, diagnosis of anxiety, depression, and stress post-trauma) and the type of SAs administrated at moment of extrication.
Statistical Analysis
All data were analyzed and reported as percentages or means with standard deviations (SD).
A logistic regression model was used to analyze data about psychological sequelae reported and their associations with the following factors: age (<65/ ≥65 years), gender (male/female), and type of SAs at moment of the extrication (ketamine/morphine).
The odds ratios (OR) and the relative 95% confidence intervals (95% CI) were reported. All analysis was performed with STATA 14 MP (STATA 14, StataCorp LLC; College Station, Texas USA) and alpha set to 0.05.
Results
One hundred and one (101) victims were rescued under the rubble. This research analyzes data from complete interview and clinical documentations obtained from 51 survivors (Figure 1): 30 were males and 21 females, with a mean age of 52 years. Twenty-six (26) subjects were treated with ketamine, while 25 were treated with morphine, during the extrication procedure. The patients’ characteristics, the burial time under the rubble, and the treatment are reported in Table 1.
Table 1. Patient Characteristics, Burial Time in the Rubble, and Treatment

Abbreviation: SA, sedative agent.
Analyses Three Years after the Earthquake
Concerning the quality-of-life analysis, only 10 survivors out of 51 perceived their health status as good. They reported four unhealthy days (SD = 2), on average, for physical disorders and two (SD = 2) for psychological disorders, on average, over the last month. On average, two days (SD = 2) during the last month reported problems with routine activity. The GHQ-12 scores showed that all survivors had psychological distress (range from 17 to 29), with a mean total score of 22.2 (SD = 3.5). Table 2 reports the differences between subjects with moderate (21/51) and pathological distress (30/51). Males and older survivors reported a higher level of distress, even if there were not significant associations, while there was a significant association between type of distress and type of SAs: among subjects treated with morphine, 20 subjects out of 26 (77%) reported pathological distress, while among subjects treated with ketamine, the pathological distress was reported by 11 out of 25 (44% [OR = 0.23; 95% CI, 0.07-0.79]).
Table 2. Distress Level after Three Years from the Disaster (Univariate Logistic Model)

Abbreviation: SA, sedative agent.
After three years from the earthquake, 18 subjects declared to have had a diagnosis of generalized anxiety (35%), while 29 were treated for depression (57%) and 29 for PTSD (57%) by a specialist. Table 3 reported the psychological disturbances and their associated factors. With regard the anxiety disorder, this analysis showed that it was related to older age (OR = 2.6; 95% CI, 1.00-12.99) and to type of SAs, reporting the better performance of ketamine than morphine: OR = 0.25; 95% CI, 0.07-0.87; P = .025.
Table 3. Psychological Disturbances and Associated Factors (Univariate Logistic Model)
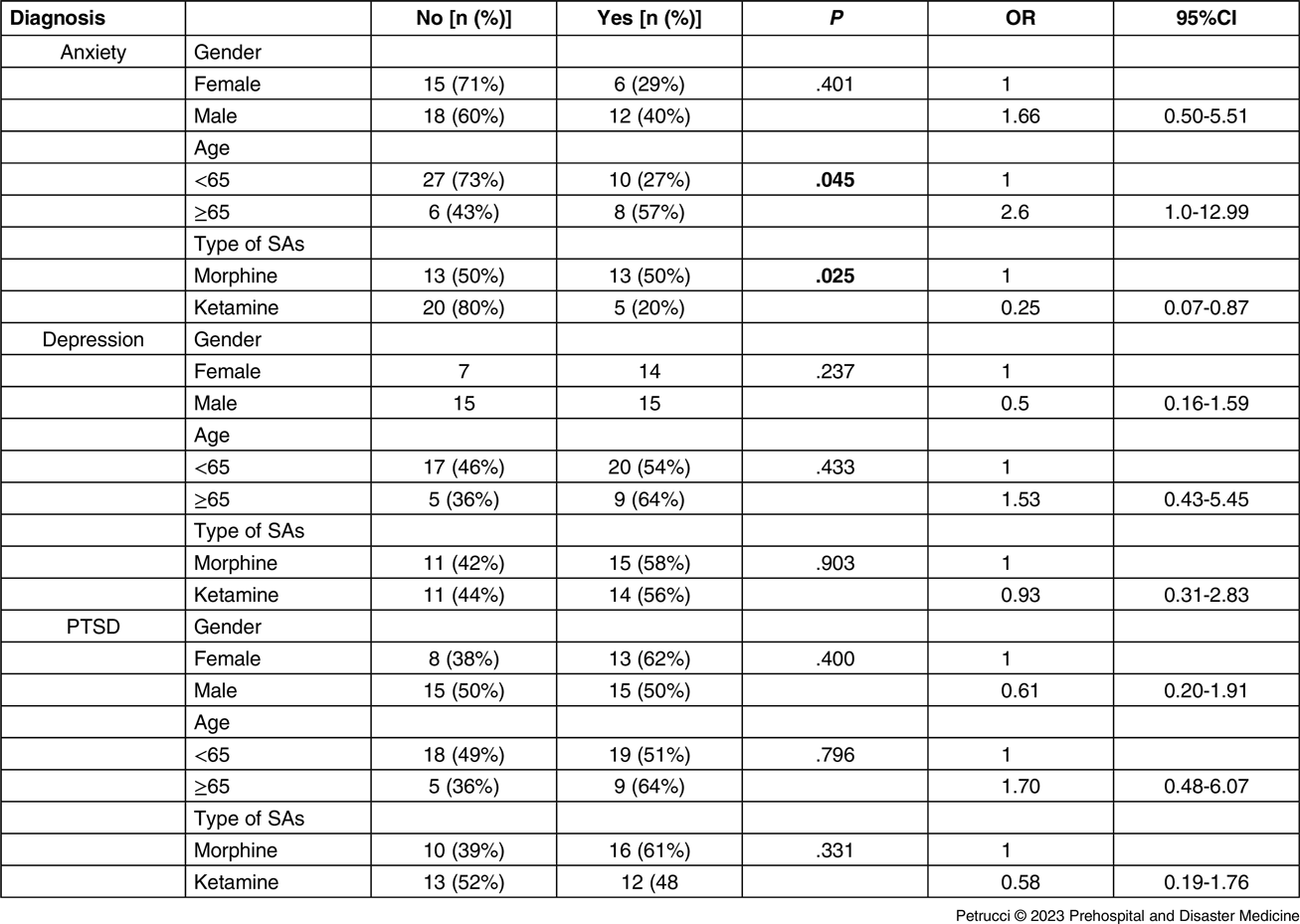
Abbreviations: PTSD, posttraumatic stress disorder; SA, sedative agent.
Discussion
The objective of this study was to investigate the health status of survivors three years following the earthquake of Amatrice (Italy), while taking into account the type of the sedation administered during the extrication phase. The experience of a major natural disaster like an earthquake is one of the worst experiences a human being can be called to endure. The imminent sense of danger of life, the physical constraint under the rubble, and the long wait for help can trigger mental processes with even serious consequences at a distance. Immediately, the goal for rescue is to find survivors, extricate them in the shortest possible time from the rubble, and choose the proper medical treatment based on triage. Importantly, the psychological conditions in which earthquake survivors find themselves must be not underestimated or untreated, even during rescue procedures in the rubble.
Concerning the quality-of-life analysis three years after the earthquake, these data show that only 10 survivors out of 51 perceived their health status as good, while the others suffered from a psychological disturbance with problems during routine activity: they reported four (SD = 2) unhealthy days on average for physical disorders, and two (SD = 2) for psychological disorders in the prior month.
In addition, the GHQ-12 scores showed that all patients had psychological distress (range from 17 to 29) and 31/51 (61%) reported pathological levels of distress.
The analysis showed that the proportion of pathological stressed subjects was higher in subjects treated with morphine (20/31) than those were treated with ketamine (11/31), and the association between distress level and type of sedation agents was significant (P = .016), thus reporting that ketamine could be a protective factor for pathological distress (OR = 0.23; 95% CI, 0.07-0.79).
Another important finding of the study was that 35% of the interviewed (18/51) survivors declared to have had a diagnosis of generalized anxiety and it was found that anxiety was more frequent among oldest survivors (≥65 years) and was related to SAs, showing that the anxiety was reported by 13 subjects treated with morphine and five treated with ketamine (OR = 0.25; 95% CI, 0.07-0.87).
The proportion of diagnoses of depression and PTSD during the period from earthquake and the interview were 57% (29/51) for depression and 55% (28/51) for PTSD, respectively, but the analyses did not show any significant association among investigated factors (gender, age, and type of SAs used).
The possibility to prevent PTSD, anxiety, and depression by using different types of SAs early in the phases of extrication from the rubble still remains a controversy. The administration of SAs during the acute phase of trauma may play an important role in modification of the formation and maintenance of AMs. They are implicated in numerous clinically relevant processes, including problem-solving, the creation of self-concept, and the formation and maintenance of chronic TRDs. Reference Rahman and Brown6 On this basis, it is possible to hypothesize that early administration of SAs may modify the AMs when they are retrieved deliberately (voluntarily) or unexpectedly (involuntarily). Subsequently, the development of TRDs on the buried victims of a major natural disaster can be promoted, even after a long time.
Morphine is a potent opioid analgesic widely used for the treatment of acute pain and for long-term treatment of severe pain. It has suitable analgesic and anxiolytic effects when used for polytrauma patients. Nevertheless, side effects of morphine include hypotension, asystole, bradycardia, and dose-dependent respiratory depression. In case of buried victims with a small pocket air, chest compression or no-free airway by the rubble, morphine may be associated with a worsening of respiratory dynamic with a dangerous survival chance decreasing. Reference Blasetti, Petrucci and Cofini8 In addition, early administration of opioids for pain relief in trapped individuals has been demonstrated to have a negative role in fear memory consolidation, preventing the memory formation of stress via increasing the brain-derived neurotropic factor (BDNF) mRNA in regions like locus coeruleus (LC), medial prefrontal cortex (mPFC), ventral tegmental area (VTA), and amygdala. Reference Nikbakhtzadeh, Borzadaran, Zamani and Shabani20
On the other hand, ketamine is an antagonist of the glutamate N-methyl-D-aspartate (NMDA) receptor that is involved in mediating stress responses and formation of traumatic memories.
It increases blood pressure with some benefit in resuscitating a hypovolemic victim with a possible head injury by increasing cerebral perfusion pressures. However, the increase in intracranial pressure caused by ketamine is of short duration. Reference Ashkenazi, Isakovich, Kluger, Alfici, Kessel and Better21 Furthermore, at sub-anesthetic doses, ketamine is associated with a low incidence of mild psychomimetic symptoms. Caution should be exercised in patients with renal or hepatic damages, which for buried victims cannot be excluded. On the contrary, morphine is a potent analgesic with a suitable sedation effect, but may be associated with worsening of life-threatening hypoxemia, hypercarbia, and acidosis, Reference Blasetti, Petrucci and Cofini8 particularly when survivors have both airway obstruction and impaired ventilation because of the entrapment under the rubble.
Trapped victims can also inhale dusts or noxious gases from the extrication maneuvers or from collapsing buildings with a further airway pulmonary gas exchange impairment due to the lack of ambient oxygen and restriction of chest wall movement. Reference Barbera and Lozano22
It is also important to underline that during a traumatic event, endogenous opioid release helps the individual to endure pain and to not experience emotional sensation, but after several minutes or hours from the event, flashbacks are exaggerated along with intrusive thoughts as a PTSD symptom. Reference Nikbakhtzadeh, Borzadaran, Zamani and Shabani20 Aligned with these premises, this study shows that all survivors after the disaster in Amatrice had psychological distress, perceiving the burial as a devastating experience. It is possible to hypothesize that this experience was probably capable of modifying the neuronal circuits responsible for memory, despite early interventions with SAs aimed not only at facilitating the extrication maneuvers, but also at containing emotional distress and pain. Unfortunately, beneficial emotional effects following the disaster were not obtained, even in the long term. However, although pharmacological prevention seems to have a marginal role, Reference Astill Wright, Sijbrandij, Sinnerton, Lewis, Roberts and Bisson7 it cannot be excluded that interventions carried out during the early phases of rescue may have interfered with the psychological outcome, especially in victims requiring long extrication procedures. In fact, this research suggests that an early administration of SAs maybe influenced the psychological conditions in which earthquake survivors find themselves after the disaster. It is possible to believe that morphine and ketamine may have played an important role in these disorders. Morena, et al demonstrated that ketamine exacerbates acute post-traumatic reaction in rats, possibly leading to development of PTSD symptomatology later in life. Reference Morena, Colucci and Mancini23 In contrast, with regard the perceived distress level and the anxiety disorder, this analysis showed a better performance of ketamine than morphine. Ketamine has emerged as an effective, rapidly acting intervention for patients with treatment-resistant depression when administered at sub-anesthetic doses. Reference Himmelseher and Durieux24–Reference Feder, Parides and Murrough26 For anesthetic aims, ketamine is used at doses of 2mg/kg or more, while sub-anesthetic doses (0.3-0.5mg/kg), alone or in combination with other analgesic drugs, may be considered a suitable choice for pain relief and moderate sedation during extrication from the rubble. The use of this drug can be considered particularly safe because it reliably preserves breathing reflexes, especially in the presence of a small air pocket or a not completely free airway. Reference Blasetti, Petrucci and Cofini8 Moreover, some clinical effects of ketamine, such as the perceptual dissociative symptoms, can be considered useful when much time is spent for the extrication maneuvers. Clinical experience suggests that a bolus dose of 0-3-0.5mg/kg typically does not cause major psychomimetic disturbances. Reference Gorlin, Rosenfeld and Ramakrishna11
With these premises, repeated injections of ketamine in the acute trauma phase may directly or indirectly interfere with neural processes of memory consolidation of the traumatic event, minimizing the formation of maladaptive memories, as a hallmark symptom of PTSD. The scientific evidence underlines that an anesthetic dose of ketamine induces a robust central and peripheral adrenergic/noradrenergic potentiation and that activation of this system is essential for the formation of memory for stressful events and AMs. On the contrary, this study explored the possibility that the neuroprotective effects and anti-inflammatory properties of ketamine can be maximally expressed when it is administered at sub-anesthetic doses, in accordance with Wang’s speculations. Reference Wang, Ye and Chen27 Nonetheless, there is a limited understanding of the accurate mechanism that underlies the potential neuroprotective effects of ketamine. In addition, the NMDA receptor activation plays a central role for the development of central and peripheral neural sensitization, which may contribute to developing PTSD. Furthermore, Park, et al noted that one month after discharge, intensive care unit population reported post-intensive care syndrome after abrupt awakening from sedation by opioids with disorientation and severe stress. Reference Park, Jung and Park28 This may contribute to the development of or increase PTSD. On the contrary, the wearing off of pharmacological effects of ketamine is slow due to its long-acting metabolites.
Ketamine is believed to exert rapid-acting antidepressant (RAAD) effects by inducing a transient surge in post-synaptic glutamate activation leading to upregulation of BDNF and increased synaptic formation. The ketamine’s therapeutic effects extend beyond depression and have been suggested in several stress-related disorders, Reference Abdallah, Averill and Akiki29 showing moderate to large effect size in reducing PTSD symptoms after single infusion. Reference Abdallah, Averill and Akiki29 In accordance, this study showed that an early sedation with ketamine directly during the disaster setting may promote the prophylaxis and reduce the risk of developing TRDs on the buried victims of a major natural disaster, with a better performance than morphine.
The data of this research show that gender and age are important factors influencing the occurrence of the traumatic life event resulting in PTSD. Peterlin, et al Reference Peterlin, Nijjar and Tietjen30 underline that when a traumatic life event occurs at a young age, the risk of major depression is greater than after. Concerning sex differences, there are several potential mechanisms in the association with PTSD or anxiety, including structural changes of subcortical brain regions because of PTSD, as well as genetic influences, and sex differences in the hypothalamic-pituitary-adrenal (HPA) response. Genetics may also play a role in the association between PTSD development and sex, in response to SAs effects. Probably, the BDNF has also been implicated as a mediator of neuronal plasticity, which is important in central sensitization, a key mechanism of PTSD pathophysiology. Reference Abdallah, Averill and Akiki29
Limitations
The propensity to exhibit lasting stress responses is complex and reflects genetics, history of environmental exposures, stage of life, and features of the traumatic stress and post-traumatic social context. These factors were not analyzed in this study, and this represents one of the several limitations affecting the research. In addition, this study investigated health status of patients through phone interview, three years after the earthquake, and data were self-reported. This was related to the fact that survivors left the city of Amatrice and a face-to-face interview was not possible. A follow-up of the victims would have been necessary during the three years from the disaster. This is another drawback of this research. Furthermore, all aspects of the new environment and social context in which the survivors lived after the disaster were not investigated, and data regarding psychological condition, treatments, and clinical history of the victims before the earthquake had to be also collected. Finally, the study design was limited by the lack of the randomization method, the comparison between SAs used, should with further study be evaluated with randomization and controls, even if this aspect is very difficult during a natural disaster.
Conclusions
The extrication from rubble is particularly critical for the survival of the victims of an earthquake. Acting in a timely manner and according to well-structured protocols is mandatory. However, after the acute event, it is often inevitable to have to deal with psychological sequelae of varying severity. What happens in the acute phases of the trauma, but also the management of the rescue phase, likely have a weight that should not be underestimated in the triggering and maintenance of long-term problems. Despite the important limitations, this study suggests that some drugs used in the early extrication phase could affect the outcome. Although these data must be substantiated by robust scientific evidence, they may suggest a preference for potentially less harmful drug strategies for anxiety and pain management during the extrication maneuvers. Preparing procedural sedation protocols for extrinsic maneuvers in maxi-emergencies should therefore be one of the objectives of an advanced rescue team. Further research are needed for evaluating the potential efficacy of these drug-based options, but this study could be a starting point.
Conflicts of interest:
The authors declare none.




