



Introduction
According to the World Health Organization, breast cancer is the most common cancer in women. It is the leading cause of cancer death among females, has a high incidence in developed countries and is on the rise in all regions of the world. 1 According to Thailand data, the National Cancer Institute reported that 31·4% of breast cancer patients in Thailand were diagnosed between 2013 and 2015. It is the most common type of cancer in women. Reference Imsamran, Supaattagorn and Chiawiriyabunya2 Radiation therapy plays a critical role in the treatment of breast cancer. 3
In radiotherapy treatment planning, the area of the lesion must receive the maximum amount of radiation dose with the least amount of radiation dose to nearby organs. Control dose distribution, high radiation areas and dose distribution outside the target are all important considerations. As a result, the advancement of radiotherapy technology aims to improve treatment efficiency while lowering the risk of complications, Reference Mondal and Sharma4,Reference Brown, Mutter and Halyard5 for example, the risk of heart disease in patients receiving radiation treatment for left breast cancer.
A three-dimensional conformity radiotherapy technique was developed. Computed tomography was utilised in radiotherapy treatment planning to assess the distribution of the radiation dose at the target organ and nearby normal organs. The conformity and uniformity of the targeted dose distribution can also be improved by adjusting the number and direction of the radiation beam to avoid exposure to normal tissue. Reference Brownlee, Garg, Listo, Zavitsanos, Wazer and Huber6
Intensity-modulated radiation therapy is an advanced radiotherapy technology. Reference Chan, Tan and Tang7 By adjusting the intensity of each beam to achieve the maximum radiation dose to the target where the nearby organs receive the least amount of radiation dose, the beam is directed in multiple directions to align the radiation dose distribution to the target organ.
However, the use of a large amount of the monitor unit (MU) in intensity-modulated radiotherapy (IMRT) compared to three-dimensional radiotherapy is a limitation. As a result, patients require more time and less radiation exposure due to radiation leakage. This raises the possibility of secondary cancer in the future. Reference Ozyigit and Gultekin8 As a result, the concept of using hybrid radiation technology, which is a combination of three-dimensional radiotherapy and IMRT, has been proposed. This allows the radiation distribution to conform to the target while reducing the low dose received by the patient outside the target. Reference Xie, Ouyang and Wang9 Also, institutes that must accommodate a large number of patients but have limited equipment reduces treatment time to increase the number of patients per day. As a result, the purpose of this research is to identify the suitable breast treatment technique for small facilities and hospitals with limited staff and equipment resources. The benefits and drawbacks of each technique should be considered to help radiation oncologists select the best treatment for breast cancer patients.
Methods and Materials
Patient images acquisition
This was a retrospective study that used a computed tomography scan of 15 patients who had left-sided postmastectomy radiation therapy (PMRT). The patient’s characteristics were classified into two categories: 1. for five patients, only the chest wall (CW) was irradiated, and 2. ten patients had irradiation for their CWs and supraclavicular lymph nodes (SPCs). All of the patients were positioned supine, with both arms on the wing board above their heads. The CT scan was operated from the tip of the shin to the upper abdomen by SIEMENS SOMATOM DEFINITION with 0·5 cm slice thickness. The study was approved by the Research Ethics Committee of the Faculty of Medicine Chiang Mai University No.EXEMPTION 7323/2563.
Delineation of the target and the organ at risk (OAR)
The clinical target volume (CTV) and organ at risk (OAR) including the ipsilateral lung, heart, contralateral lung and contralateral breast were localised by the radiation oncologist as in Figure 1. The planning target volume (PTV) margin was extended 0·5 cm from the CTV to create PTV-CW for the CW-only irradiation group. Regarding the CW plus SPC irradiation, PTV-CW and PTV-SPC are separated by an extended margin of 0·5 cm from the CTV CW and CTV SPC, respectively. The ipsilateral lung and heart were excluded from PTV for both groups.
Dose prescription and treatment planning
By Eclipse treatment planning version 15.6 with AAA algorithm for 6-MV photon beam, all 15 PMRT patients were generated in 4 treatment techniques, including 3DCRT, field-in field (FiF), IMRT and hybrid plans. The PTV-CW and PTV-SPC dose prescriptions were 50 Gy in 25 fractions. The treatment techniques were used to categorise the acceptable criteria. Plans were accepted at 46 Gy (92% of the prescription dose) for 3DCRT and FiF techniques, covering 95% of the PTV, while the maximum dose (Dmax) must be less than 115% of the prescription dose. However, IMRT plans at 47·5 Gy (95% of prescription dose) covered 95% of the PTV, while the Dmax must be less than 55 Gy and the Dmin must be greater than 47·5 Gy. Acceptable criteria for OARs were 8 Gy for mean heart dose and 20% for both lung volumes receiving less than 20 Gy (V20% < 20 Gy).
The following are the treatment plans for 15 patients as in Figure 2.
Three-dimensional conformal radiotherapy (3DCRT)
A 0·5-cm bolus thickness was used for an adequate skin dose in fractions 13th–25th. The treatment field size must open and cover the PTV-CW with a 2–3 cm margin expansion to account for movement of the CWl due to breathing, while a multileaf collimator (MLC) was used to block the heart and lung area to reduce the amount of radiation dose. To adjust the uniform dose distribution, wedge beams were used. The weighting of the medial and lateral tangential beams is then adjusted to ensure that the dose distribution covers the target volume. The one anteroposterior (AP) beam direction was used for PTV-SPC, and MLC defined the treatment field conformed to PTV-SPC.
Field-in-Field (FiF)
The beam directions were placed the same in the 3DCRT technique. However, the 2–4 subfields were created manually by using MLC to reduce high-dose regions.
Intensity-modulated radiation therapy (IMRT)
The dynamic IMRT with static nine gantry angle was used (15, 35, 55, 80, 100, 120, 300, 315 and 340). For optimisation, this technique used inversed planning with the Eclipse treatment planning system.
Hybrid plans
This technique combines 3DCRT and IMRT, with 3DCRT 60% (120cGy/Fraction) and IMRT 40% (80cGy/Fraction) used. Both 3DCRT and IMRT used the same beam direction as the 3DCRT and IMRT techniques.
Plan evaluation and statistical analysis
The dose volume histogram was generated for all PTV and organs at risk. The dosimetric results for each treatment technique were compared using the following quantities: target coverage by V95%, D2% and D98%, and the conformity index (CI) as proposed by Paddick et al. was defined as follows: Reference Paddick10
 $${\rm{CI}} = {{\rm{V}} _ {95{\rm{\%}}} \over{{{\rm{PTV}}}}} \times {{\rm{V}} _ {95{\rm{\%}}} \over{{{\rm{PIV}}}}}$$
$${\rm{CI}} = {{\rm{V}} _ {95{\rm{\%}}} \over{{{\rm{PTV}}}}} \times {{\rm{V}} _ {95{\rm{\%}}} \over{{{\rm{PIV}}}}}$$
where V95% refers to the volume of PTV received 95% of the prescription dose (47.5 Gy), PTV refers to the volume of the PTV, and PIV refers to the volume of PTV received 95% of the prescription dose (47.5 Gy).
The homogeneity index (HI) was defined as:
 $${\rm{HI}} = {{{{\rm{D}}2{\rm{\% }} - {\rm{D}}98{\rm{\% }}}}\over{{{\rm{D}}50{\rm{\% }}}}}$$
$${\rm{HI}} = {{{{\rm{D}}2{\rm{\% }} - {\rm{D}}98{\rm{\% }}}}\over{{{\rm{D}}50{\rm{\% }}}}}$$
where D2%, D50% and D98% refer to doses of 2%, 50% and 80% volume of PTV.
For all four treatment techniques, the dose distribution for OARs including the heart, ipsilateral lung, contralateral lung, contralateral breast and both lungs was compared. SPSS, version 28.0, was used for all statistical analyses. On each technique of comparison metrics, the one-way analysis of variance (ANOVA) test and the paired sample t-test were used to determine statistical significance with p-values of 0·05.
The plan quality score was calculated by adding the scores of each parameter in each technique, which were defined as ‘0,’ ‘1’ and “2" when the obtained p-values from the one-way ANOVA test were greater than 0·05, < 0·05 and < 0·001, respectively, and then comparing the sums with the highest one.
Results
PTV dosimetric comparison
As shown in Figure 3, the dosimetric comparison for 3DCRT, FiF, IMRT and hybrid techniques of CW-only irradiation and CW plus SPC irradiation revealed the differences among four techniques for the V95%, D2% and D98% for PTV. Where both groups produced identical results. 3DCRT plans with V95% and V98% were significantly lower than the other three groups. By a statistically significant margin, the V95% of IMRT plans outperformed 3DCRT and FiF plans. However, IMRT plans exhibited target coverage similarities with hybrid plans. The hot spot region in D2% of the 3DCRT plan was significantly higher than the other three groups, whereas the mean dose of PTV for the four plans did not differ.

Figure 1. Target and OAR delineation for two groups of patients. A. Chest wall only irradiation. B. Chest wall and SPC irradiation.
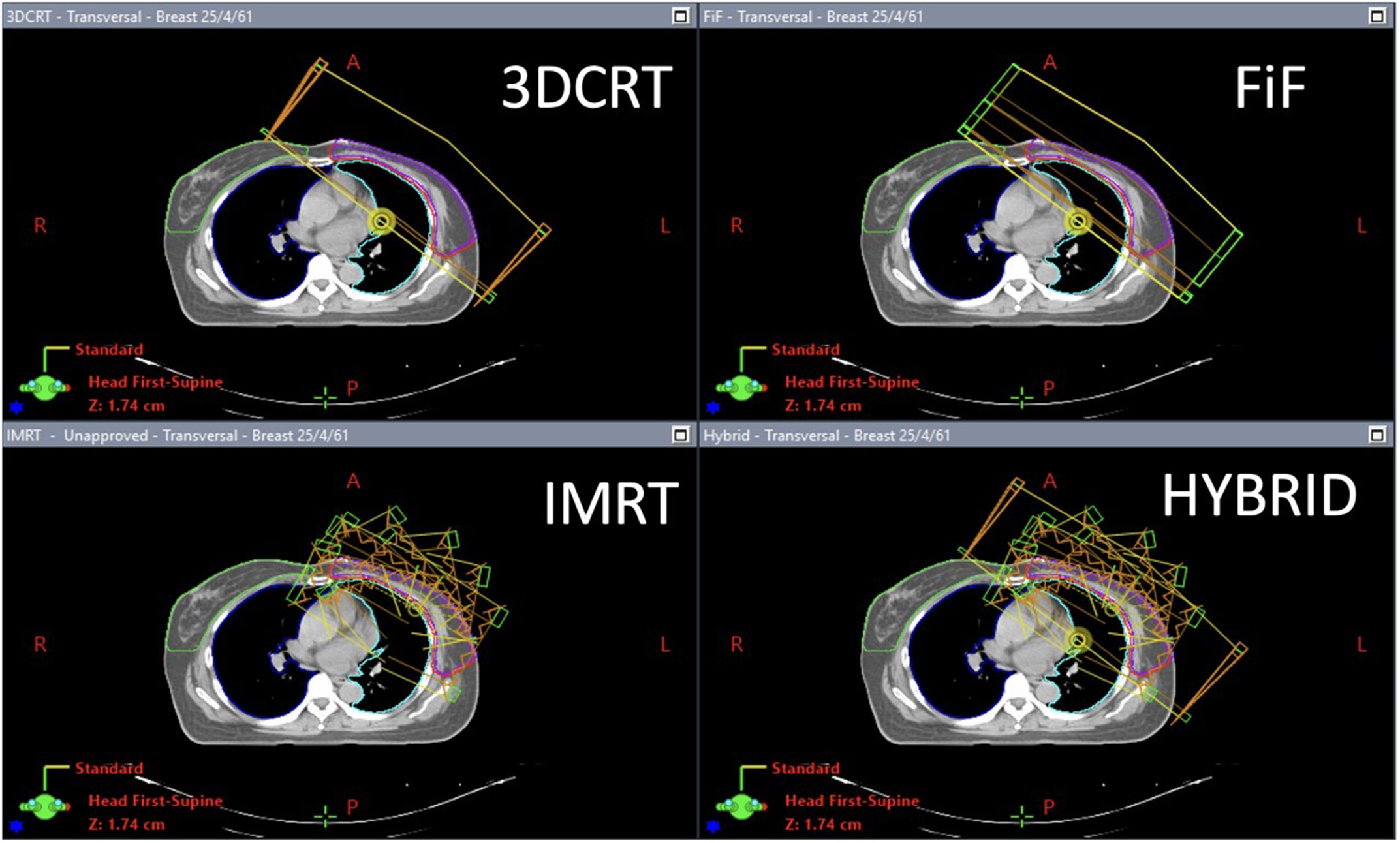
Figure 2. Field alignment in the transverse plane (3DCRT: three-dimensional conformal radiotherapy technique; FiF: field-in-field technique; IMRT: intensity-modulated radiotherapy technique; hybrid: hybrid technique).

Figure 3. Dose distribution of each of the four treatment plans. A. Chest wall-only irradiation. B Chest wall and SPC irradiation. (3DCRT: three-dimensional conformal radiotherapy technique; FiF: field-in-field technique; IMRT: intensity-modulated radiotherapy technique; hybrid: hybrid technique).
The IMRT plan performed significantly better than the other three plans for CI and HI by significant differences with 3DCRT and FiF, while IMRT performed similarly to hybrid plans for conformity and homogeneity parameters by not significant differences in CI and HI, as shown in Table 1.
Table 1. The dose statistic, dose conformity and homogeneity parameters for target in four treatment techniques

3DCRT: three-dimensional conformal radiotherapy technique; FiF: field-in-field technique; IMRT: intensity-modulated radiotherapy technique; hybrid: hybrid technique; PTV: planing target volume; V95%: volume of PTV were received 95% of prescribe dose; D98% and D2%: doses of 98% and 2% volume of PTV; Dmean; mean dose of PTV; HI: homogeneity index; CI: conformity index.
Notes: a Had significant difference between 3DCRT and FiF (p < 0·05).
b Had significant difference between 3DCRT and IMRT (p < 0·05).
c Had significant difference between 3DCRT and hybrid.(p < 0·05).
d Had significant difference between FiF and IMRT (p < 0·05).
e Had significant difference between FiF and hybrid (p < 0·05).
f Had significant difference between IMRT and hybrid (p < 0·05).
OAR dosimetric comparison
Heart
In both patient groups, CW-only irradiation and CW plus SPC irradiation had similar outcomes. The 3DCRT and FiF techniques demonstrated better heart sparing by lowering the mean heart dose, with statistically significant differences between the four techniques. The mean heart dose was similar in the IMRT and hybrid plans. However, as shown in Table 2, IMRT and hybrid showed significantly lower volume when receiving high doses of 30 or 40 Gy.
Table 2. The dose statistic for organ at risk in four treatment techniques
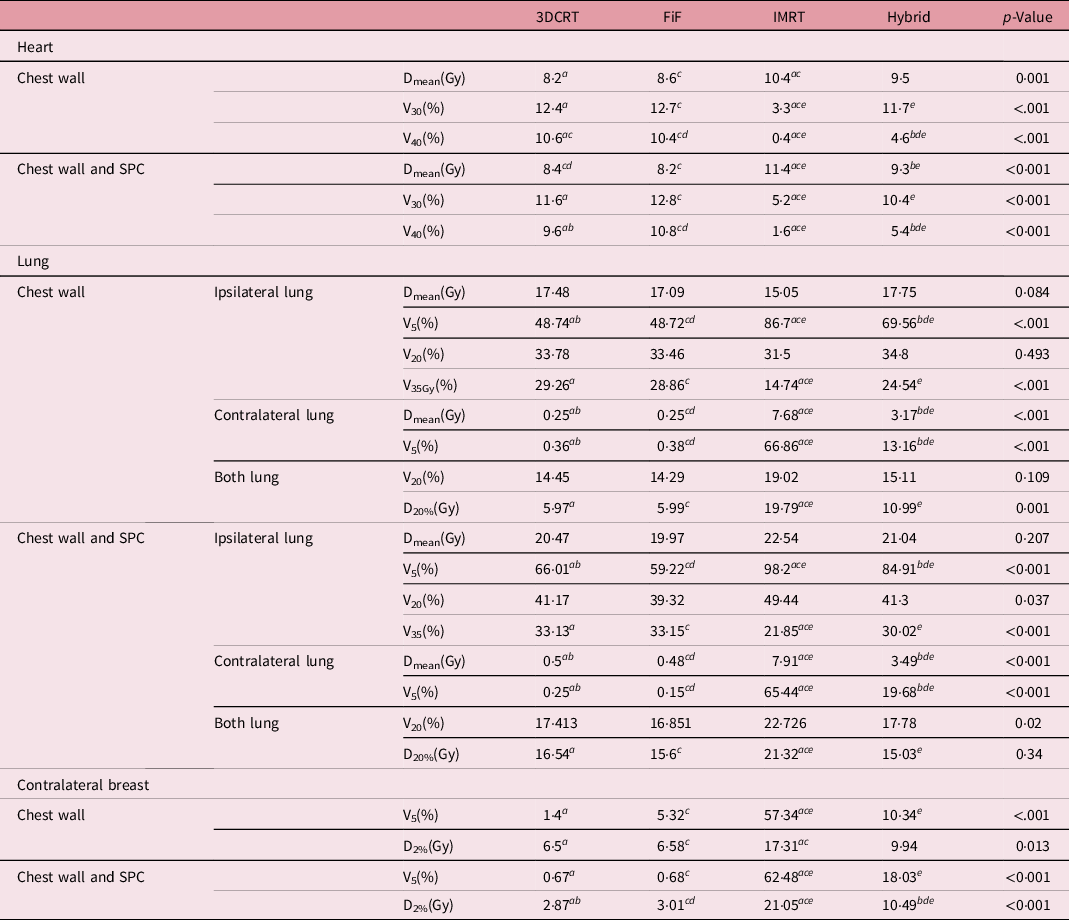
Dmean; mean dose of OAR; V5, V20, V30, and V40: volume of OAR was recipes dose 5 Gys, 20 Gys, 30 Gys, and 40Gys; D20% and D2%: doses of 20% and 2% volume of OAR.
Notes: a Had significant difference between 3DCRT and IMRT (p < 0·05).
b Had significant difference between 3DCRT and hybrid·(p < 0·05).
c Had significant difference between FiF and IMRT (p < 0·05).
d Had significant difference between FiF and hybrid.(p < 0·05).
e Had significant difference between IMRT and hybrid.(p < 0·05).
Lung
The mean dose and V20Gy of the ipsilateral lung did not differ between the four techniques. Low-dose volume (V5Gy) of the ipsilateral and contralateral lung can be reduced using 3DCRT and FiF techniques. When compared to 3DCRT and FiF plans, IMRT and hybrid revealed significantly higher low-dose spreading for V5Gy. However, the IMRT technique can reduce the ipsilateral lung’s high-dose volume.
Contralateral breast
The low dose of contralateral breast showed the largest volume in IMRT plans. Furthermore, the maximum dose (D2%) of the IMRT plan was significantly higher than the 3DCRT plan and FiF plan for both patient groups.
Treatment time
Table 3 shows that the IMRT plans provided the longest treatment time, which was found to be statistically significant. However, the IMRT and hybrid plans had comparable irradiation times.
Table 3. The treatment time in four treatment techniques

Notes: a Had significant difference between 3DCRT and IMRT (p < 0·05).
b Had significant difference between 3DCRT and hybrid.(p < 0·05).
c Had significant difference between FiF and IMRT (p < 0·05).
d Had significant difference between FiF and hybrid.(p < 0·05).
Table 4. The plan quality scores for four treatment techniques

3DCRT: three-dimensional conformal radiotherapy technique; FiF: field-in-field technique; IMRT: intensity-modulated radiotherapy technique; hybrid: hybrid technique.
Plan quality scores
When dosimetric parameters and treatment time of 3DCRT, FiF, IMRT and hybrid techniques were considered, the summation scores of CW-only irradiation were 22, 23, 29 and 15 as in Table 4, respectively. The scores (22, 28, 29 and 18) showed concordant results with the group of CW plus SPC irradiation; the results with the highest score demonstrated the superiority of the IMRT plan in dosimetric parameters but inferiority in treatment time.
Discussion
The dosimetric parameters of four techniques for left-sided PMRT were compared in this study. The conformity number was superior in IMRT, hybrid, FiF and 3DCRT, respectively. The conformity revealed the same trend in two patient groups, CW alone and CW plus SPC. This result was consistent with Xiaoxue Xie et al. Reference Xie, Ouyang and Wang9 and Hua Zheng et al. Reference Hua, You-Qun and Yuan11 , who found that IMRT had the highest conformation number when compared to 3DCRT and hybrid plans. Furthermore, the homogeneity parameter of IMRT plans had the highest value, which was consistent with Fuli Zhang et al. Reference Fuli, Yadi and Weidong12 and Guang-Hua Jin et al. Reference Guang-Hua, Li-Xin and Xiao-Wu13 . The dose for OAR, on the other hand, resulted in superiority dose sparing in 3DCRT for the heart, lung and contralateral breast, which was consistent with Hua Zheng et al. Reference Hua, You-Qun and Yuan11 as well as Serhat et al. Reference Aras, İkizceli and Aktan14
Treatment time is an important factor for small clinics that serve a large number of patients per day with limited staff and equipment. Although IMRT outperformed in terms of dosimetry parameters, it had the longest treatment time. FiF will be the appropriate technique for PMRT treatment of CW and CW + SPC based on the plan quality scores due to OAR sparing and short treatment time.
Conclusion
The IMRT plan had the highest plan quality but required the most time to treat. In a small facility centre with limited equipment, treatment times are critical. As a result, the FiF plan was found to be the best technique for both CW-only and CW plus SPC irradiation due to its short treatment time and highest plan quality scores for OAR dose sparing.







