Introduction
Adverse life events
Although no standard definition of an adverse life event exists, various descriptions have been offered. “Adverse”, “traumatic”, or “negative” life events represent sudden, dramatic experiences (Suh et al., Reference Suh, Diener and Fujita1996) that have the potential to significantly alter one’s social world (Wheaton, Reference Wheaton, Avison and Gotlib1994). They are typically unexpected, rather than universal, age-graded transitions (Rutter, Reference Rutter1996), and require a significant change in an individual’s life pattern and adaptive or coping behavior (Holmes and Rahe, Reference Holmes and Rahe1967). Elsewhere, they are referred to as “potentially traumatic events” due to their associations with post-traumatic stress disorder (PTSD). These are variously defined as events entailing any actual or perceived threat to the life or physical safety of the individual, their loved ones or those around them (American Psychiatric Association, 1994), or to individuals’ physical or psychological wellbeing (Australian Psychological Society, 2019).
Earlier studies observed that individuals with depression and other conditions are more likely to have experiences of adverse life events than those without (Brown et al., Reference Brown, Sklair, Harris and Birley1973; Brown and Harris, Reference Brown and Harris1978; Paykel, Reference Paykel1978). These studies typically found associations between events and onset of conditions occurred over relatively short time spans (i.e. less than one year) (Suh et al., Reference Suh, Diener and Fujita1996; Brown et al., Reference Brown, Sklair, Harris and Birley1973). Later work, however, has highlighted the potential for major events to represent “turning points” which cause lasting shifts in individuals’ developmental and life trajectories (Rutter, Reference Rutter1996), and investigated associations between specific adverse life events individually and later-life mental health outcomes. For example, abuse and interpersonal loss in childhood have been associated with various mental health conditions over the life course including mood disorders and anxiety (Green et al., Reference Green2010). Childhood sexual abuse in particular has been shown to predict depression and lower wellbeing in adulthood (Kamiya et al., Reference Kamiya, Timonen and Kenny2016).
Timing of adverse events
According to Elder’s principles of life course theory (Elder, Reference Elder1998), the developmental impact of specific life events may be contingent on when they occur in a person’s life (Rutter, Reference Rutter1996). Although some studies have found that more recent events are of greater importance (Suh et al., Reference Suh, Diener and Fujita1996), associations between adverse events and mental health outcomes have been shown to persist for long periods after their occurrence, including from childhood to later life (Green et al., Reference Green2010; Kessler and Magee, Reference Kessler and Magee1993).
Self- and other-orientation of adverse events
Another principle of life course theory is that of “linked lives”, in which consequences of stressors or adverse events are shared through social relationships (most notably parent–child relationships) (Elder, Reference Elder1998). Adverse events may be experienced directly by individuals or indirectly through knowledge of experiences of other people. In contrast with previous editions, the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) offered a wider definition of traumatic events to make a distinction between events which involve an injury or threat to the physical or psychological integrity of either the self or of others (American Psychiatric Association, 1994). Some studies have considered this distinction (Breslau et al., Reference Breslau, Chilcoat, Kessler and Davis1999; Shmotkin and Litwin, Reference Shmotkin and Litwin2009; Green et al., Reference Green2010; Palgi et al., Reference Palgi, Shrira, Ben-Ezra, Shiovitz-Ezra and Ayalon2012; Ogle et al., Reference Ogle, Rubin and Siegler2014). This concept is similar to that of “egocentric” and “non-egocentric” stress proposed by Aldwin (Reference Aldwin, Stephens, Crowther, Hobfoll and Tennenbaum1990) within the context of families. Parallels have also been drawn between mental health outcomes following experiences of other-oriented adverse events and phenomena such as “compassion fatigue” and “vicarious” or “secondary” traumatization. These terms describe symptoms of exhaustion, hypervigilance, and avoidance experienced by professionals working with, and family members of, people with PTSD (Baird and Kracen, Reference Baird and Kracen2006).
The only studies to disaggregate counts of events according to self- or other-orientation found associations between experiences of other-oriented adversity in early-life and positive later-life mental health outcomes and between self-oriented events in adulthood and adverse mental health outcomes (Shmotkin and Litwin, Reference Shmotkin and Litwin2009; Shrira et al., Reference Shrira, Shmotkin and Litwin2012).
Life course models of risk: timing and accumulation of exposures
Different models have been proposed to describe associations between potentially harmful exposures over the life course and later-life functioning, wellbeing, or mental health. Latency factors, or “programming effects”, exert lasting influences throughout the subsequent life course. A critical period represents a limited window in which a given exposure can impair subsequent development and later-life outcomes (Ben-Shlomo and Kuh, Reference Ben-Shlomo and Kuh2002), whereas events in a sensitive period have a more pronounced effect than the same exposure in a different period. Timing of these sensitive and critical periods, which need not only occur in childhood (Krause et al., Reference Krause, Shaw and Cairney2004), depends on both the exposure and outcome of interest (Cohen et al., Reference Cohen, Janicki-Deverts, Chen and Matthews2010).
The accumulation-of-risk model, based on the concept of “insult accumulation” (Riley, Reference Riley1989), conceives the association between such exposures and later-life outcomes as a lifelong dose–response relationship (Cohen et al., Reference Cohen, Janicki-Deverts, Chen and Matthews2010). Damage accrues over the life course as the number, duration, and severity of exposures to adversity increases, and as compensatory systems lose efficacy over time (Kuh et al., Reference Kuh, Ben-Shlomo, Lynch, Hallqvist and Power2003). Various studies have highlighted additive accumulation of exposure to adverse events as important for later-life wellbeing and mental health (Turner and Lloyd, Reference Turner and Lloyd1995; Krause, Reference Krause2004; Kessler et al., Reference Kessler2010).
Objectives and hypotheses
As greater numbers of people in developed economies approach later life, the determinants of their mental health and wellbeing will assume ever greater importance. The aim of this study was to investigate how different types of adverse events, and their timing, influence how they may affect later life wellbeing and mental health. Its specific objectives were to investigate associations between counts of adverse events over the life course and wellbeing and mental health outcomes in older people, and to assess the extent to which these associations depended on: (i) their timing (age of occurrence), (ii) their orientation (self or other), and (iii) both their timing and orientation.
Based on previous studies, we hypothesized that cumulative experiences of adverse events over the life course would be associated with lower wellbeing and higher odds of depression in later life. Second, we hypothesized that adverse events occurring at all ages would be associated with negative outcomes, with more recent events (at later ages) potentially showing a stronger association. Finally, we hypothesized that both self- and other-oriented events would be associated with lower wellbeing and higher odds of depression. In regard to both orientation and timing, the results of Shrira et al. (Reference Shrira, Shmotkin and Litwin2012) would suggest that exposures to other-oriented adverse events, particularly in early life, are associated with higher wellbeing and positive mental health outcomes in older people while self-oriented events in adulthood are associated with lower wellbeing and worse mental health outcomes.
Methods
Analytic sample
Data were drawn from Waves 1–7 (2002/2003–2014/2015) of the English Longitudinal Study of Ageing (ELSA), a nationally representative sample of older people (aged 50 and over) living in private households in England (Steptoe et al., Reference Steptoe, Breeze, Banks and Nazroo2013). Ethical approval for ELSA data collection was granted by the London Multicentre Research Ethics Committee (MREC/01/2/91), informed consent was obtained from all participants, and all observations were anonymized. No specific approval was required for this study as it was based on secondary data analysis.
We restricted our analysis to respondents who participated in the Life History Module in Wave 3 (2006–2007), who were 50–90 years at any wave, had provided complete information on age of occurrence of all adverse events investigated and had no missing covariate data in at least one wave.
Wellbeing and mental health outcomes
Outcomes included two measures of wellbeing (CASP-12 and life satisfaction) and one of mental health (depressive symptomatology). The CASP-12 (control, autonomy, self-realization, and pleasure) scale (see Appendix A1, published as supplementary material online attached to the electronic version of this paper), available in ELSA Waves 1–7, was developed for individuals in later life and provides a global assessment of multiple domains encompassing hedonic and eudemonic aspects of wellbeing (Hyde et al., Reference Hyde, Wiggins, Higgs and Blane2003).
Probable depression was measured using the eight-item Centre of Epidemiological Studies Depression Scale (CES-D), a screening test for depression and depressive disorder based on the number of depressive symptoms. It has been shown to be a reliable, validated tool with high internal consistency, acceptable test-retest stability, high generalizability across population subgroups, excellent concurrent validity by clinical and self-report criteria, and substantial evidence of construct validity (Radloff, Reference Radloff1977). Scores were calculated by summing the number of self-reported symptoms occurring within the past week (range: 0–8) (see Appendix A2). A score of three or more was used to define probable depressive caseness (Turvey et al., Reference Turvey, Wallace and Herzog1999), as recommended in previous studies (Courtin et al., Reference Courtin, Knapp, Grundy and Avendano-Pabon2015; White et al., Reference White2016). CES-D measures were available from Waves 1–7 of ELSA and were expressed as binary outcomes (probable caseness/non-caseness).
Self-appraisals of subjective life satisfaction were assessed in Waves 2–7 and operationalized using a seven-point Likert scale with higher values indicating higher life satisfaction (see Appendix A3).
Adverse life events
Retrospective information on types of adverse events experienced and their age of first occurrence was collected in the Wave 3 Life History Module. This module comprised the Life History Interview, which included questions on relationships and family, housing, mobility and work history, and the Life History Self-Completion Questionnaire, which covered quality of parental care during childhood and adverse life events. Sixteen types of adverse event were identified (based on Breslau et al., Reference Breslau, Kessler, Chilcoat, Schultz, Davis and Andreski1998). Two (maternal separation and parental divorce) were drawn from the interview while all other items were assessed in the self-completion questionnaire. Six items were specific to childhood (ages 0–15 years) while the remaining 10 could occur at any age (0–49 years). Events were categorized according to whether they were self- or other-oriented using the same approach as in previous work (Shmotkin and Litwin, Reference Shmotkin and Litwin2009; Shrira et al., Reference Shrira, Shmotkin and Litwin2012). All events occurred before the first wave in which a respondent was included in ELSA and had full information on at least one of the three outcomes investigated. From these 16 event items, two count variables for exposure to self- and other-oriented events were derived by summing the number of event types in which the primary harm was to the self and in which the primary harm was to another individual, respectively. Both variables had ranges of 0–8.
Covariates
Covariates were conceptualized as potential confounders for relationships between life course events and later-life outcomes. We operationalized physical frailty based on accumulation of deficits using items relating to medically diagnosed conditions, medical symptoms, functional activities, and activities in daily living (Searle et al., Reference Searle, Mitnitski, Gahbauer, Gill and Rockwood2008) (see Appendix A4). The resulting scale included 36 items and was scaled as a continuous variable from 0 to 1. Models were further adjusted for gender, current self-reported labor market status (retired/in paid employment/unemployed/permanently sick or disabled/looking after the home or other), housing tenure (outright ownership/ownership with mortgage/renting or other), participation in social activities within the previous month (yes/no) (see Appendix A5), birth outside the United Kingdom (yes/no), partnership status (in a marriage or other partnership/non-partnered), household wealth, and gross household income. Respondents were categorized by quintile of equivalized non-pension household net wealth. Household income was transformed taking the natural logarithm to reduce this skewness and normalize its distribution (Office for National Statistics, 2016) and was equivalized to account for differences in household size by dividing by the square root of the number of household members. Financial variables were inflation-adjusted using annual consumer price index inflation terms for all consumer items, obtained from the OECD Prices and Purchasing Power Parities database (Organisation for Economic Co-operation and Development, 2019), and expressed in 2011 £. Please see Richardson et al. (Reference Richardson, Carr, Netuveli and Sacker2018) for further details on specification of these variables in ELSA.
Occupational position was measured using the five-category National Statistics Socio-economic Classification (NS-SEC) groupings (Office for National Statistics, 2000) based on respondents’ current occupation or last-known occupation if no longer in employment. A final sixth category was included for respondents who had never worked. All covariates except for birth abroad and occupational position were taken at the time of interview for each observation.
Descriptive analysis
We calculated summary statistics, including mean, standard deviation (SD), skewness, and internal consistency (Cronbach’s α) as appropriate, for each of the three outcome variables for respondents in Wave 3 with complete data adverse events and control variables.
We then estimated weighted proportions of respondents in the ELSA Wave 3 Life History Module with complete information on adverse events and age of occurrence who had experienced each adverse event type by age 16 and by age 50 years. We then plotted the weighted cumulative proportions of respondents who had experienced each event by age. Cross-sectional probability weights were used to ensure representativeness of the English population (Steptoe et al., Reference Steptoe, Breeze, Banks and Nazroo2013).
Statistical analysis
Continuous outcomes (CASP-12 and life satisfaction) were analyzed with linear random-effects models to reflect the repeated measures of individuals across waves. Logistic random-effects models were fitted for the binary outcome (CES-D). All models were fully adjusted for all covariates listed above, and analyses were performed using Stata 14 (StataCorp, 2015) (for more information on model specification and selection of model covariates, and discussion of potential mediation of the primary associations tested by model covariates, see Appendix A6). Variance inflation factors were calculated to test for multicollinearity between model covariates (see Appendix A7).
Models were fitted corresponding to different assessments of adverse events, operationalized as count variables. First, the association between the total number of events and each outcome measure was tested (Model A). Four fully adjusted models (Models B–E) were fitted for each outcome with adverse events disaggregated according to their timing (within different age ranges representing different life course stages: see Galobardes et al., Reference Galobardes, Shaw, Lawlor, Lynch and Davey Smith2006; Galobardes et al., Reference Galobardes, Lynch and Smith2007) and orientation (self or other). Models were specified with the following mutually adjusted exposure measures:
-
Model A: Total adverse events at all ages (0–49 years)
-
Model B (events by age of occurrence): Adverse events in early childhood (0–5 years), adverse events in childhood late childhood (6–15 years), adverse events in early adulthood (16–30 years), and adverse events in late adulthood (31–49 years)
-
Model C (events by orientation): Self-oriented events at all ages (0–49 years) and other-oriented events at all ages (0–49 years)
-
Model D (events by age of occurrence and orientation): Self-oriented events in childhood (0–15 years), self-oriented events in adulthood (16–49 years), other-oriented events in childhood (0–15 years), and other-oriented events in adulthood (16–49 years)
-
Model E (events by age of occurrence and orientation): Self-oriented events in early childhood (0–5 years), late childhood (6–15 years), early adulthood (16–30 years), and late adulthood (31–49 years), and other-oriented events in early childhood (0–5 years), late childhood (6–15 years), early adulthood (16–30 years), and late adulthood (31–49 years).
We considered whether experiences of adverse events influenced trajectories of wellbeing from age 50 to 90 and operationalized latent growth curve models within a multilevel framework for each of the three outcomes, with age fitted as a random effect and interacted with counts of total adverse events experienced (0–49 years).
Sensitivity analyses
We conducted three sensitivity analyses (see Appendices A8, A9, and A10). First, we tested the association between total adverse events experienced (0–49 years) and depression outcomes when the latter was operationalized as a count of symptoms (as opposed to a dichotomous variable). Second, we attempted to provide evidence against potential reverse causation between depressive caseness and reporting of adverse events in the same wave (Ross, Reference Ross1989; Shrira et al., Reference Shrira, Shmotkin and Litwin2012), for example, due to potential overreporting of adverse events among those with depressive symptoms, by restricting the analysis of depression caseness outcomes to respondents who were not identified as having depressive caseness in Wave 3 and using data from Waves 1–2 and 4–7 only. Third, we tested the association between adverse events experienced (disaggregated by age of occurrence and orientation) and the number of waves in which respondents were identified as having depressive caseness (Waves 1–7).
Results
Analytic sample
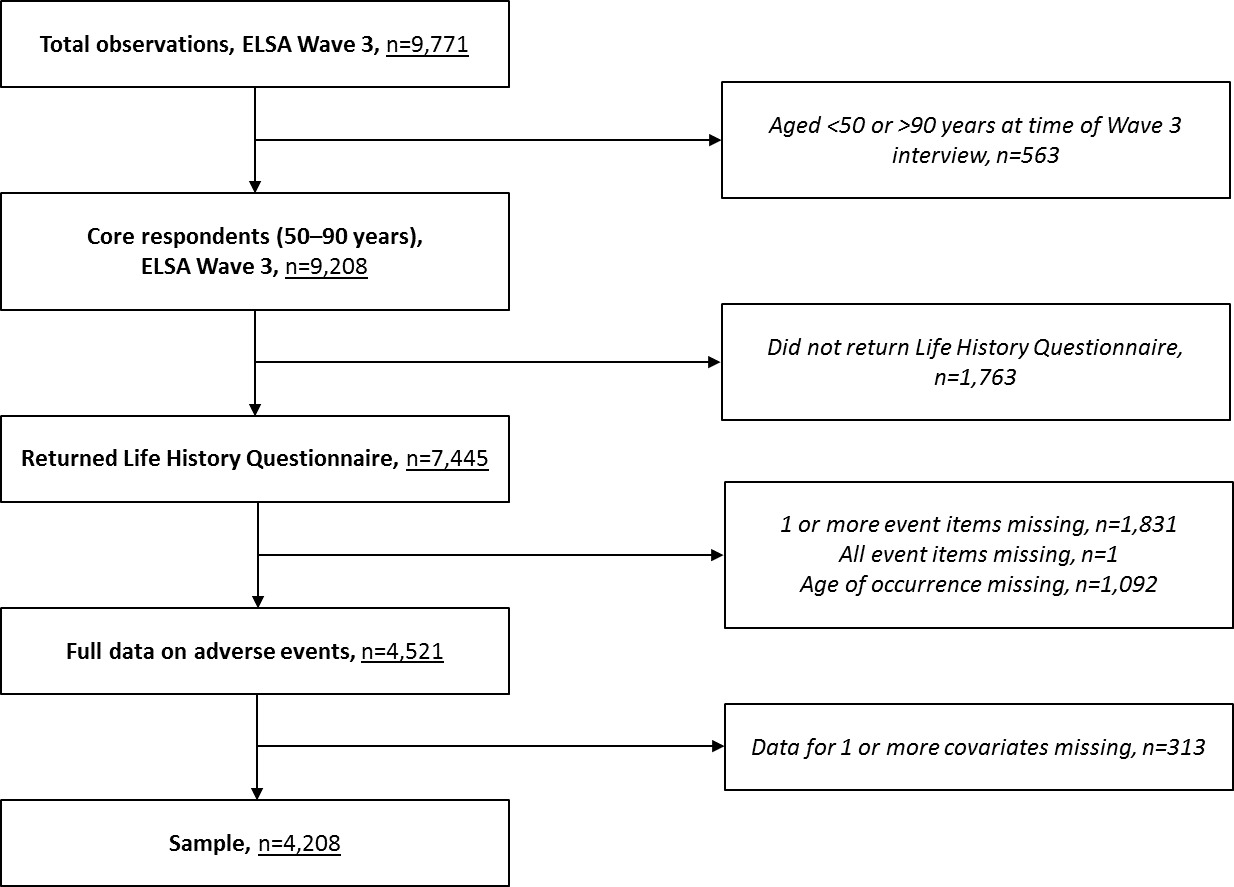
A total of 9,771 respondents participated in ELSA Wave 3, of which 9,208 were aged 50–90 years. Of these, 7,445 participated in both the Wave 3 Life History Interview and returned the self-completion questionnaire, and 4,521 provided complete data on all 16 events and the age of occurrence. Our analysis included data from 4,208 unique individuals with at least one observation with no missing covariate information over Waves 1–7 (see Figure S1, published as supplementary material online attached to the electronic version of this paper).
Separate analytic samples were identified for each outcome measure after dropping observations with missing outcome values. The analytic sample for CASP-12 outcomes included 4,176 unique individuals with 20,176 observations over Waves 1–7. Samples for depressive caseness and life satisfaction outcomes included 4,208 respondents with 22,039 observations over Waves 1–7 and 4,152 respondents with 17,948 observations over Waves 2–7, respectively.
Descriptive analysis
Summary statistics for CASP-12, probable depressive caseness, and life satisfaction were calculated for Wave 3 respondents with complete data on adverse events and covariates (sample n = 3,159, 3,450, and 3,243, respectively). The mean CASP-12 score on a range of 12–48 was 38.04 (SD: 5.56). The distribution of CASP-12 scores was relatively symmetrical with a slight negative skew (skewness: −0.71). Internal consistency of the 12 scale items was good (Cronbach’s α: 0.842). Prevalence of depressive caseness was 18.14% (95% CI: 16.86–19.43%) of the Wave 3 sample. Internal consistency of the eight-item CES-D scale, with scores representing number of symptoms present, was also good (Cronbach’s α: 0.801). Mean subjective life satisfaction on a range of 1–7 was 5.36 (SD: 1.36, skewness: −1.32).
The characteristics of the analytic sample, both for Wave 3 respondents without missing data on adverse events or for covariates, and for all observations over Waves 1–7 without missing event or covariate data, are shown in Table S1, published as supplementary material online attached to the electronic version of this paper. Wave 3 respondents experienced a mean of 1.65 events from ages 0–49 years, with a mean of 0.65 self-oriented and 0.99 other-oriented events. Sample characteristics were similar for Wave 3 responses and observations in Waves 1–7, although respondents’ mean frailty scores were lower and household income were higher for the latter (reflecting higher likelihood of repeat follow-up for respondents with these characteristics).
Table 1 presents the weighted proportion of respondents who experienced each specific adverse event by age 16 and by age 50 years. Of 4,521 respondents with complete data on adverse events, 3,449 had experienced one or more of the 16 events assessed (weighted proportion: 75.9%). Before age 16, the most commonly experienced self- and other-oriented events were “separation from mother for 6 months or more” (13.1%) and “having parents who argued or fought very often” (13.9%). By age 50, the most common self- and other-oriented events were having a life-threatening illness or accident (15.7%) and having to provide long-term care to a disabled or impaired relative or friend (90.6%). Figure 1 and Figure S2 show the weighted cumulative proportions of respondents with full information on adverse events who experienced specific adverse events by age.
Table 1. A summary of adverse life events in ELSA Wave 3 Life History Module by self- or other-orientation and proportions of respondents experiencing specific adverse events by age 16 and age 50 (weighted, n = 4,521)
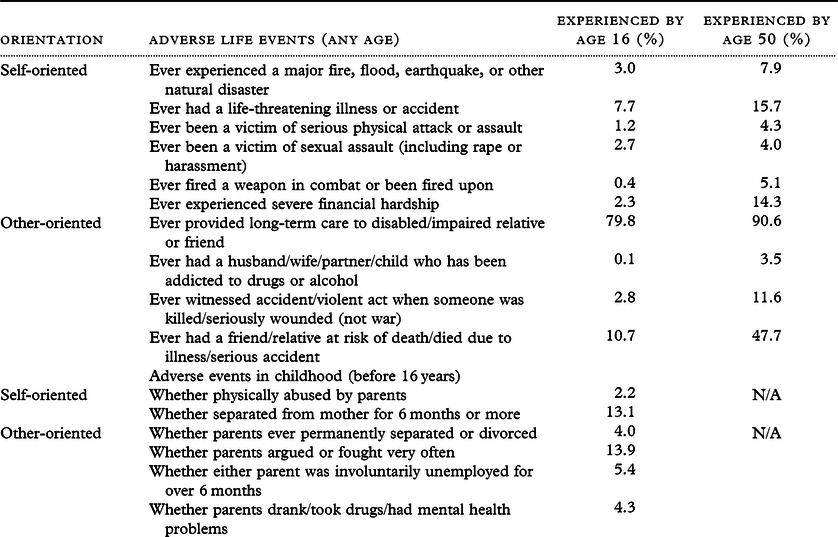

Figure 1. Cumulative proportions of respondents in the ELSA Wave 3 Life History Module experiencing specific adverse events by age (weighted, n = 4,521).
Statistical analysis
Table 2 shows the results of adjusted models for the association between total adverse events and CASP-12 and depressive caseness outcomes (Model A). Unemployment, female gender and not being in a partnership were associated with lower CASP-12 scores and higher odds of probable depressive caseness while engagement in social activities and higher household income, household net worth and occupational position were associated with positive outcomes across both measures. Age was associated with lower CASP-12 scores but lower odds of depressive caseness.
Table 2. Complete results of fully adjusted model for the association between total adverse events (0–49 years) and CASP-12 scores (n = 20,176 observations/4,176 unique individuals) and CES-D depressive caseness (n = 22,039 observations/4,208 unique individuals)

Table 3 shows the associations between total adverse events, and for events disaggregated by age and orientation (Models A–E), and CASP-12 outcomes. Total counts of cumulative adverse events over the life course (0–49 years) were associated with a decrease in scores by −0.49 (95% CI: −0.58, −0.41, p < 0.001) for each additional adverse event experienced (Model A). Adverse events occurring in all age ranges, and total self- and other- oriented events, were also associated with lower CASP-12 scores (Models B and C). When self- and other-oriented events were further disaggregated by age of occurrence (Model D), both self- and other-oriented events in adulthood (16–49 years) were associated with lower CASP-12 scores with effect sizes of −0.71 (95% CI: −0.92, −0.49, p < 0.001) and −0.50 (95% CI: −0.68, −0.31, p < 0.001), respectively. In childhood (0–15 years), other-oriented events were found to significantly predict lower CASP-12 scores in later life (−0.63, 95% CI: 0.82, −0.44, p < 0.001) while self-oriented events did not (−0.10, 95% CI: −0.32, 0.11, p = 0.354).
Table 3. Results of fully adjusted models for associations between total adverse events disaggregated by age of occurrence and self- or other-orientation (Models A–E) and CASP-12 scores (n = 20,701 observations/4,176 unique individuals)

* All models were fully adjusted for covariates including age, gender, physical frailty index, current labour market status, participation in social activities, partnership status, quintile of household net worth, household income, housing tenure at the time of interview, birth abroad and last-known occupational position (five-category NS-SEC).
Table 4 shows results for depressive caseness outcomes. Total counts of adverse events were associated with higher odds of probable depressive caseness (OR: 1.19, 95% CI: 1.14, 1.25, p < 0.001) (Model A). The same was found for events occurring in all age ranges, and total self- and other-oriented events (Models B and C). Self-oriented events in adulthood were strongly associated with higher odds of depressive caseness (OR: 1.33, 95% CI: 1.18, 1.50, p < 0.001). While we found a significant association between other-oriented events and depression outcomes (OR: 1.27, 95% CI: 1.14, 1.40, p < 0.001) no significant association was found for self-oriented events (OR: 1.07, 95% CI: 0.95, 1.21, p = 0.261) (Model D). While other-oriented events in both early childhood (0–5 years) and late childhood (6–15 years) were both strongly associated with lower wellbeing and higher odds of depressive caseness, no significant association was found for self-oriented events in early and late childhood (Model E).
Table 4. Results of fully-adjusted models for associations between total adverse events disaggregated by age of occurrence and self- or other-orientation (Models A–E), and CES-D depressive caseness (n = 22,039 observations/4,208 unique individuals)

* All models were fully adjusted for covariates including age, gender, physical frailty index, current labor market status, participation in social activities, partnership status, quintile of household net worth, household income, housing tenure at the time of interview, birth abroad and last-known occupational position (five-category NS-SEC).
Results for life satisfaction were similar to those for CASP-12 (see Table S2 and Table S3). In general, the results for all three outcomes showed two gradients in effect sizes with self-oriented events having larger negative associations with later-life wellbeing when they occurred later in the life course and the effect of other-oriented events diminishing with age.
Interaction effects obtained from latent growth curve models indicated that there was no statistically significant difference in trajectories of any of the three outcomes investigated by total adverse events (0–49 years).
Sensitivity analyses
The results of the sensitivity analyses confirm the positive and significant association between overall numbers of adverse life events (0–49 years) and counts of CES-D depressive symptoms (Appendix A8). We also found that the association between adverse events and depressive caseness remained even after excluding respondents identified with depressive caseness in Wave 3 (Appendix A9). Finally, we found a positive and significant association between experiences of adverse events and the number of waves in which an individual was identified with depressive caseness (Appendix A10).
Discussion
This study expands the evidence base on the role of experiences of different types of adverse events, and their timing, in predicting the later-life effects of trauma. Its results support the case for intensification of efforts to prevent trauma and for exposure to adverse events at all points in the life course to be considered an issue of public health concern (Magruder et al., Reference Magruder, Kassam-Adams, Thoresen and Olff2016).
The results of the descriptive analysis, based on a representative sample of the English population, highlight the widespread prevalence of experiences of adverse events, both in terms of overall exposure and exposure to specific events, together with the ages at which risk of experiencing specific events is greatest.
Consistent with expectations, we found greater cumulative exposure to adverse events over the life course to be associated with significantly lower wellbeing and increased odds of depressive caseness after age 50 (Model A). These same associations were found for overall exposure to adverse events occurring in all age ranges tested (Model B), but, in contrast with our initial hypothesis, adverse events occurring later in the life course (closer to the date of interview) were not more strongly associated with negative wellbeing and depressive symptoms compared with earlier events. While both self- and other-oriented events occurring across all life course stages were associated with negative wellbeing and mental health outcomes as hypothesized (Model C), other-oriented events in childhood were strongly associated with later-life wellbeing and depressive symptoms in older people while no significant association was found for self-oriented events (Models D and E). Both self- and other-oriented events in adulthood were significantly associated with negative wellbeing and depression outcomes.
Our results for adverse events by their orientation and timing differ from those of Shrira et al. (Reference Shrira, Shmotkin and Litwin2012) and Shmotkin and Litwin (Reference Shmotkin and Litwin2009), who found that other-oriented events, particularly those occurring in childhood, were associated with higher CASP-12 wellbeing in later life. The authors hypothesized that their finding was due to experiences of other-oriented events earlier in the life course providing opportunities for posttraumatic growth (Weiss, Reference Weiss2004), development of empathy, and a sense of commitment or responsibility to others who are victims of severe adverse events. This, in turn, is hypothesized to positively influence identity development, capacity for adaptation, and maintenance of positive wellbeing and mental health. One explanation for this divergence in findings may be that their Israeli population samples are not comparable with that of the present study; prevalence of depression is substantially higher in SHARE-Israel and other Israeli population surveys than in comparable European populations (Shmotkin, Reference Shmotkin, Jacoby and Keinan2003). Another may be that specific events occurring at particular ages may assume different meanings, and implications for wellbeing and mental health over the life course, within different social or cultural contexts (Elder, Reference Elder1998; Turner and Schieman, Reference Turner and Schieman2008); previous work has shown that cognitive appraisals of stressfulness of specific events can differ between cultural or ethnic groups (Pine et al., Reference Pine, Padilla and Maldonado1985; Brown et al., Reference Brown, Mitchell and Ailshire2018).
Counts of adverse events by age of occurrence and orientation were mutually adjusted, demonstrating that the association between childhood (particularly other-oriented) events and negative later-life outcomes not only persisted for a long period following their occurrence but were also independent of subsequent adverse events. Associations between experiences of adverse events and negative wellbeing and depressive symptoms were also independent of individual-level variables, including socioeconomic position, physical frailty, and social participation.
Our results also provide insight into how models of risk drawn from life course research may relate to individuals’ experiences of adverse events and later-life outcomes. The accumulation-of-risk model provides the best description of the associations between exposure to adverse events over the life course and later-life wellbeing and depressive symptoms found in this study. Childhood may represent a sensitive period in which other-oriented events exert a greater influence on wellbeing and mental health outcomes later in the life course, as suggested by the negative association between other-oriented events in childhood and later-life wellbeing and depressive symptoms independent of subsequent events. This sensitive period may arise as a result of other-oriented events taking a specific form and social meaning when they occur in childhood (Alwin, Reference Alwin2012) resulting in differential wellbeing and mental health effects as a result of their timing (Kuh et al., Reference Kuh, Ben-Shlomo, Lynch, Hallqvist and Power2003).
Strengths and limitations
The degree to which our results may be generalizable to contexts other than England, or to other age cohorts, is uncertain. For example, Lacey et al (Reference Lacey, Bartley, Pikhart, Stafford, Cable and Coleman2012) found that the association between parental separation and psychological distress diminished in a younger cohort when compared with an older one. The sensitive nature of some questionnaire items may have led to their underreporting. Recall bias may also have occurred; particularly for events further chronologically removed from the date of interview (Green et al., Reference Green2010; Hardt and Rutter, Reference Hardt and Rutter2004). The extent to which reports of adverse events were influenced by repression of potentially distressing memories is also unknown. Although the issue of false memories of adverse events has previously been raised (Loftus, Reference Loftus1993), this is considered unlikely to represent a serious issue in retrospective studies (Hardt and Rutter, Reference Hardt and Rutter2004). The retrospective nature of the life histories entails that no data are available from the time events occurred to validate retrospective self-reports.
Other studies raise concerns of inconsistencies in reporting of potentially traumatic events over time and whether all events are reported with equal reliability (Turner and Lloyd, Reference Turner and Lloyd1995; Hepp et al., Reference Hepp2006). One reason may be that recollections of past states or events are influenced by aspects of current circumstances, including mental health status (Ross, Reference Ross1989). Individuals use autobiographical memory to explain or justify their current state. Although contrasts between past and present states may be exaggerated when change is expected to have occurred, attitudes towards past events and their reporting may be correlated with current circumstances when an individual assumes or expects their state has remained stable over time. This “endowment effect” is likely to be stronger for more recent events as they are perceived as more closely related to the individual’s present state (Shrira et al., Reference Shrira, Shmotkin and Litwin2012). This bias is more likely to have influenced reporting of more recent events and strengthened apparent associations between adverse events and negative wellbeing and depressive symptoms, but may have been mitigated by the collection of information on life events via the separate self-completion questionnaire. The finding of a positive and significant association between number of events experienced and depressive caseness even after excluding those identified with depressive caseness during the survey wave in which adverse events were reported provides some evidence against the influence of such bias on our results (see Appendix A9).
Potential social desirability bias was also likely reduced by the absence of an interviewer for most event items. Although consistency in reporting of events could not be investigated as retrospective reports of events were recorded in one wave, use of a life grid for collection of information on all events included in the ELSA Wave 3 Life History Interview may have aided participants’ recall (Blane, Reference Blane1996).
Exposure to adverse events may not be fully exogenous to the individual. Personality traits, such as openness to experience and neuroticism, may predict both adverse events and later-life wellbeing and mental health outcomes (Ogle et al., Reference Ogle, Rubin and Siegler2014; Phillips et al., Reference Phillips, Carroll and Der2015). Parental mental illness may also predict both childhood adversity and mental illness through genetic pathways (Green et al., Reference Green2010). Related to this is the concept of dependent events, which, rather than having a direct causal relationship, may be related to the development of the mental health problem itself (Brown et al., Reference Brown, Sklair, Harris and Birley1973) or arise from the individual’s own behavior (Bebbington, Reference Bebbington1993).
Brown and colleagues make a distinction between acute stressors (life events) and chronic stressors (major difficulties); both of which are associated with onset of depression (Brown and Harris, Reference Brown and Harris1978; Brown et al., Reference Brown, Bifulco and Harris1987). This distinction is ambiguous for some of the event items in this study, particularly for certain other-oriented events in childhood. Mental health conditions are multifactorial in origin, and the relationship between individual events and mental health outcomes may be influenced by interactions with various factors (Paykel, Reference Paykel1978), including “matching” circumstances or ongoing difficulties surrounding events (Brown et al., Reference Brown, Bifulco and Harris1987), which this study may not have considered. Our measure of adverse events was based on their first occurrence and did not account for repeat occurrences. Unlike in other studies (Brown et al., Reference Brown, Bifulco and Harris1987; Ogle et al., Reference Ogle, Rubin and Siegler2014), respondents were not invited to rate their severity.
The study’s strengths include coverage of a wide range of events occurring at all stages of the life course, its use of a large sample of unique individual respondents with event data, rich covariate data and its representativeness of the English population (although this may have been weakened by ELSA’s exclusion of individuals living in institutions such as care homes or prisons). Use of multiple waves of data from the ELSA survey with observations over a period of 13 years maximized sample size. The interpretation of the results is strengthened by the fact the study employed three different outcome measures and found similar associations for each. CASP-12 overcomes weaknesses of more commonly used unidimensional wellbeing measures by assessing multiple domains of wellbeing (Hyde et al., Reference Hyde, Wiggins, Higgs and Blane2003; Vanhoutte, Reference Vanhoutte2014).
Conclusion
Poor mental health is strongly influenced by a range of social and economic determinants, including exposure to adverse life events such as violence, child abuse, and neglect (World Health Organization, 2013), and consideration of the effects of such events on both mental and physical functioning (Felitti et al., Reference Felitti1998) merits inclusion of the global public health agenda (Magruder et al., Reference Magruder, Kassam-Adams, Thoresen and Olff2016).
Identification of sensitive periods for specific types of life events in terms of their potential impact on later-life wellbeing and mental health outcomes may also guide attempts to provide timely treatment interventions to prevent or mitigate their effects (World Health Organization, 2013; Qi et al., Reference Qi, Gevonden and Shalev2016).
Further work could consider the role of culture as a moderator impact of adverse events on wellbeing and mental health (Krause, Reference Krause2004). Future studies could also adopt a “resources of resistance” perspective by attempting to identify resources which individuals may draw upon to mitigate potential negative impacts of adversity on later-life functioning, and inform design of specific “trauma-informed” interventions tailored to individuals’ patterns of exposure to adversity over the life course (Magruder et al., Reference Magruder, Kassam-Adams, Thoresen and Olff2016).
Description of authors ’roles
SR conceived the study, designed, and conducted the quantitative analysis and drafted the manuscript. EC, GN, and AS contributed substantively to the design and interpretation of the analysis and revised the manuscript for intellectual content. All authors had access to the data and approved the final draft.
Conflicts of interest
The authors have no conflicts of interest to declare.
Data sources and reproducibility
The ELSA is available to registered users from the UK Data Service website (https://beta.ukdataservice.ac.uk/datacatalogue/series/series?id=200011). Please contact the corresponding author for access to derived datasets, and Stata syntax for data management and analysis as part of this study.
Source of funding
This work was supported by the Economic and Social Research Council under Grants ES/J500185/1, ES/J019119/1 and ES/R008930/1. Funding for the English Longitudinal Study of Ageing is provided by the National Institute on Aging under Grants 2RO1AG7644-01A1 and 2RO1AG017644, and a consortium of UK government departments coordinated by the Office for National Statistics. This paper represents independent research part funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1041610220003373.