



Introduction
It is widely accepted that older adults benefit greatly from being physically active (Hartley and Yeowell, Reference Hartley and Yeowell2015; Kim et al., Reference Kim, Chun, Heo, Lee and Han2016; Yamada, Reference Yamada2016). A vast majority of older adults express that they are aware of the benefits of physical activity (Crombie et al., Reference Crombie, Irvine, Williams, McGinnis, Slane, Alder and McMurdo2004; Newson and Kemps, Reference Newson and Kemps2007; Costello et al., Reference Costello, Kafchinshi, Vrazel and Sullivan2011). Despite this awareness, many older adults are sedentary and their participation in physical activity is below established levels necessary for health improvement (Nyman, Reference Nyman2011; Mehra et al., Reference Mehra, Dadema, Kröse, Visse, Engelbert, Van Den Helder and Weijs2016). In the United States of America (USA) and Canada, older generations are consistently less active than younger cohorts (Statistics Canada, 2015; Physical Activity Council, 2020). As a result, a generational disparity exists in physical cultures, a concept which refers to the practices, rules, rituals, beliefs, norms and values that are present within spaces of physical activity (Lox et al., Reference Lox, Martin and Petruzzello2003; Shilling and Mellor, Reference Shilling and Mellor2007).
The dominant discourses shaping the physical cultures within which older adults tend to be physically active are the decline narrative and successful ageing. Related to the biomedical notion associating age with dependency and disability, the decline narrative conceives of age as a disease to be treated (Gullette, Reference Gullette1997). Successful ageing, according to Rowe and Kahn's (Reference Rowe and Kahn1997) model, is defined as maintaining independence, avoiding disability and disease, and engaging in productive, social activities. In physical cultures, exercise is positioned as an anti-ageing treatment in order to age successfully and avoid decline (Katz, Reference Katz2000, Reference Katz2001; Tulle, Reference Tulle2008; Gilleard and Higgs, Reference Gilleard and Higgs2013). Notable critiques of these discourses, in the context of physical cultures, include a need to address the stigmatisation that arises from blaming individuals’ sedentary lifestyles for failing to age ‘successfully’ (Allain and Marshall, Reference Allain and Marshall2017) and the fitness industry's misleading claims regarding the extent to which exercise can affect the ageing process (Tulle, Reference Tulle2008).
More recent counter-discourses shaping the physical cultures within which older adults might be physically active are less concerned with successful ageing's and the narrative of decline's foci on corporeal ageing, and more concerned with the social and embodied meaning of physicality and movement. We provide three examples. First are the sensual and affective discourses of pleasure, fun and enjoyment (Poole, Reference Poole2001; Phoenix and Orr, Reference Phoenix and Orr2014; McPhate et al., Reference McPhate, Simek, Haines, Hill, Finch and Day2016). Phoenix and Orr (Reference Phoenix and Orr2014) offer a four-part typology of pleasure in physical activity: sensual pleasure, pertaining to the sensations felt during an activity; documented pleasure, thereby extending enjoyment via writing about the activity; the pleasure of habitual action, appreciating the structure and purpose provided by routine physical activity; and the pleasure of immersion, wherein the physical activity acts as an escape from daily stressors. Second are the discourses pertaining to socialisation and community (Tulle and Dorrer, Reference Tulle and Dorrer2012; McPhate et al., Reference McPhate, Simek, Haines, Hill, Finch and Day2016). Tulle and Dorrer (Reference Tulle and Dorrer2012: 1124) recommend that community-oriented physical cultures ‘aimed at fostering enjoyment and happiness derived from the discovery of physicality, and the creation of social ties when these have disappeared, should be given priority over the strict focus on form and health’. Third is the recent proposed reframing of physical activity as a ‘career’ in order to oppose the decline narrative (Palmer et al., Reference Palmer, Bowness and Tulle2021). This discourse offers a metaphor for explaining the ebbs and flows of socially contextualising factors as they affect physical activity patterns, habits, aims and preferences throughout the lifecourse.
These discursive perspectives inevitably influence the exercise environment and impact the subjective experience of exercisers (Paulson, Reference Paulson2005; Tulle and Dorrer, Reference Tulle and Dorrer2012). One way in which they do so in a group exercise environment is via the ideological positions of the exercise instructors. Accordingly, the meanings that older adults attach to their exercise experiences shape the meanings of physical cultures for older adults (Sims-Gould et al., Reference Sims-Gould, Hurd Clarke, Ashe, Naslund and Liu-Ambrose2010). Scholars have found that instructors who embody the decline narrative in their teaching create barriers by imposing unnecessary limitations, based on ageist assumptions, on older exercisers (Kluge and Savis, Reference Kluge and Savis2001). Instructors who embody the discourse of ‘successful ageing’ in their teaching have been critiqued for failing to relate to older exercisers by ignoring the realities of corporeal ageing (Andrews, Reference Andrews1999) and focusing on constant improvements, as measured by metrics of exercise quantity, rather than focusing on the quality of the exercise experience (Tulle and Dorrer, Reference Tulle and Dorrer2012). Both environments tend to result in low attendance and adherence to exercise because the physical culture created by the instructor fails to align with the desires of the older exercisers. Conversely, instructors who emphasise fun and community have been found to engender more inclusive physical cultures for older exercisers (Tulle and Dorrer, Reference Tulle and Dorrer2012; McPhate et al., Reference McPhate, Simek, Haines, Hill, Finch and Day2016).
Leaders of exercise classes have been found to be vital determinants of exercise enjoyment and adherence (McAuley and Jacobson, Reference McAuley and Jacobson1991; Carron and Spink, Reference Carron and Spink1993; Carron et al., Reference Carron, Hausenblas and Mack1996; Petrescu-Prahova et al., Reference Petrescu-Prahova, Belza, Kohn and Miyawaki2015). Previous research has also pointed to a lacuna in scholarship that connects what instructors are taught by certification bodies to what instructors in turn teach to their exercise clients (Markula and Chikinda, Reference Markula and Chikinda2016). Following this line of inquiry, this research employed an institutional ethnography (IE) approach in order to uncover the social discourses that shape socially (in/ex)clusive physical cultures for older exercisers in both mainstream and older-adult group fitness classes, with specific attention paid to the influence of exercise instructors. Our aim in undertaking this research was to contextualise and understand the socio-cultural influences that affect the teaching methods that exercise instructors employ in both mainstream and older-adult group fitness classes. Herein, we argue that attention must be paid to the policies and professional practices that govern how exercise instructors conceptualise and deliver older adult exercise programming (Smith, Reference Smith and May2002, Reference Smith and Hesse-Biber2007), ‘so that how [this world] is being put together can be made observable from the point of view of those caught up in it’ (Smith, Reference Smith and Hesse-Biber2007: 411).
Methodology
To study the social process of teaching that takes place between instructors and older exercisers, the method of inquiry underlying this study is an IE. Because IE is attuned to the shared experiences of the social groups under investigation, IE's social ontology is well aligned to the constructivist position (Smith, Reference Smith and May2002, Reference Smith2005, Reference Smith2006). IE neither contributes to theory nor makes any assumptions as to the meanings ascribed to social processes; therefore, we did not impose a pre-conceived theoretical framework (Smith, Reference Smith and May2002, Reference Smith and Hesse-Biber2007; Rankin, Reference Rankin2017b). That said, IE's roots are in critical theory, and thus aligned with our aim of elucidating influences of power governing the interactions taking place between instructors and older exercisers (Smith, Reference Smith and Hesse-Biber2007). Modern iterations of power are said to be ‘exerted through the documentary processes used to describe, categorize, define, direct, visually represent, or otherwise coordinate and control the everyday world’ (Townsend, Reference Townsend1996: 188). Given that fitness is an institution governed by rules and policies, as articulated and passed across time and place via texts, reliant on competent social actors, such as instructors, to enact these rules (Campbell and Gregor, Reference Campbell and Gregor2004; Ecclestone and Jones, Reference Ecclestone and Jones2004), IE was the best methodology to address our research question.
The research question underlying this study was:
• What are some of the socio-cultural discourses represented in the training and workplace policies that govern how exercise instructors conceptualise and deliver older adult exercise programming, and how might this affect the (in/ex)clusivity of social exercise environments?
To answer this question, we (a) investigated the local, or daily experiences, of the exercise exchange between instructors and older exercisers, drawing attention to older exercisers’ experiences of (in/ex)clusivity; and (b) mapped the socio-cultural influences (also known as ruling relations in IE) at the translocal level (influences that are beyond observation in the ‘local’ experience) that affect these daily experiences (Campbell and Gregor, Reference Campbell and Gregor2004).
Methods
IE does not specify how one should conduct their research, but rather outlines that for which one should look (Campbell and Gregor, Reference Campbell and Gregor2004). DeVault and McCoy (Reference DeVault, McCoy and Smith2006) describe this approach as emergent, and approaches vary for each project. As outlined by Campbell and Gregor (Reference Campbell and Gregor2004), the researcher in an IE follows leads, following ruling relations, to map the ways in which embodied subjects are connected to larger networks of influence. When it appears that no novel data can be added, and when no further mapping can occur, the study is considered complete. To this end, IE might integrate several methods for data collection, such as interviews and observations, all of which were employed in this study.
The local
The local focus in IE is on people's actual behaviours by attending to how people engage in work, defined broadly from Marx and Engel's conceptualisations of work as a material practice (Townsend, Reference Townsend1996; Townsend et al., Reference Townsend, Langille and Ripley2003; Campbell and Gregor, Reference Campbell and Gregor2004; Quinlan, Reference Quinlan2009). Informants who work within the institution under investigation are a means of entry into the topic being researched; therefore, we sought first to speak with informants, as research participants are called in an IE, about their day-to-day work experiences (Campbell and Gregor, Reference Campbell and Gregor2004; Campbell, Reference Campbell and Smith2006). Informants in this study consisted of older exercisers and exercise instructors.
To investigate the local, lived experience, KH utilised a go-along method and semi-structured interviews with 14 older exercisers for a total of 25 observational hours in community group exercise classes (both mainstream and classes specific to older adults) (Table 1). Go-alongs are a phenomenologically informed method for capturing reflexive embodiment ‘in situ’ (Kusenbach, Reference Kusenbach2003: 455, original italics), which consist of simultaneous observation and in-depth, qualitative interviews in the observational setting. We deemed go-alongs to be the most appropriate method, because interviews in IE are framed as ‘talking to people’ (Campbell, Reference Campbell and Smith2006: 77), much in a manner like a go-along interview. Thus, KH accompanied and exercised alongside the exercisers at the group exercise classes that the exercisers normally attend.
Table 1. Details of the exercisers
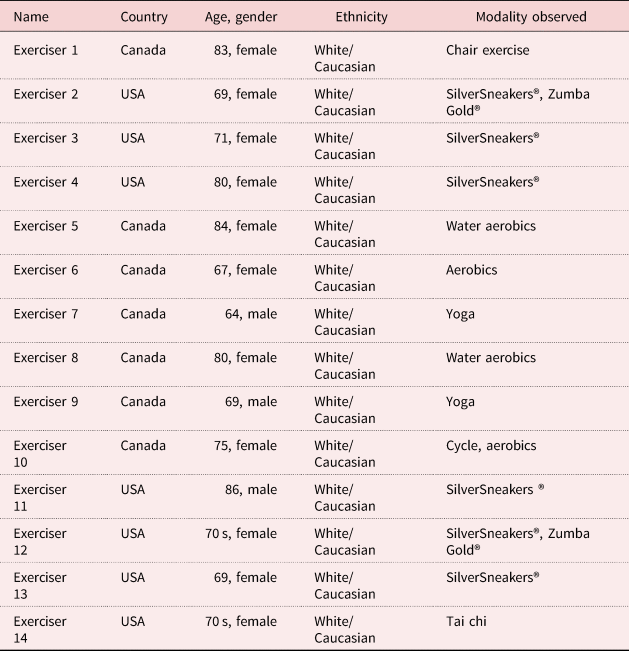
Note: USA: United States of America.
The go-along was complimented by a semi-structured interview that took place after the exercise class so that the researcher could pose questions about the class experience. Informants may not be explicitly aware of the ways in which their work is organised, thus IE aims to involve informants actively in the process of uncovering and describing the influence of these social processes (Campbell, Reference Campbell and Smith2006). Herein, our focus was on what the informant disclosed about their work, materially, and how it connected them to a larger network of social actors engaged in that work, ideologically (Rankin, Reference Rankin2017b; Smith, Reference Smith and May2002). It was also here where we grounded our ‘standpoint’ (Rankin, Reference Rankin2017a), centring our analysis on the embodied experiences of these older exercisers.
In an IE, the aim is ‘to locate and trace the points of connection among individuals working in different parts of institutional complexes of activity’ (DeVault and McCoy, Reference DeVault, McCoy and Smith2006: 18). Thus, extending from the local experience of older exercisers, we next investigated the work of exercise instructors. KH observed, for a total of 47 hours, and conducted semi-structured interviews with 22 exercise instructors (Table 2). Instructors were purposively sampled with an aim for heterogeneity such that instructors possessed a range of social characteristics (e.g. race/ethnicity, age, body type, gender/sex, etc.). We did not limit this sample to only those affiliated with the older exercisers involved in the study, as this would restrict the contexts in which instruction is observed, and as such we would not be able to ascertain if our observations were idiosyncratic or normal operational procedures (Campbell and Gregor, Reference Campbell and Gregor2004).
Table 2. Details of the exercise instructors

Notes: USA: United States of America. CCAA: Canadian Centre for Activity and Aging. 1. ‘Other’ means that the instructor held a certification, or certifications, that did not correspond to the eight certifications and/or certificates included in this study (as noted in Table 1).
All informants signed an informed consent form; instructors signed an additional form acknowledging that their employers were aware of and consented to the instructor's participation in the study. All participants of the classes observed were notified of the researcher's presence and data were only collected on those who consented to participate in the study. Ethics was approved by the university ethics board. All interviews, except one, were digitally recorded and transcribed verbatim (one informant did not consent to the use of the recorder for their interview and so handwritten notes were taken).
The translocal
Ruling relations are ‘individuals, organizations, professional associations, agencies and the discourses they produce and circulate’ (Mykhalovsky and McCoy, Reference Mykhalovsky and McCoy2002: 19) that govern, in this study, how exercise instructors conceptualise and deliver exercise programming for older adults (Smith, Reference Smith and May2002, Reference Smith and Hesse-Biber2007). In an IE, texts are a ‘means of access, a direct line into the relations it organizes’ (Smith, Reference Smith1990: 3). Texts are unchanging and a means by which work practices are standardised, even if the ways in which the texts are read and enacted may differ by individual interpretation (Walby, Reference Walby2007; Gergen, Reference Gergen2009; Quinlan, Reference Quinlan2009). In this study, the ruling relations consisted of the national and international policy documents that influence certifying bodies, as well as the certifying bodies themselves, that develop and deliver the curricula that are used to train and certify exercise instructors who work with older adults. Therefore, to uncover the translocal influences of power exerted by ruling relations to govern how exercise instructors conceptualise and deliver older adult exercise programming, we collected myriad texts as data (Rankin, Reference Rankin2017a).
Ultimately, we included eight curricula used for training and certifying exercise instructors from five certifying bodies in Canada and the USA in this study (Table 3). The curricula varied in terms of mode of delivery and materials included, thus texts included in analysis were comprised of: print manuals; print study guides; handouts; online course resources including video learning modules; transcripts; and practice exams. We also included marketing materials and information from these bodies’ websites where applicable.
Table 3. Curricula included in content analysis
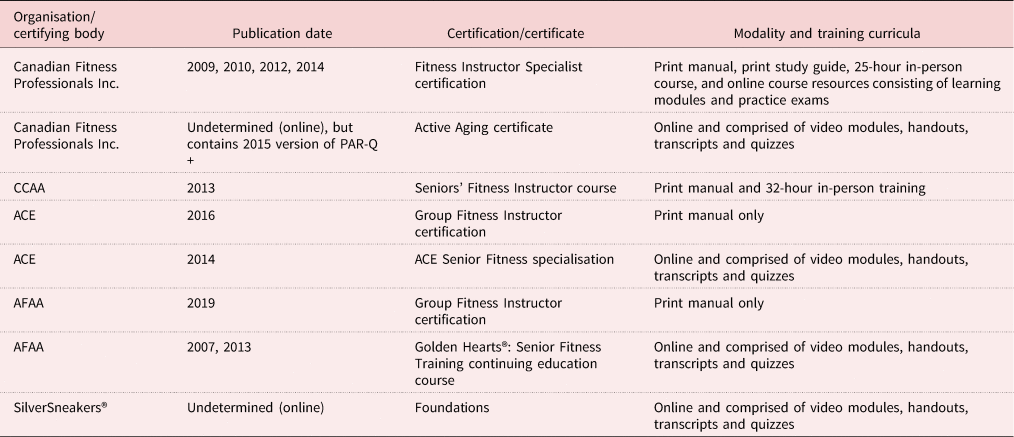
Notes: CCAA: Canadian Centre for Activity and Aging. ACE: American Council on Exercise®. AFAA: Aerobics and Fitness Association of America®. PAR-Q+: Physical Activity Readiness Questionnaires.
Analysis
KH read the texts, transcripts and notes from observations, and extracted data that pertained to work, as defined above. KH then re-read the data and identified the following themes: jargon; exercise environment and music; age relations, ageism and age segregation; health; professional practice; safety and efficacy; certification; employer policies; screening; class planning; progressions, regressions and modifications; industry trends; activities of daily living; contraindications; neoliberalism, efficiency and risk. For this paper, we re-read the data coded for screening, progressions/regressions/modifications and contraindications. For each of these three themes, we first looked at the data from the exercisers to centre their experiences. We then mapped the linkages between exerciser and instructor experiences, finding converging and diverging perspectives. Similarly, we then traced connections between exerciser/instructor interactions to data extracted from the texts. Throughout, we paid attention to how the language utilised in these curricula (Smith, Reference Smith and May2002) and how the discourses contained therein were embodied and carried out in the daily context of groups exercise for older adults (DeVault and McCoy, Reference DeVault, McCoy and Smith2006).
Reflexivity and rigour
In IE, the researcher is considered to be part of the social environment and their role is an analyst who should side with, and advocate for, the subject under scrutiny (Campbell and Gregor, Reference Campbell and Gregor2004; Smith, Reference Smith2005), which in this study was taking up the ‘standpoint’ of older exercisers. It is this notion of ‘taking sides’ (Freire, [Reference Freire1970] 1993) that expose IE's critical underpinnings. It is also a critical emphasis that informs IE's orientation towards social democracy and advocacy (Campbell and Gregor, Reference Campbell and Gregor2004). It is therefore imperative that researchers engage in reflective practice to acknowledge the power their position might entail, which is particularly vital when research is undertaken by ‘insiders’, like KH, who is a professionally trained group exercise instructor (Rankin, Reference Rankin2017b). Reflexive practice helps ensure that findings are reflected in the data, establish the ways in which the researchers’ positionalities could influence the study's outcomes and mitigate any potential for the abuse of that power, thus preventing acting as an ‘imperialist’ researcher (May, Reference May2002; Smith, Reference Smith2005; Walby, Reference Walby2007). Therefore, the authors engaged in the practice of reflexivity throughout the course of the study via written, reflexive field notes and working as ‘critical friends’, wherein KH discussed challenges and reflections with MG (Groenewald, Reference Groenewald2004; Smith and McGannon, Reference Smith and McGannon2018).
To ensure rigour, we employed principles put forth by Smith and McGannon (Reference Smith and McGannon2018). Firstly, we made use of member reflections by asking informants in interviews if the findings from a literature review on the topic of study was compatible with their lived experience (Campbell and Gregor, Reference Campbell and Gregor2004; Smith and McGannon, Reference Smith and McGannon2018). Secondly, we engaged in the aforementioned practice of consulting critical friends (Smith and McGannon, Reference Smith and McGannon2018). Finally, because rigour is established in IE through the accuracy of mapping social relations (DeVault and McCoy, Reference DeVault, McCoy and Smith2006), we employed empirically based, relativist criteria to ensure that the social relations mapped were grounded in the data collected and the resultant networks were a correct representation of that which was established in the data (Smith and McGannon, Reference Smith and McGannon2018).
Findings
An IE investigation centres around the problematic, the contradictions and tensions that render individuals in the local setting powerless (Townsend et al., Reference Townsend, Langille and Ripley2003; Rankin, Reference Rankin2017a). According to Rankin:
The problematic is generated from the data, and it often rests on stories (accounts) that reveal troubles arising in (or conflicts between) authorized and experiential knowledge; whereby the tensions that standpoint informants know about and experience are either invisible or misrepresented within the authorized accounts. (Rankin, Reference Rankin2017b: 3, original italics)
The primary problematic underlying this study is that the work undertaken in the fitness industry to create inclusive group fitness classes produces age-exclusive exercise markets that conflate age and ability, thus upholding the decline narrative by implicitly equating youth with health and ability, and older age with disease and disability. In the findings that follow, we share data that weave together material and ideological accounts whereby authorised knowledge embedded in curricula used to train and certify exercise instructors, and hence practised by instructors, is at odds with both the experiential knowledge possessed by instructors, as well as the standpoint of older exercisers. Additionally, at times, we highlight contradictions between these accounts.
Curricula and certification
Segmenting the exercise market stems from national and international guidelines, as well as professional standards of practice documents, that influence what information is taught for entry-to-practice group exercise instructors. The USA (Jones and Clark, Reference Jones and Clark1998) and Canada (Canadian Centre for Activity and Aging and Health Canada, as cited in Ecclestone and Jones, Reference Ecclestone and Jones2004) independently developed national guidelines to inform curricula development for group exercise instructors who work with older adults. This was because they recognised that, given the increased incidence of chronic health conditions in the older population, ‘programming for older adults require[d] more care and expertise than for other age groups’ (Jones and Clark, Reference Jones and Clark1998: 208) and entry-to-practice training for mainstream group exercise was insufficient for working with older adults (Markula and Chikinda, Reference Markula and Chikinda2016). These guidelines thus acknowledge that older exercisers require adapted exercise instruction for their unique physical and psycho-social circumstances. Specifically, they call for ‘moderate-intensity programs’ for ‘independent senior adult participants with medical clearance’ (Jones and Clark, Reference Jones and Clark1998: 214), thus excluding frail older adults, who would require instructors with specialised training. Several certifying bodies included in this study were partners in adopting these curricula guidelines, thus demonstrating a direct link between these guidelines and the curricula included in this analysis.
These national guidelines were later developed into the International Curriculum Guidelines for Preparing Physical Activity Instructors of Older Adults (Ecclestone and Jones, Reference Ecclestone and Jones2004), which was spearheaded again by a number of organisations and individuals affiliated with the certifying bodies included herein. These guidelines have been praised for taking a holistic approach to understanding physical activity and ageing (Grant and Kluge, Reference Grant and Kluge2007). Comprising this approach are nine suggested training modules: (1) an overview of physical activity and ageing; (2) multi-disciplinary conceptualisations of ageing; (3) screening and assessing as part of goal setting; (4) exercise programme planning and design; (5) how to adapt exercises for older adults diagnosed with common medical conditions; (6) educational skills; (7) business, communication and leadership skills; (8) safety and first aid; and (9) professional, ethical and legal considerations (Ecclestone and Jones, Reference Ecclestone and Jones2004). With the exception of modules 1, 2 and 5, when mapped on to mainstream group exercise performance standards (i.e. National Fitness Leaders Association Canada, 2020), there is considerable overlap between the expectations for mainstream and older adult fitness. In the sub-sections that follow, we explore how some of these modules are represented in the training curricula, enacted by the instructors informing this study and received by the older exercisers who participated in this research.
Screening to ensure safety
According to most certifications, and as aligned with suggested modules 3 (screening) and 7 (legal issues) from the international guidelines, proper screening of the prospective exerciser is a vital practice for identifying exercisers who are at risk of injury or death as a result of becoming more physically active. In canfitpro™'s training, wherein they cite leading medico-legal experts Drs JoAnn Eickhoff-Shemek and David Herbert (and colleagues), ‘Pre-exercise screening is part of your duty to care, and it is your legal responsibility’; therefore, by not screening exercise professionals are at risk for ‘unnecessary’ liability and clients are at risk. Negligence, including failing to screen participants, could lead to liability for the instructor and their employer where applicable.
In our appraisal, screening tools are laden with age-based assumptions, thus demonstrating how the separation between mainstream and older adult fitness and physical cultures is materially embodied in these screening methods. For instance, the Physical Activity Readiness Questionnaires (PAR-Q), developed by the Canadian Physiological Society (Warburton et al., Reference Warburton, Jamnik, Bredin and Gledhill2014), was the most often utilised screening tool by the group exercise instructors observed. A copy of the PAR-Q was provided by all curricula, except one. With the exception of canfitpro™, which recommends the latest iteration of the PAR-Q (the PAR-Q+ which is for screening everyone, regardless of age), these curricula acknowledged that the PAR-Q was only validated for people aged 15–69, thus excluding a good proportion of older adults (Warburton et al., Reference Warburton, Jamnik, Bredin and Gledhill2014). Based on publication dates, the PAR-Q+ may not yet have been available before some of the other curricula were being developed and published (see Table 1), thus this exclusion can, in part, be explained by a structural lag (Warburton et al., Reference Warburton, Jamnik, Bredin and Gledhill2014).Footnote 1 However, it stands to note that older adults were once excluded from many screening and testing procedures in fitness and physical cultures because of a lack of empirical work to validate tools for this population. This is also indicative of the problematic lack of ‘normative’ data for older adults in regards to screening tools. Moreover, in the absence of screening tools appropriate for use with older adults, or with persons diagnosed with one or more chronic conditions, these curricula recommended medical clearance, which was acknowledged in the curricula as a potential barrier to exercise participation.
Despite emphasising the importance of screening, the curricula also acknowledged that screening was outside the scope of professional practice for many group fitness instructors. Indeed, this was the case as observed by KH. We observed that most group exercise instructors employed by a gym, or similar establishment, did not perform any assessments or screening measures, citing lack of money and time, except in the rare circumstances where required by the employer. For instance, Instructor 1, who worked for a regional fitness chain, explained to us that they are paid for the hour of teaching the class, and not for socialising with participants, preparing or planning their classes, or screening their exercise participants. Instructor 2, on the other hand, shared that they spend an extra two to three hours on bureaucratic work required by their employer:
So, the sign-in sheets, I have to do them. I have to redo them because there's a lot of new people. I have to get the PAR-Q for them, like the … you know that, right? So, I have to make sure those new people, get them signed in. So, there's a lot of little paperwork. Then I've got to go and clean the equipment, so sanitise it … So a lot of little things but, believe it or not, they take time.
This stands in stark contrast to Instructor 3, who is self-employed and thus is not constrained by the same institutional forces as Instructors 1 or 2. Instructor 3 expressed to us that they valued taking time to socialise after class, citing that they felt this practice was important for combating social isolation, engendering group social cohesion, and boosting attendance and adherence among their older clients. Being self-employed, Instructor 3 chose to be social on their own time, but being self-employed, they were also required to keep on file a copy of their clients’ completed PAR-Q forms. One rationale for this is that self-employed instructors purchase their own liability insurance; whereas, instructors employed by a gym or facility are covered under the business or organisation's insurance policy. Therefore, the onus to complete assessments shifts depending on who is the purchaser of the liability insurance.
Instructors who employed the PAR-Q (Warburton et al., Reference Warburton, Jamnik, Bredin and Gledhill2014) recognised some shortcomings. According to Instructor 4:
If you have 50 people in the class you won't sit with each one before the class and get to know them, but when you ask them a question, ‘Is there anyone here that has or suffer from whatever, do you guys get dizzy or if you're intensely working out with high [intensity]’ – whatever, any of those simple questions they will let you know. You will know what's in your class, you know, and at the end there is the waiver, you're safe but at least you know how to deal with them. So that's the way I do it before – if I'm going to a new class at the beginning.
Now it's different because I co-ordinate different programmes and I have certain ways when I start the programme. So, like us here they have to register with me and I have the PAR-Q, I have the health questionnaires. I have an individual kind of conversation with them in case if needed, but in general, I check everybody is okay, we're okay to do that. Now changes happen, sometimes things happen during your class, before the class maybe something happened yesterday and I didn't know, I always tell them if something happened that I don't know and I have to know it before we start, please let me know.
What this demonstrates is instructors’ use of informal screening methods. Whether due to lack of time, resources or mandates from employers to assess exercisers formally or due to the recognition that the information collected by the PAR-Q is static, but exerciser's health status is dynamic from day to day, Instructor 4 will informally assess their clients before, during and after class, and adapt their exercise programme accordingly to meet exercisers’ needs in situ.
Grant and Kluge (Reference Grant and Kluge2007) posit that predominately focusing primarily on quantifying physical functioning and abilities of older adults, as in the case of screening tools, the biographical meaning making on the part of older adults is absent and marginalised from these official texts. Thus, they argue that it is vital to explore older exercisers’ experiences of being screened. Yet, from the standpoint of older exercisers who participated in this study, very few were on the receiving end of any screening measures and did not express being aware that these screening tools were exclusively based on age. Therefore, older exercisers were ignorant to the ways in which these screening tools quantified their ageing bodies. What was important to older exercisers, however, was the actual exercises selected by the instructor and how these exercises were progressed, regressed or modified.
Progressions, regressions and modifications
One aim of screening, as cited by the training curricula, is to ensure that the exercises selected by the instructor are considered safe for the exerciser. Thus, the information derived from screening should inform module 4, exercise programme planning and design, and module 5, how to adapt exercises for older adults, from the aforementioned international guidelines. This approach, as outlined, works well in personal training where exercise interventions can be personally tailored, but is not as feasible in group fitness whereby the needs of the individuals are subordinated to the needs of the group (Carron and Spink, Reference Carron and Spink1993). Instead, training curricula suggest that ‘Appropriate progression and regression options should be included within class blueprint in order to ensure … inclusive movement experiences’ (American Council on Exercise), which Instructor 5 articulated is their aim as an instructor:
I say this to people all the time … that's what we pride ourselves on, is that we want anyone to be able to step into a class and feel accomplished when they step out. So, like, it's a tough part of the job of the instructor, but that's part of my job, that's what I signed up for, and if you step into my class, I want you to feel like you went out, having the workout that you came for.
It therefore appears that the provision of options, known as multi-level teaching, may indeed foster more inclusive physical cultures.
Every curriculum promoted inclusive instruction via multi-level teaching styles wherein modifications, regressions and progressions were offered. Training manuals explained that progressions ‘progress’ and make an exercise more challenging; whereas, modifications and regressions describe the ways in which the exercises are adapted when a particular body/person cannot or should not perform a particular movement. Herein, manuals specified that modifications and regressions may include safer substitute movements, such as low- or non-impact exercises to replace movements that are high-impact. Informants, instructors and older exercisers alike expressed the importance of progressions, modifications and regressions. Consider Instructor 6's experience:
I teamed up with another instructor last summer. So, I took pilates and this instructor was probably like maybe 22 and trains athletes. Who knows who's going to show up [to the class]? So, he's ready to do boot camp, you know, run and down the trail and calisthenics and he had three people show up that probably hadn't worked out in ten years and then a bus pulled up of special needs people. And that was his group that he had to work with. And he panicked, like he didn't know what to do. And at the end he just looked at me like a deer caught in headlights and he was just like, ‘I just wasn't expecting that.’ So, like I think when you do SilverSneakers® like you learn all your modifications for everything and that carries over to every group. So, it's not necessarily, you know, a 30-year-old could have blown out their knee and they come in the gym, what are you going to do, if you don't know how to modify? So, that's my approach to every class.
From the standpoint of older exercisers, modifications were highly valued, as exemplified by Exerciser 1:
…there are some things that I used to do on the floor a lot before … that I don't know if I could do now. That's why, like, she's going to do yoga with us, but we're going to do yoga in the chair. So, no problem, although I did do yoga two years ago and that was on a mat, but I can't do as much as I used to in that respect. When I did yoga before, I could stand without holding on, but after I broke my femur, I don't have the type of balance I had and I think that injury is more than age and trying, because [that exerciser] over there is 95 and she moves like crazy.
Both Instructor 6's and Exerciser 1's examples not only underscore the importance of modifying exercises in order to be more inclusive, but also highlight the importance of health and functional ability-based, rather than chronologically age-based, criteria. The latter conflates age and ability, and is therefore ageist because age as the sole criteria is determining what is considered to be safe practice (Kluge and Savis, Reference Kluge and Savis2001). Moreover, ability-based criteria are grounded in reality that bodies (of all ages) vary in their performative abilities.
However, instructors and exercisers alike pointed out shortcomings with the multi-level approach touted by the curricula. As Instructor 7 observed: ‘I find that when you teach even when you give modifications people tend to do what you're doing.’ Instructor 8's answer to this was to normalise the modification, but also push when necessary:
Some of the times [I] just to say, ‘Hey, everybody, I'm giving you permission to use the block. I'm on it.’ Like, you know, that kind of thing, I think is important. The modifications would definitely be something that I'm bringing to people's level to make it more accessible. I push myself to make sure that everybody's getting a challenge. So, I may be bringing it up sometimes, so I think it's up and down during a practice.
Instructor 5 elaborated how modifying was even more challenging in a class serving heterogeneous clients, such as a group exercise class for older adults, by asserting that, ‘there's always a range in every class that you have to be prepared for, but it's really, really large in [the low-impact group]’.
Exercisers too commented on the limitations they perceived with regards to multi-level teaching. Exerciser 2, for example, emphasised that modifications may not be enough to create inclusive physical cultures:
Because you've got more people with different abilities and everybody tries to up it a little bit. No, some people can do some things better than others, but it's not like so far out of the realm that you're never going to get there. They tell you to modify it. But if you're the only one modifying it … you never think you're going to get to there. Yeah, there's certain restrictions, physically, as you get older. And, you know, like I said, if you're struggling with introductory to algebra, you don't want to sit in the calculus class.
Exerciser 2's comparison of mainstream exercise to calculus brings to the fore an essential problem with teaching multi-level classes: one can modify, but only so far from the benchmark; at some point, there is a need to change the benchmark in order to meet the needs of people whose abilities are not otherwise met. Herein, again, Exerciser 2 draws attention to ability-based interventions; however, some of the analysed certifications have taken to age-based criteria for determining what exercises are appropriate for a given population.
Contraindicated exercises
Modification might, at times, mean foregoing specific movements altogether, as is the case of contraindicated exercises, or exercises that are deemed inappropriate, unsafe and not recommended for certain populations. The national and international guidelines do not provide any advice regarding specific exercises; therefore, each curriculum is free to take a different approach to contraindicated exercises. Some curricula did not specify contraindicated movements for older adults; some curricula described circumstances under which certain exercises are contraindicated, such as in cases whereby a person with a particular chronic condition should not perform a particular movement for safety reasons; and one curricula outlined some contraindicated movements that no member of the general public should perform.
While some manuals endorsed health- and ability-based criteria for the determination of contraindicated movements, the two organisations where older adults are the sole receivers of the exercise product (the others have mainstream fitness equivalents serving people of all ages) specified distinct exercises that are contraindicated for all older exercise participants, regardless of ability or health. The rationale these curricula provided was that broad application of contraindications for all exercisers ensures safety of the masses given that an instructor may not know everyone's health status, older exercisers might not be aware of or forthcoming about their health status, and/or the group exercise instructor might not perform screenings or assessments.
In practice, abiding by the rules of one's certification varied with respect to contraindicated exercises. Consider the following observations whereby instructors either: willingly or mistakenly failed to respect the contraindications mandated by their certification; employed relativist criteria for the application of contraindications, respecting contraindications in group exercise classes branded by their certification but not transferring these contraindications to their mainstream classes even when the same older adult attends both class formats; or applied contraindications to only those in the class for whom those contraindications are appropriate. Firstly, Instructor 9, who is not certified, was observed including moves that are, in KH's estimation, no longer considered safe in either older adults or mainstream exercise; whereas Instructor 10 included two contraindicated moves in their exercise class (as determined by comparing observations to contraindications outlined in the curricula under which Instructor 10 was certified). The contraindicated movements that Instructor 10 included are often employed in mainstream fitness, and were indeed observed therein.
Secondly, Instructor 6 was observed abiding by the contraindicated regulations of SilverSneakers®, but only in SilverSneakers® branded classes, not in mainstream or other branded classes. Likewise, Instructor 11 was observed abiding by the contraindications dictated by SilverSneakers®, but used their professional judgement when teaching Zumba® Gold class. Herein, Instructor 11 was observed using a microphone despite the fact that Zumba® Gold's professional practice is for exercisers to follow the instructor's lead, and as such instructor's do not talk during the class. Instructor 11 violated this professional practice, because they shared with us that they believe it is important to be able to communicate verbally to older clients during class. However, no other Zumba® Gold instructor observed violated this principle. Finally, rather than applying across-the-board contraindications, some instructors applied contraindications to only those in the class for whom those contraindications are appropriate, thus allowing exercisers to use their judgement as to whether or not to perform the potentially contraindicated exercise. This was indeed the case observed wherein Instructor 2 told people that a particular exercise is contraindicated for people with a hip replacement, offering them a modification, but inviting the rest of the class to perform the exercise.
Employing relativist criteria, as Instructor 2's example exemplifies, requires professional expertise. However, instructors are taught that they must abide by the curricula in order to maintain their certification, which at times can mean subordinating their expertise. However, the following provides a poignant example where we witnessed an instructor push back against institutional ruling relations that govern the actions of the exercise instructor, thus prioritising their professional judgement. Instructor 4 shared with us how they pushed back when going through one particular instructor training. They disagreed with the certification body's requirement that instructors teach in accordance with their guidelines, including contraindications outlined in the certifying body's curriculum. Indeed, as in Rankin and Campbell's (Reference Rankin and Campbell2009) study of nursing, the guidelines to which exercise instructors must abide according to their certification subordinate their professional competence and serve as a means to rationalise when and with whom certain exercises are employed.
Instructor 4 questioned how this particular certification body's requirement to apply condition-specific contraindications benefited the older exerciser. They shared with us that this approach distils the exerciser down to only one health problem, rather than considering them as a holistic person with many other potential needs and/or conditions. Rather, Instructor 4 emphasised the importance of pre-screening and listening to the exerciser to ascertain their concerns and needs in order to determine what exercises are appropriate and inappropriate for each individual exerciser. The example Instructor 4 shared was: if the individual has osteopenia and is at a slight risk for fracture, then a spinal rotation stretch is considered contraindicated. However, if this individual also is diagnosed with Parkinson's disease, then trunk rigidity is a concern and a spinal rotation stretch is highly indicated. Thus, a holistic approach would be to weigh the benefits and risks and teach proper form.
Like Instructor 4, Instructor 7 questioned the rationale for certain contraindications, calling them ‘limiting’, and instead deferred to their own expertise and competence as a group exercise instructor:
…So, technically I'm not supposed to do grapevines but I'm like why would I tell someone not to do something that works on agility and balance, and side movement when they can do it? So, I give them options … If you don't want to go – I know that I cued it today but sometimes I'll say if you're comfortable going away from the chair but not crossing your feet you can march to the side and come back. Why would I hold somebody back when they can do it?
Here, Instructor 7 weighed the benefit of the exercise against the risk and implicitly endorsed ability over age, which resulted in going against the advice of their training and certification. Instructor 7 continued:
I have people that come to SilverSneakers® class and now they want to do other of my [mainstream] classes, right? So, I just explain and again I've told you my philosophy is I want it to be accessible on as many levels as I can so to me the only difference is you have to be able to get on the floor.
Recognising that older adults can, and do, attend both her mainstream and older-adult specific classes, Instructor 7 exposes the problematic of applying age-based criteria without consideration of ability, that it undermines the inclusivity of mainstream and older-adult group fitness alike.
Depending on the training of the instructor, older adults attending both mainstream and older adult-specific group exercise programming can receive different directives as to what constitutes safe movements, as was evident in the examples above. This dichotomy arises from the tension between the application of health and ability-based criteria or age-based criteria to contraindications that arises from lack of consensus among certifying bodies and their curriculum. Take Exerciser 3, who questioned if they should ‘show off’ their (flex)abilities in front of their older peers:
Me, I can bend over and put my hands flat on the floor still. So, and I tend to do that to stretch my back, and I sometimes think maybe I shouldn't be doing that, occasionally, around everybody else that's older. Can a lot of people do that? But to me, that feels great. So, and it's a flexibility I still have.
Exerciser 3 attended a SilverSneakers® class, and as such the stretch they describe would be contraindicated, thus limiting what ‘feels good’ to Exerciser 3's body. Their (flex)abilities are thus limited during the class based on age alone, leading them to probe the appropriateness of their actions.
Instructors’ adherence to the application of age-based contraindications not only subordinate instructors’ professional competence, but fail to account for exercisers’ agency. For instance, Instructor 6, as per their SilverSneakers® training, tells participants, ‘Keep your head above your heart.’ However, that did not stop an older exerciser in the class from defying Instructor 6 and fully bending to touch her toes, like Exerciser 3. Consequently, exerciser agency can undermine the best intentions of ensuring safety by employing broad contraindications. Furthermore, we argue that applying contraindications to only those in the class for whom those contraindications are appropriate offers teachable moments that can serve to either reassure older exercisers that the exercise is appropriate for them to perform, or educate older exercisers to avoid movements that undermine their safety. So rather than cueing, ‘Keep your head above your heart’, Instructor 6 could have cued ‘Keep your head above your heart if you suffer from x, y, or z’, in order to respect the agency of older exercisers.
Indeed, older exercisers seemed to prefer instructors to apply contraindications to only those in the class for whom those contraindications are appropriate:
If you have an issue, like I said someone has an issue with their shoulder, ‘Okay but watch your shoulder. Now pick up weights.’ So, [the instructor] educates us really in things that we should or shouldn't do, you know if we are limited. So, [the instructor] does talk about limitations and that, if you – she doesn't point anybody out, but like ‘If you have this, remember you can't do this’, so she does educate us in what we can and can't do and that's important. (Exerciser 4)
This approach that Exerciser 4 described requires a higher degree of competence on the part of instructors, but results in greater inclusivity. It is also in this instance where it becomes apparent that instructors’ application of ability-based criteria not only teaches exercisers how to modify appropriately given their health-based limitations, thus creating inclusive exercise environments aligned with the notion of teaching multi-level classes, but also overcomes the inherent ageism of widely implementing age-based contraindications.
Discussion
What this study adds to this literature is a map connecting the material and the discursive. Herein, it is evident that the actions that take place in the group exercise encounters are highly governed by the ruling relations emanating from the governing bodies that certify group exercise instructors. Such actions remain largely invisible to the older exercisers who are the intended beneficiaries of such policies. Policy and practice decisions, such as decisions made to label certain exercises as contraindicated for all older exercisers attending age-exclusive classes, become embedded in the curricula written by these certifying agencies as rules that (re)produce exclusion and the decline narrative of ageing (Gullette, Reference Gullette1997). Echoing previous literature, this present study advocates that age-based criteria without consideration of ability is ageist and problematic, in that it conflates age and ability (Kluge and Savis, Reference Kluge and Savis2001).
Instructors in this study who resisted such potentially exclusionary practices did so by using their professional competence in order to employ relativist criteria by applying contraindications only where appropriate. Older exercisers in this study expressed a preference for this approach, which not only respected exercisers’ autonomy, but taught exercisers vital lessons on how to adapt exercises to fit their bodies. However, instructors who fail to abide by the rules of their certification can lose their certification or be legally liable for resultant injuries. Unfortunately, once certified, quality assurance is in the hands of the instructor's employer. Most certifying bodies do not continue to evaluate instructors after they are certified; instructors remain certified if they continue to submit continuing education credits and pay dues to their certifying body. In addition, many instructors possess multiple certifications. This is significant, because as this study demonstrates, the contraindications across certifying bodies vary. The lack of consensus regarding contraindication best practices is thus problematic for practice as what is acceptable by one certification's standards might be contraindicated by another.
Certifying bodies were not the only influence affecting the interactions between exercise instructors and older exercisers. This research revealed that employer policies could undermine practices promoted by the certifying curricula. For example, screening, touted by the curricula to engender participant safety, was highly influenced by employer policies and practices. Screening, and other employer-based bureaucratic practices, were described as taking considerable time, which for some instructors served as barriers towards pro-social aims. Importantly, this could interfere with instructors’ efforts to create community-oriented physical cultures, which are known to contribute to inclusive physical cultures (Tulle and Dorrer, Reference Tulle and Dorrer2012). Additionally, instructors recognised that these screening tools were static and failed to capture the dynamic nature of working with older exercisers. These instructors spoke about employing informal screening before and during classes to gauge exercisers’ capabilities in daily practice, as well as engaging in multi-level teaching.
In order to engender inclusivity, certifying bodies recommend multi-level teaching, but the social process of group exercise delivery to older adults is more nuanced than training curricula suggest. Previous research has found that adapting exercises to support exercisers’ limitations does indeed foster inclusivity (D'Abundo, Reference D'Abundo2007; Nau et al., Reference Nau, Nolan and Smith2021), but our research suggests that multi-level classes may not adapt enough to foster inclusivity. Pitfalls not overcome by multi-level teaching include: (a) when exercisers mirror what the instructor demonstrates and thus fail to modify or customise the exercise to their abilities; and (b) when the abilities of the exercisers comprising the group are exceedingly heterogeneous. As Exerciser 2 suggested, ‘if you're struggling with introductory to algebra, you don't want to sit in the calculus class’; hence, some of the shortcomings of multi-level teaching may be overcome by stratifying group exercise classes by ability, whilst still continuing to employ multi-level options.
Regrettably, the fitness industry is not clearly stratified by ability. To appeal to older consumers, and thus increase the number of physically active older adults, it has been said that the exercise market has been divided by age into mainstream fitness and older adult fitness, with older adult fitness emerging in response to older adults’ unique health and functional needs that could not otherwise be addressed in mainstream exercise classes (Ecclestone and Jones, Reference Ecclestone and Jones2004; Tulle and Dorrer, Reference Tulle and Dorrer2012; Massie and Meisner, Reference Massie and Meisner2019). Herein, mainstream fitness is said to emphasise performance and competition whilst older adult fitness emphasises health and function (Gilleard and Higgs, Reference Gilleard and Higgs2013). This notion is aligned with the dichotomy of either decline or success and overlooks physical activity for pleasure (Phoenix and Orr, Reference Phoenix and Orr2014). Scholars have argued that this division not only validates the exclusion of older adults from the more youth- and competition-oriented mainstream physical cultures, but the meaning of such a division has been observed to be internalised by older adults and used as a strategy to justify less-intense engagement with physical activity (Tulle and Dorrer, Reference Tulle and Dorrer2012; van Dyk, Reference van Dyk2014).
The health-oriented culture exclusively targeting older adults ignores the heterogeneity of this segment of the population. Excluded herein are masters athletes, who engage in competitive athletics, and older adults embodying fourth-age characteristics, such as frailty, and for whom even fitness interventions targeting older adults are too vigorous (Dionigi, Reference Dionigi2006; van Dyk, Reference van Dyk2014; Higgs and Gilleard, Reference Higgs, Gilleard, Tulle and Phoenix2015; Massie and Meisner, Reference Massie and Meisner2019; Clarke et al., Reference Clarke, Currie and Bennett2020). The range of abilities that older adults possess is more heterogeneous than is represented in these curricula and, as such, large portions of the older adult populace are excluded from the practice recommendations rooted in these texts. Therefore, the creation of older adult-specific exercise classes may indeed foster a more inclusive physical culture for some older persons, but this is at the exclusion of many older adults whose ranges of abilities are not well-suited to these programmes. Moreover, age-segregated, as opposed to ability-segregated, group exercise classes overtly exclude younger adults whose needs and abilities might be better addressed in an older-adult fitness class (or more aptly named a low-impact fitness class), as was described by Instructor 6 above. These younger individuals might not want to be identified as ‘old’ by being part of a social group devoted to older persons (Dionigi, Reference Dionigi2006). Therefore, we argue that exercise classes stratified by ability might create more fitness opportunities for persons of all ages and abilities.
The problematic identified here, of conflating age with ability, ignores non-health-related reasons for exercising, such as for pleasure (Poole, Reference Poole2001; Phoenix and Orr, Reference Phoenix and Orr2014; McPhate et al., Reference McPhate, Simek, Haines, Hill, Finch and Day2016), socialisation (Tulle and Dorrer, Reference Tulle and Dorrer2012; McPhate et al., Reference McPhate, Simek, Haines, Hill, Finch and Day2016) and serious leisure (Stebbins, Reference Stebbins2007; Palmer et al., Reference Palmer, Bowness and Tulle2021). The notion of physical activity careers was proposed to overcome this problem by advocating for physical cultures that embrace a myriad of discourses which would resonate with the heterogeneous meanings older adult ascribe to physical activity (Palmer et al., Reference Palmer, Bowness and Tulle2021). We echo this notion by calling for greater consideration of the ways in which physical cultures could become more inclusive by embracing social- and meaning-oriented approaches to exercise and physical activity.
Limitations
IE, although touted to be emancipatory (Campbell and Gregor, Reference Campbell and Gregor2004; Smith, Reference Smith2005), has been criticised for objectifying the ‘subject’ of analysis (Walby, Reference Walby2007: 1017), which in this study would be older exercisers. The authors acknowledge that, despite trying to centre the analysis on the experiences expressed by the older exercisers who participated in this study, the informants’ experiences might not be shared by all older adults. Thus, by keeping the subject of analysis focused on the material practices that have a downstream effect on the exerciser, we aimed to reveal the tensions and contradictory professional practices that have the potential to affect older adults who participate in group exercise. This research alone cannot emancipate older adults from the power enacted by ruling relations, but can serve as a means for consciousness raising (Freire, [Reference Freire1970] 1993).
The focal point of IE analysis is mapping or recording the ways in which social processes related to the embodied experience of a phenomena are organised by the aforementioned ruling relations (Campbell and Gregor, Reference Campbell and Gregor2004). The end product, rather than theory, is explication, wherein one illuminates the hidden forces governing the embodied experience under scrutiny (Campbell, Reference Campbell and Smith2006). IE's findings are, therefore, empirical, but subjective and thus lack generalisability outside the specific institutions under investigation (Campbell and Gregor, Reference Campbell and Gregor2004; Smith, Reference Smith2005). Thus, this research neither makes claims to contribute to social theory, nor is it generalisable to other group exercise instructor certifications. Moreover, influences of power cannot be mapped comprehensively (Smith, Reference Dionigi2006), as IE ‘is, in principle, never completed in a single study’ (Smith, Reference Smith and May2002: 30). Therefore, further inquiry that extends the scope of this IE, such as investigating the experiences of younger adults whose abilities are not well met by mainstream fitness, is needed.
Conclusion
The aim of this study was to apply an IE approach to elucidate the socio-cultural discourses that are represented in the training and workplace policies that govern how exercise instructors conceptualise and deliver older-adult exercise programming. In so doing, we explicated some of the ways in which these curricula, and the ideologies they espouse, are enacted by group exercise instructors to engender (in/ex)clusive social exercise environments. Specifically, this study reveals the problematic conflation of age and ability in fitness and physical cultures, and how the discourse of multi-level teaching, as a means of producing inclusive physical cultures, perpetuates norms regarding ability and health that exclude many potential exercisers. Indeed, the we found that the fitness industry's attempt to create inclusive group fitness classes produced age-exclusive exercise markets that conflate age and ability, thus upholding the decline narrative by equating youth with health and ability, and older age with disease and disability. The standpoint of older exercisers reveals the importance of ability-based criteria; therefore, we argue that, in order to be more inclusive, there is a greater need for physical cultures that cater to a greater range of abilities.
Acknowledgements
The authors would like to thank and acknowledge Dr Gavin Andrews (McMaster University, Canada) and Dr Miya Narushima (Brock University, Canada) for their feedback on an early draft of this article.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
Ethics was approved by McMaster University's ethics board.



