


More than four million African Americans were emancipated by the end of the Civil War. Even though Reconstruction ushered in hopes for political and economic progress, African Americans continued to experience the crushing reality of racism, poverty, and labor exploitation (Ayers Reference Ayers2007). Southern blacks faced daunting challenges and struggled to reinvent themselves in the face of new economic realities and increasing racial violence. For those who remained in rural areas, they found that the war had devastated the infrastructure and the southern economy. Although they were no longer enslaved, impoverished African Americans were faced with negotiating labor contracts, often with the men who once owned them. For those who left farming behind, their migration transformed southern cities as black institutions and neighborhoods emerged. The Great Migration (1916–1970) reshaped U.S. demography, but many of its defining characteristics had arisen decades earlier (Ayers Reference Ayers2007:151–152). In towns and cities, these migrants and their descendants encountered racial discrimination in housing and employment.
Archaeological research has addressed the lifeways of freed African Americans and their descendants within the context of structural racism and economic subjugation in both urban and rural contexts (e.g., Barnes Reference Barnes2011; Davidson Reference Davidson2004; Wilkie Reference Wilkie2003). Although related research in bioarchaeology has been on the rise, post-emancipation black experiences remain relatively unexplored (Blakey and Rankin-Hill Reference Blakey, Rankin-Hill, Zuckerman and Martin2016:111). Still, inroads have been made in addressing racial disparities in illness and trauma (de la Cova Reference de la Cova2010, Reference de la Cova2011; Thompson Reference Thompson2017) and the complexities of health status among people of African descent (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002; Rankin-Hill Reference Rankin-Hill1997, Reference Rankin-Hill, Zuckerman and Martin2016; Vanderpool and Turner Reference Vanderpool and Turner2013; Watkins Reference Watkins2012). What these studies have in common is an emphasis on difference: “rather than pointing to a common experience of disenfranchisement, these studies highlight variation within and between these populations resulting from different social and biological responses to these constraints” (Watkins Reference Watkins2012:22). With this in mind, our objective is to consider the relative quality of life of African Americans from a bioarchaeological perspective.
Notably, we situate our research within the bioanthropology literature that defines race and gender as social constructs and the studies that emphasize the role of racism in health outcomes (Blakey Reference Blakey2001; Blakey and Rankin-Hill Reference Blakey, Rankin-Hill, Zuckerman and Martin2016; Geller Reference Geller2008; Goodman Reference Goodman, Zuckerman and Martin2016; Rankin-Hill Reference Rankin-Hill1997, Reference Rankin-Hill, Zuckerman and Martin2016; Watkins Reference Watkins2012). Thus, our study is not embedded in biological notions of racial and sexual differences, and we stress the “lived experiences of discrimination” (Goodman Reference Goodman, Zuckerman and Martin2016:71) in our interpretations of health and longevity. Although race is socially constructed, historically people of African descent have experienced poorer health than whites, even when controlling for socioeconomic status (de la Cova Reference de la Cova2011; Kuzawa and Gravlee Reference Kuzawa, Gravlee, Zuckerman and Martin2016). A related goal, therefore, is to contribute to the existing scholarship on the biological consequences of anti-black racism.
In this article, we consider what the health and longevity implications were for those who remained in rural areas as opposed to those who left for the city. We address the urban penalty thesis that claims that infectious diseases and the difficulties of city life led to rural–urban disparities in morbidity and mortality (Haines Reference Haines2001). Bioarchaeology has the potential to complicate this generalizing framework, however. Research on African Americans reveals health variations between urban populations where socioeconomic context is implicated in well-being (Watkins Reference Watkins2012). Davidson and colleagues (Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002:273) compared the data from the urban Freedman's Cemetery with the rural Cedar Grove Cemetery and concluded that the health status of these two populations was similar, a finding that challenges the urban penalty argument. We expand on this research by including osteoarchaeological data from additional rural cemeteries. We address whether urbanites paid a steep penalty in their quality of life relative to African American agricultural laborers. Alternatively, did racial inequality lead to equally poor health, regardless of where African Americans settled? We also address black women's health. Their household-related and extra-domestic labor were integral to the well-being of their families (Battle-Baptiste Reference Battle-Baptiste2011; Jones Reference Jones2009; Teague and Davidson Reference Teague, Davidson and Barnes2011; Wilkie Reference Wilkie2003). Not only having and rearing children but also taking on “othermothering” roles in caring for people (Collins Reference Collins2000), black women assumed a tremendous burden.
Our biocultural study includes sites in Alabama, Tennessee, Arkansas, and Texas. We refer to these states as part of the South based on their legacy of slavery and former Confederate status (Ayers Reference Ayers2007:3–5). We begin with an overview of the sites and their historical context. We then address rural versus urban mortality and the related data for stress, taking account of disease, living conditions, and diet in our interpretations. The evidence reveals that there were rural children who suffered from similarly adverse conditions as urban children. For those who survived to adulthood, however, early life stressors and continued residence in the city led to reduced longevity. A discussion of work-related stress and osteoarthritis follows. We then focus on black women and posit that their working and reproductive lives are implicated in their higher midlife mortality and reduced longevity in comparison to black men. The overall results of this study illuminate how racism and poverty detrimentally affected African American health.
Cemetery Case Studies
The urban (Freedman's Cemetery) and rural cemeteries (Elko Switch, Foster, Ridley Graveyard, Cedar Grove, and Providence; Figure 1; Table 1) selected for this study were excavated as cultural resource management projects, and none of our data are original. We hope to raise the visibility of a valuable yet underused source of data for African American bioarchaeology. The politics surrounding historic cemetery preservation should impress on researchers the importance of considering what is already available for study (Figure 2). We surveyed more than 30 cemetery projects and chose the best comparative samples available based on time period, site location, preservation, and comparability of data reporting. Still, there are limitations of the data and reporting that we address later. A total of 1,623 burials were identified, and we include 1,529 individuals in our analyses (Table 2).

Figure 1. Cemetery site locations.

Figure 2. David Newton's Dream of Freedom sculpture, Freedman's Memorial Park and Cemetery (photo courtesy of Dallas native, Diana Petterson, and used with permission).
Table 1. Sites Examined in this Study.

Notes: For Freedman's Cemetery, there were 1,157 individuals buried in 1,151 graves. One burial, containing one individual, cannot be phased and is excluded from all analysis. For Cedar Grove, 80 individuals were interred in 79 graves.
a Number of human burials identified.
b Number of burials excavated.
c Number of burials with no human remains.
Table 2. Sex and Age Distribution by Site.

Of the cemeteries considered here, the urban Freedman's Cemetery has been the most extensively researched (Condon et al. Reference Condon, Becker, Edgar, Davidson, Hoffman, Kalima, Kysar, Moorehead, Owens and Condon1998; Davidson Reference Davidson2004; Peter et al. Reference Peter, Prior, Green and Clow2000). Until 1902, it was the only Dallas cemetery designated for African Americans, and thus it served various neighborhoods. The communities associated with the rural cemeteries mainly comprised farm laborers (Buchner et al. Reference Buchner, Breitburg, Williams and Williams1999; Oster et al. Reference Oster, Weaver, Richardson and Wyatt2005:7; Shogren et al. Reference Shogren, Turner and Perroni1989; Thompson Reference Thompson2009:19–20; Watkins Reference Watkins and Rose1985; Wilson Reference Wilson2005:17). The Cotton Belt, which extended from Maryland to Texas, included Tennessee, Arkansas, and Alabama, and these states had some of the highest rates of U.S. cotton production. Residents in each of these close-knit communities attended the same churches and schools (e.g., Buchner et al. Reference Buchner, Breitburg, Williams and Williams1999:41–45; Watkins Reference Watkins and Rose1985). For instance, Baptist churches founded both Cedar Grove and Providence cemeteries (Oster et al. Reference Oster, Weaver, Richardson and Wyatt2005:20; Rose Reference Rose1985). Social ties were also engendered through shared connections with place and the legacy of plantation slavery. People interred at Cedar Grove and Ridley had continued to labor on nearby plantations after emancipation (Buchner et al. Reference Buchner, Breitburg, Williams and Williams1999: 45–48; Watkins Reference Watkins and Rose1985:11–12). Similarly, Elko Switch and Foster cemeteries are located on grounds once owned by slaveowners (Shogren et al. Reference Shogren, Turner and Perroni1989:273; Thompson Reference Thompson2009:19–20). Black communities made up of sharecroppers were still present near Elko Switch during the twentieth century (Shogren et al. Reference Shogren, Turner and Perroni1989:245, 283). At Foster, the earliest burials were likely those of sharecroppers, yet the nearby presence of a post-1900 textile mill indicates that more recent interments may be those of mill workers (Thompson Reference Thompson2017:535).
We established a chronology of the sites consisting of three major periods for the analyses related to childhood morbidity and mortality (Figure 3). A primary consideration in devising this sequence was to ensure that rural samples were available for comparison with Freedman's. The results are imperfect, because there are unavoidable temporal overlaps and phasing for Foster Cemetery is not available.

Figure 3. Sites by time period with number of individuals indicated for each interment phase (Elko Switch, Freedman's, Ridley) or time span (Foster, Providence, Cedar Grove).
There are limitations inherent in the data and characteristics of the cemetery populations that will influence our results. About 30% of individuals were born enslaved; a few of the Elko Switch burials may date to slavery. Thus, some of the data relate to conditions under slavery. Migration also shaped demographics: young people tended to migrate to cities, whereas older people remained in rural areas. To some extent, our comparisons of urban–rural mortality reflect this migration pattern.
Sampling and taphonomic issues might also bias our results. In terms of sampling, at Providence only 24% of the cemetery was excavated, as part of an expansion of the Memphis airport. Other sites were also partly excavated: at Freedman's, 24% of the burials were disinterred; at Elko Switch, about 35%; at Cedar Grove, approximately 63%; and at Ridley, 75%. The percentage of unexcavated Foster burials was not reported. These partial excavations could have a large impact if children were buried in separate areas. In most of these cemeteries, however, children were located amidst adult interments, probably in family groupings (e.g., Oster et al. Reference Oster, Weaver, Richardson and Wyatt2005:38–39; Shogren et al. Reference Shogren, Turner and Perroni1989:225). The exception is the Ridley Graveyard, where discrete clusters of children were buried (Buchner et al. Reference Buchner, Breitburg, Williams and Williams1999:201). Skeletal preservation was also a problem, and we were cautious regarding possible preservation bias in the representation of children, women, and the elderly (Walker et al. Reference Walker, Johnson and Lambert1988). This was especially an issue for Foster Cemetery, where 96 of 223 burials had no (n = 73) or very poorly preserved (n = 23) skeletal remains; the researchers did not estimate age by coffin size there. Poor skeletal preservation was also observed for the Ridley Graveyard and Elko Switch.
With regard to reporting, it was difficult to compare qualitative observations of pathologies and the methods used for age assessment across the site reports. For Freedman's and Cedar Grove, stress markers were reported using the Western Hemisphere Data Coding Scheme, which standardized the data (Goodman and Martin Reference Goodman, Martin, Steckel and Rose2002). Reporting for other sites used slight/mild, moderate, and severe or alternative descriptions. For the purposes of intersite comparison of skeletal pathologies, we generally relied on a criterion of presence or absence. Because population demography is central to our analyses, the methods that researchers used to estimate age are important. At Freedman's, Cedar Grove, and Providence (Condon et al. Reference Condon, Becker, Edgar, Davidson, Hoffman, Kalima, Kysar, Moorehead, Owens and Condon1998:xiv; Oster et al. Reference Oster, Weaver, Richardson and Wyatt2005; Rose Reference Rose1985), researchers used an array of techniques. For subadults, these included analysis of dental eruption and calcification, growth of long bones, epiphyseal unions, and endocranial suture closures. For adults, changes to the pubic symphyses and articular surfaces of the ilia were measured, as well the deterioration of sternal rib ends and dental wear. This same battery of techniques was cited for Foster (Thompson Reference Thompson2009:34–38), although only a subset may have been used in some cases because of poor skeletal preservation. For Ridley, researchers were able to determine sex and age for 47 individuals (Buchner et al. Reference Buchner, Breitburg, Williams and Williams1999:211–216), yet were not specific on the methods used, stating that “metric and nonmetric observations gathered from the preserved portions of the skeletons were used to determine sex, age, stature, genetic affinity, and pathologic condition” (Buchner et al. Reference Buchner, Breitburg, Williams and Williams1999:212). Likewise, for Elko Switch, the report does not specify the dental and skeletal criteria used to arrive at age estimates (Shogren et al. Reference Shogren, Turner and Perroni1989:37–88, 196, 192). In the absence of human remains, the estimated ages for subadults buried at Ridley (n = 2), Providence (n = 3), Elko Switch (n = 20), and Freedman's (n = 53) were based on the size of the grave shaft, coffin remains, or both, a technique often used by bioarchaeologists working on historic cemetery populations (Condon et al. Reference Condon, Becker, Edgar, Davidson, Hoffman, Kalima, Kysar, Moorehead, Owens and Condon1998:67; Jantz and Wilson Reference Jantz, Wilson, Oster, Weaver, Richardson and Wyatt2005:Appendix 1, 89–94; Shogren et al. Reference Shogren, Turner and Perroni1989:191–196). Individuals who could only be placed in categories of longer than 10 years were not used in our demographic estimates. Still, the lack of specifics for age assessment methods for Elko and Ridley raises the possibility that our observed differences for age-at-death are due in part to the use of different techniques to assess age.
Biological sex (based on pelvic and cranial traits) was assessed using methods that are now called into question because of how they assume a male–female binary and conflate sex and gender (Geller Reference Geller2008). More recent sex assessment approaches in feminist bioarchaeology decouple sex and gender, problematize sex and gender categories, and refrain from imposing preconceived ideas about social difference onto the past (Agarwal and Wesp Reference Agarwal and Wesp2017). This literature emphasizes that data organized by binary sex do not fully capture the embodied experiences of people that are reflected in the skeletal record (Zuckerman and Crandall Reference Zuckerman and Crandall2019). There is the possibility, for example, that an individual's gender presentation may conflict with the assigned sex. Although space does not permit elaboration on these issues, these positions inform our use of the terms “men/women” in place of “males/females” in this article. This usage aligns with how African Americans were socialized into dichotomous gender roles that are documented in the historical record. Further, it allows us to address the health-related consequences of being interpellated by others as raced and gendered persons.
Finally, the “osteological paradox” is relevant to this research (Wood et al. Reference Wood, Milner, Harpending, Weiss, Cohen, Eisenberg, Hutchinson, Jankauskas, Česnys, Katzenberg, Lukacs, McGrath, Roth, Ubelaker and Wilkinson1992). Skeletal pathologies related to chronic stress take time to develop and are often found among people who survived illness, malnutrition, or both. In contrast, the diseases that led to rapid death usually leave no skeletal traces. Thus, the mortality and longevity data proved instrumental in interpreting quality of life, because there were instances in which the evidence for pathologies alone might have suggested that health conditions were better than they actually were.
Historical Context
A biocultural approach to interpreting the past considers how biology and culture interrelate. Blakey (Reference Blakey2001:409) explains that such an approach “combines cultural and social formation with the demography and epidemiology of archaeological populations to verify, augment, or critique the socioeconomic conditions and processes experienced by past human communities.” It follows that a biocultural framework hinges on interpreting human remains by careful consideration of their historical context (Geller Reference Geller2008:128), which we discuss next. Further insights into work, diet, living conditions, and the disease environment are provided as our interpretations unfold.
Agricultural Lifeways in the Rural South
Our rural populations were composed mostly of tenant farmers and sharecroppers. Emancipation introduced new labor relations between landowning whites and freedmen that prevailed well into the twentieth century. Few blacks were able to purchase land (Hersey Reference Hersey and Haggard2010:135); the majority were stuck on the lower rungs of a farming hierarchy known as the “agricultural ladder” where they labored under contract (Figure 4; Alston and Kauffman Reference Alston and Kauffman1998:266–268; Burton Reference Burton1998:221–222, 224; Hersey Reference Hersey and Haggard2010:136). African Americans were exploited by the crop lien system in which landowners provided seed and tools; in turn, farmers promised more of their harvest as repayment. Faced with high interest rates, black farmers rarely retained much of their crop. Further, merchants and plantation owners (often one and the same) operated stores and sold food to agricultural workers at inflated prices (Dirks Reference Dirks2016:50).

Figure 4. Children of a sharecropping family in Montgomery County, Alabama, 1937 (photo courtesy of Library of Congress [Digital ID fsa 8b35934]).
The transition in labor arrangements also led to changes across the plantation landscape. With tenancy and sharecropping, plantation owners broke up large swathes of land into plots. Families abandoned the former slave quarters and resettled on the plots they worked (Penningroth Reference Penningroth2003:81–82). This dispersed settlement pattern retained the social dynamic that African Americans were familiar with, as kin-related households resided in small enclaves (Elman et al. Reference Elman, London and McGuire2015). Importantly, under freedom, parents claimed the labor of their children, who played important roles in farming and in the household economy (Jones Reference Jones2009:84).
Several observations have implications for our interpretations of the evidence. First, tenants and sharecroppers struggled to maintain the balance between producing cash crops and raising their own food (Wilkison Reference Wilkison2008). The skeletal pathologies indicate that farmers had varied levels of success with household production in their attempts to meet landowners’ demands for cotton planting. Second, the low population density of farmsteads proved to be important in reducing exposure to infectious diseases and leading to greater longevity among farmers. Third, rural families tended to be large, because children contributed to agricultural work (Elman et al. Reference Elman, London and McGuire2015). Spreading the labor among family members helps explain the rural–urban disparity in osteoarthritis discussed later.
African Americans in Dallas
For African Americans who sought to escape from farming, migration to cities proved the rule. In Dallas, they encountered job insecurity, poor living conditions and sanitation, and exposure to infectious diseases. Bioarchaeological studies of urban populations demonstrate how these factors, when combined with rapid population growth, led to high mortality rates and skeletal pathologies related to chronic stress (Buzon et al. Reference Buzon, Walker, Verhagen and Kerr2005; Grauer et al. Reference Grauer, Williams, Bird, Zuckerman and Martin2016).
Founded in 1841, Dallas was a small agricultural town that witnessed an increase in its black population right after the Civil War. Freedmen arrived seeking lost family members and refuge from sharecropping. In 1869, they established Freedman's Town and its cemetery (Davidson Reference Davidson2004). The arrival of railways in the 1870s spurred the city's growth and economy, and other black enclaves soon emerged. Most African Americans held low-wage, unskilled, or semiskilled jobs (Engerrand Reference Engerrand1978:208). Men were mainly general laborers, porters, and teamsters, whereas women worked as domestics and laundresses (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002:260). Many black men were underemployed, which led to high numbers of their spouses entering the workforce (Engerrand Reference Engerrand1978:207; Jones Reference Jones2009:103–105).
By the turn of the century, Dallas was home to more than 42,000 people and still growing. The Dallas Morning News published articles on housing for the poor, which lacked “sanitary facilities, adequate privacy, or sunlight and air” (Fairbanks Reference Fairbanks2014:39). Most homes did not have running water, and outdoor, open privies were the norm. Poor Dallasites lived in small dwellings that were crowded together, leading to densely packed neighborhoods. These dire circumstances were largely the plight of African Americans (Galveston-Dallas News 1911:20–21).
With abolition and the Reconstruction Amendments, white southerners grew fearful that blacks’ political gains would diminish white supremacy. Thus, by the 1890s, southern states began to codify segregation through Jim Crow legislation. Further buttressed by the Supreme Court's 1896 decision in Plessy v. Ferguson, Jim Crow laws enforced racial discrimination in all manner of public places, including schools and restaurants. Hospitals were also segregated, and some refused to treat black patients altogether (Litwack Reference Litwack1998:233; Prather et al. Reference Prather, Fuller, Marshall and Jeffries2016:667). City ordinances and an “informal code of exclusion and discrimination” ensured that blacks of every class had no choice but to live in majority-black enclaves under abject living conditions (Litwack Reference Litwack1998:229, 235, 336–337). In urban and rural areas, the racial hierarchy was maintained by discriminatory hiring practices and by whites who refused to sell farmland to blacks. The inability to move up the agricultural ladder or secure decent jobs, poor housing conditions, and poor sanitation was implicated in African Americans’ morbidity and mortality (Prather et al. Reference Prather, Fuller, Marshall and Jeffries2016:667).
Adult Mortality and the Urban Penalty
Although this article focuses on African Americans, it is important to emphasize that there were significant racial disparities in mortality for our study period. In general, blacks died at younger ages than whites, and the U.S. mortality statistics underscore this point (e.g., Glover Reference Glover1921). In 1899–1900, 34% of blacks versus 30% of whites died before age five (U.S. Census Bureau 1901). In 1900, 67% of blacks died by age 30 versus 49% of whites. For all Americans, infant mortality was high, but black mortality peaked again for ages 20–30 (Figure 5). More whites died in their sixties and seventies, simply because more lived to that age. In 1900, life expectancy at birth was about 49 years for whites compared to 34 years for African Americans (Arias and Xu Reference Arias and Xu2018:Table 21).

Figure 5. U.S. census mortality profiles for 1900 by race, sex, and age-at-death cohorts.
With regard to our data, Dallas men and women interred at Freedman's Cemetery had lower mean ages-at-death and less longevity than their rural counterparts (Table 3). These Dallasites had high mortality between the ages of 25 and 40, and few lived beyond the age of 50 (Figure 6). The average age-at-death for Dallas adults was 34.6 years, compared to 40.8 for rural adults (Table 3), and this disparity holds across time. We compared the mean age-at-death for 170 rural adults (M = 40.8, SD = 14.2) with that of 565 urban adults (M = 34.6, SD = 9.3) using a two sample t-test and found the difference to be statistically significant: t(215.2) = −5.3, p = 0.0001. This difference in mean age, however, does not capture the considerable mortality disparities between these populations. That is, the mean does not reflect that the modal or peak age-at-death for adults in Dallas was 30–34, whereas for rural inhabitants it was age 50+ (Figure 6; a K-S test indicates that the distributions of age-at-death for rural and urban adults are significantly different: D[732] = 0.122, p = 0.0001).

Figure 6. Urban and rural adult mortality profiles with age-at-death for each age interval as a percentage of all deaths.
Table 3. Demographic Statistics for Urban and Rural Sites by Sex and Age.

a Percentage of individuals out of total number of urban or rural individuals where age assessment (for subadults) or age and sex assessments (for adults) was possible.
This rural–urban disparity relates to the urban penalty (Feigenbaum et al. Reference Feigenbaum, Muller and Wrigley-Field2019; Maeda Reference Maeda2018; Preston and Haines Reference Preston and Haines1991). Haines (Reference Haines2001:1–2) asserts that crowding, contagious diseases, polluted water and inadequate sewerage, and an influx of migrants newly exposed to the urban disease environment contributed to the “excess mortality of cities.” African Americans were disproportionately affected by the urban penalty (Costa and Kahn Reference Costa and Kahn2015). In her biocultural study of white and black males born during the late nineteenth century and who died in three U.S. cities, de la Cova (Reference de la Cova2011) found significant health disparities between these two groups. African Americans suffered from much higher rates of tuberculosis and treponemal disease. Because both these black and white men were indigent and unskilled laborers, socioeconomic status alone could not account for these disparities. Instead, the mostly southern-born blacks in her sample faced racial discrimination in migrating to northern cities that confined them to crowded tenements in areas with poor sanitation.
Tuberculosis was indeed a major cause of death among blacks (Thompson Reference Thompson2017). In addition, typhoid fever and diarrheal diseases caused nearly half of the deaths in cities related to infectious diseases (Cutler and Miller Reference Cutler and Miller2005:1–2). These were spread by contaminated drinking water and poor sanitation; in the warmer South wherever open privies dominated, such as in Dallas, fly-transmitted infections were common (Troesken Reference Troesken2004:18). Effective public health measures were implemented in the twentieth century at a time when less than half of households had filtered water and even fewer had sewer lines (Haines Reference Haines2001:12–13). A large portion of Dallas's drinking water came from the Trinity River, referred to as the “mythological river of death,” given its link to typhoid fever cases and contamination from slaughterhouses (Trinity River Authority of Texas 2019; U.S. Department of Commerce 1916:42, 146). Dallas did not adequately treat its water supply until 1914, yet many black Dallasites still lacked running water by 1925 (Fairbanks Reference Fairbanks2014:39; U.S. Department of Commerce 1916:43, 45, 146, 156).
Dallas's population experienced epidemics that might have affected our mortality data, including outbreaks of smallpox in 1882 and 1889 and of cholera and scarlet fever in 1892 (City of Dallas Health Department 1870–1975). Census records from 1880 to 1920 record the continuous impact of these diseases, along with typhoid fever, influenza, and malaria (U.S. Census Bureau 1881, 1891 1901, 1921). For children, diarrheal diseases such as cholera infantum, dysentery, enteritis, and typhoid fever were the deadliest and were responsible for more than half of infant deaths in 1900 (Wilcox Reference Wilcox2008).
The low-density, dispersed settlement pattern among farmers mitigated against water contamination and the spread of diseases (Haines Reference Haines2001:7). Instead, mosquito-borne malaria was endemic in the rural South until the 1930s (Humphreys Reference Humphreys2009). Malaria was strongly associated with rural impoverishment, and all of the rural cemeteries were located in malarial areas. In the United States, 600,000 cases were reported in 1914 (Sledge and Mohler Reference Sledge and Mohler2013), yet the death rate was low (CDC 2012). Still, persons infected were lethargic, and agricultural productivity slowed as a result (Sledge and Mohler Reference Sledge and Mohler2013).
African American Childhood Health and Mortality
Assessing children's health status is important for evaluating the health of their communities, because they are more susceptible than adults to disease and malnourishment. Moreover, malnutrition and illness in early life can have cumulative, long-term effects on adult morbidity and longevity (Beauchesne and Argawal Reference Beauchesne and Agarwal2018). For African Americans, the “wear and tear” of racism also detrimentally affected their health over the course of their lives, a concept referred to as “biological weathering” (Goodman Reference Goodman, Zuckerman and Martin2016; Kuzawa and Gravlee Reference Kuzawa, Gravlee, Zuckerman and Martin2016). Thus, the evidence for childhood stress we present indicates that adults who survived it remained at greater risk for illness and reduced longevity. The data for adult mean age-at-death and longevity, especially for Dallasites (Table 3), support the idea of weathering.
For the six cemetery populations together, 36% of children never lived to age five, compared to 30% for white children (U.S. Census Bureau 1901), supporting the claim that race was the “most important variable in predicting child mortality” (Preston and Haines Reference Preston and Haines1991:209–210). “Size of place” (low- versus high-density areas) is cited as the second important factor for predicting child mortality (Preston and Haines Reference Preston and Haines1991:174, 210). Yet, when the data for stress and child mortality are compared over time and by site, a more complex narrative of children's well-being emerges.
There are two patterns in Figure 7. First, there are very similar urban–rural mortality rates for the early and middle periods, during which half of those interred were under the age of five. Second, for the late period, mortality rates varied for rural children, with rates in Ridley and Cedar Grove surpassing that of Freedman's. Thus, rural childhood conditions were not altogether healthy. We also note that taphonomic issues meant that 57% of the Foster burials were excluded, leading to a potential underrepresentation of children. The variations in rural child mortality are also evident in the markers for childhood chronic stress.

Figure 7. Child mortality (under the age of five) by time period and site.
Linear Enamel Hypoplasia and Early Life Stress
We consider the data for linear enamel hypoplasia (LEH), a nonspecific indicator of stress, to help explain the findings related to child mortality. Enamel hypoplasia refer to enamel defects that appear as grooves across the surface of teeth, indicating periods when enamel formation was disrupted by disease or malnutrition (Blakey et al. Reference Blakey, Leslie and Reidy1994). When this defect is present in the permanent incisors and canines, it points to stress between the ages of six months to six years (Goodman and Armelagos Reference Goodman and Armelagos1985; White and Folkens Reference White and Folkens2005). There are two observations for the LEH data: an increase in the rate of hypoplastic teeth for both urban and rural children over time and, for the late period, variations among rural populations in this pathology (Table 4).
Table 4. Enamel Hypoplasia (One or More Hypoplastic Teeth) by Period and Site.
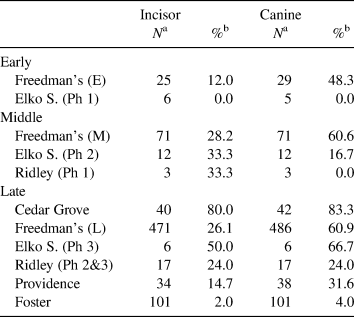
Note: Based on permanent dentition: maxillary or mandibular incisor or canine.
a Sample size.
b Expressed as percentage of individuals for whom this condition could be observed.
Dallas children experienced chronic stress across all three time periods, and the frequencies of hypoplastic teeth rose before 1900. For Elko Switch, enamel defect frequencies also increased over time. As the percentages of affected individuals rose, child mortality declined (Figure 7). This is likely an effect of the osteological paradox, with more children surviving stress to exhibit enamel hypoplasia. In the earlier period, children likely died from acute illnesses, malnutrition, or both before their permanent teeth erupted or enamel defects could form. For the late period, the different rates of hypoplastic teeth among rural inhabitants suggest variations in diet and environmental stress across these rural communities. Individuals interred at Cedar Grove, in particular, exhibited very high frequencies of enamel defects that implicate poor childhood conditions. Importantly, when considered by site, the child mortality rates and the LEH data do not suggest that the countryside was altogether healthier for children than the city.
Wide-scale public health measures were not implemented in Dallas until after Freedman's Cemetery closed. Thus, the decline in child mortality might be attributed to greater community stability toward the end of the century. For instance, churches, mutual aid societies, and fraternal lodges emerged in Freedman's Town (Peter et al. Reference Peter, Prior, Green and Clow2000) that helped residents weather conditions associated with impoverishment. Black doctors began to practice in Dallas during the 1890s (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002:272). Thus, African Americans made progress in instituting “cultural buffers” (Rankin-Hill Reference Rankin-Hill, Zuckerman and Martin2016:144–145) that probably had positive impacts on children's health. In rural areas, blacks continued to reside on familiar lands and lived in close proximity to extended family members and friends. Both factors would have alleviated some stress. Moreover, the midwives and mothers who routinely provided care work to community members, often relying on traditional medicinal practices, could have made a difference in improving child survival rates (Collins Reference Collins2000; Wilkie Reference Wilkie2003).
In general, Dallas children suffered from chronic illness, poor diet, or both over time, and there were rural conditions that were just as detrimental to children's well-being. We delve further into the health disparities between rural communities next.
Porotic Hyperostosis and Cribra Orbitalia
Porotic hyperostosis (PH) is a pathological condition that presents as porous lesions in the cranial vault; when evident in the orbital roof, it is called cribra orbitalia (CO; Brickley Reference Brickley2018:897). Porotic hyperostosis has different causes, including malnutrition, trauma, parasites, hemolytic anemias, and infectious diseases. The conventional explanation is that these lesions are the result of hemolytic or acquired iron-deficiency anemia (Blom et al. Reference Blom, Buikstra, Keng, Tomczak, Shoreman and Stevens-Tuttle2005; Brickley Reference Brickley2018). Walker and colleagues (Reference Walker, Bathurst, Richman, Gjerdrum and Andrushko2009:116), however, question iron-deficiency anemia as an etiology for PH and CO, stating that it fails to “stimulate the massive marrow hypertrophy necessary to produce these lesions” (but see Oxenham and Cavill Reference Oxenham and Cavill2010). Instead, they propose that megaloblastic anemia (dietary deficiencies and malabsorption of vitamin B12, folate, or both) is a proximate cause for PH (Walker et al. Reference Walker, Bathurst, Richman, Gjerdrum and Andrushko2009:112). The authors further suggest that megaloblastic anemia and scurvy (vitamin C deficiency) in particular, but also rickets and physical trauma, can result in the orbital porosities identified as CO (Walker et al. Reference Walker, Bathurst, Richman, Gjerdrum and Andrushko2009:115). The manifestations of CO and PH occur during childhood; in adults these lesions are usually healed (Blom et al. Reference Blom, Buikstra, Keng, Tomczak, Shoreman and Stevens-Tuttle2005:153; Brickley Reference Brickley2018). We introduce the data first and, for this study, note that CO and PH evince detrimental impacts on health that included anemia.
The data for CO and PH are presented in Table 5 (see Supplemental Table 1 for data by age-at-death). Only Freedman's Cemetery had large enough samples for the early and middle periods; thus, Elko Switch and the Ridley Graveyard are excluded. For Freedman's, the individuals initially affected with CO and PH were interred during the middle period; by the late period, a greater percentage of individuals were affected. For the rural samples, there are significant variations. Cedar Grove once again stands out with the highest CO and PH frequencies, whereas there are relatively few individuals affected in Providence and Foster. The synergistic effect of multiple factors is usually cited for PH and CO, and we consider diet, parasites, and disease (e.g., Blom et al. Reference Blom, Buikstra, Keng, Tomczak, Shoreman and Stevens-Tuttle2005).
Table 5. Frequencies of Cribra Orbitalia and Porotic Hyperostosis.
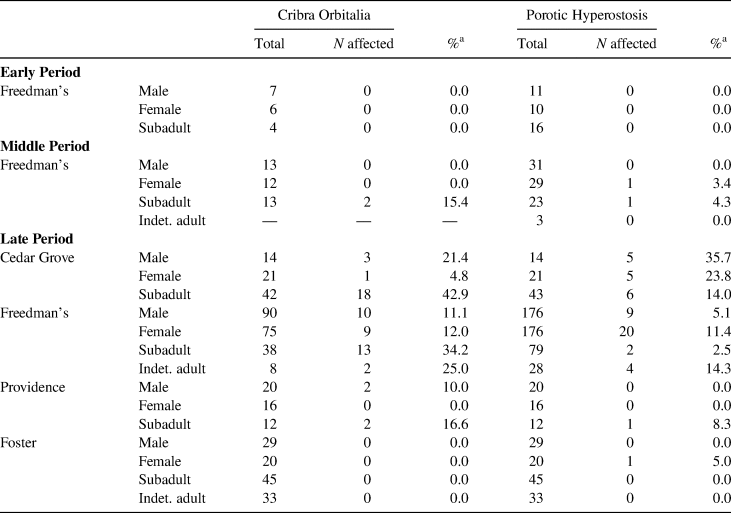
a Percentage of all measurable individuals in specified sex or age class.
The crop lien system and dietary differences are partially implicated in the variations of CO and PH among rural inhabitants. Landowners controlled the terms of the contracts signed with sharecroppers and often forbade them to raise livestock, an important source of vitamin B12 and iron. Grazing livestock on arable land reduced the amount of cash crops that could be grown; for example, the 1865 contract signed by Cedar Grove freedmen prohibited livestock raising (Watkins Reference Watkins and Rose1985:12). Most sharecroppers owned only a few hogs, and fresh pork was not a dietary staple (Dirks and Duran Reference Dirks and Duran2001:1882). Instead, impoverished southerners subsisted on pork fatback, molasses, and cornmeal, usually purchased on credit (Dirks Reference Dirks2016; Vanderpool and Turner Reference Vanderpool and Turner2013).
Although these foods are high in calories, sharecroppers often struggled to put food on the table (Ferris Reference Ferris2012:9). Moreover, although molasses is high in iron, a reliance on cornmeal was linked to pellagra, a common disease among poor southerners. Pellagra is caused by niacin deficiency and can result in diarrhea, dementia, and, in extreme cases, death. Incidence of the disease peaked in 1928, with 230,000 cases reported in the South (Clay et al. Reference Clay, Schmick and Troesken2019:32). According to her death record, Bell Cunningham, aged 26, died of pellagra and was interred at the Ridley Graveyard (Buchner Reference Buchner, Breitburg, Williams and Williams1999:Appendix B). Significantly, in cotton-growing regions, African Americans’ consumption of animal products decreased by half during the fall and winter, when income from farming ceased and food supplies were depleted (Dirks Reference Dirks2016:90–92). Eggs, a key source of iron, vitamin B12, and folate, also became scarce then. This annual pattern of food insecurity is tied to plantation tenancy and may have been experienced by Cedar Grove residents.
The low frequencies of CO and PH among individuals interred at Providence and Foster cemeteries suggest that they resided in communities with more successful household economies. As during slavery, African Americans after emancipation relied on a range of subsistence strategies to diversify and supplement their core diet of fatback, cornmeal, and molasses. Archaeological research has demonstrated that southern blacks fished and hunted wild game (Holland Reference Holland1990; Tuma Reference Tuma2006). Faunal remains associated with tenant farmers at Alma and Riverlake plantations in Louisiana confirm their consumption of fish, chicken, domestic turkey, duck, rabbit, and opossum (Palmer Reference Palmer2005:233–237)—all good sources of protein, iron, and vitamin B12. Plant-based foods, including leafy greens, provided folate and additional iron to the diet. Tenants who were able to keep a garden (many could not; Ferris Reference Ferris2012) typically raised collard or turnip greens, although they were only available in season.
If, as we suggest here, Cedar Grove residents experienced recurring food insecurity, a combination of malnutrition, diseases, and parasites would have elevated the risk of developing anemia, especially among the more vulnerable young. Malaria and hookworm infection can result in severe anemia, and both were endemic in the rural South. Researchers have demonstrated a link between malaria and CO and PH in archaeological populations (Gowland and Western Reference Gowland and Western2012). Both Cedar Grove and Providence cemeteries were located in counties at especially high risk for malaria (Hong Reference Hong2007). The hookworm is a parasite associated with poor sanitation, and most farmers used chamber pots or the outdoors (Ayers Reference Ayers2007:210; Wilkie Reference Wilkie2003:187–188). Because impoverished children in rural areas often went barefoot, they were prone to hookworm infection (Humphreys Reference Humphreys2009:1739).
Turning to Freedman's Cemetery, research on free blacks interred at Philadelphia's First African Baptist Church (FABC) cemetery (1822–1843) illustrates how city living elevated African Americans’ risk of illness and death (Rankin-Hill Reference Rankin-Hill, Zuckerman and Martin2016:144). Although this population was generally healthier than other blacks, the FABC skeletal series exhibited three patterns associated with African diasporic populations: high child mortality rates, episodes of malnourishment and infectious diseases, and high frequencies of osteoarthritis (Rankin-Hill Reference Rankin-Hill, Zuckerman and Martin2016:150). Racial segregation, rapid population growth, and substandard housing led to elevated chronic stress, as evinced by the porotic hyperostosis and hypoplastic enamel defects among individuals interred at the FABC cemetery.
The historical and bioarchaeological evidence for Freedman's Cemetery suggests similarities in conditions between this population and that interred at the FABC cemetery.
There was no evidence for CO and PH for the early period; frequencies of both sharply increased over time (Table 5); for CO, X 2(247) = 5.41, p = 0.02; for PH X 2(545) = 4.06, p = 0.04). This trend correlates with the city's rapid growth (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002). From 1880 to 1910, the population increased from 10,000 to 92,000. Although child mortality rates declined, blacks increasingly lived in higher-density neighborhoods and experienced worse living conditions. Their lack of filtered water and sanitary facilities and the prevalence of livestock roaming city streets meant greater exposure to diseases and parasites (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002:251; Fairbanks Reference Fairbanks2014). These conditions alone would lead to increased bouts of severe anemia, particularly among the young. Yet, impoverishment and the inability to raise food or hunt in the city meant that black Dallasites were also prone to malnourishment.
The data for CO reveal a shared pattern of poor maternal health, weaning practices, and gastrointestinal infections across the rural–urban divide. For Cedar Grove children between the ages of zero to three years, half (16 of 31) were affected with CO, whereas for post-1900 Freedman's, 30% (8 of 26) of children in this age group were affected (Supplemental Table 1). Bioarchaeologists have demonstrated how malnourishment in mothers not only compromised the health of the developing fetus but also infants nursed on breastmilk with low levels of vitamins B12 and C could develop megaloblastic anemia and scurvy (Newman and Gowland Reference Newman and Gowland2017:226; Walker et al. Reference Walker, Bathurst, Richman, Gjerdrum and Andrushko2009). Further, diarrheal diseases such as cholera infantum and dysentery were major causes of death among infants. Acute gastroenteritis can reduce the absorption of vitamin B12 (Walker et al. Reference Walker, Bathurst, Richman, Gjerdrum and Andrushko2009:115). During and after slavery, infants as young as four months were introduced to table foods (Blakey et al. Reference Blakey, Leslie and Reidy1994; Ewbank Reference Ewbank1987:117–118; Kiple and Kiple Reference Kiple and Kiple1977). These foods were mainly starchy paps made with fat, cornmeal, or hominy and mixed with water or milk (Steckel Reference Steckel1995:1924). These high-carbohydrate, low-protein weaning foods have been linked to scurvy, rickets, and anemias (Kiple and Kiple Reference Kiple and Kiple1977; Vanderpool and Turner Reference Vanderpool and Turner2013). Foods mixed with contaminated water or milk would cause diarrheal diseases. In Dallas, by 1907, the city's inspection of milk and dairies did not include testing for bacteria, and spoiled milk was a prime source of bacterial infections (Ewbank Reference Ewbank1987:117–118; Grauer et al. Reference Grauer, Williams, Bird, Zuckerman and Martin2016:212; McMillen Reference McMillen1985:342; U.S. Census Bureau 1910). Thus, the health of mothers and of young children interred at Cedar Grove and Freedmen's was compromised by malnourishment, poor sanitation, and diarrheal diseases (e.g., Walker et al. Reference Walker, Bathurst, Richman, Gjerdrum and Andrushko2009:118).
Using multiple lines of evidence, we arrived at several findings. First, there were rural conditions that were as detrimental to children's health as city living. This is supported by the data for stress and child mortality for Elko Switch, Ridley, and Cedar Grove. For rural children, variations in health and mortality rates were likely due to differences in diet, sanitation, and exposure to parasites and diseases. Although some of these rural samples are relatively small, comparing the data by site rather than as an aggregate proved essential in elucidating these variations. Finally, for those who survived to adulthood, Dallas men and women were at higher risk than their rural counterparts for midlife mortality and reduced longevity (Table 3). Thus, biological weathering and chronic stress in early life had a more adverse impact on Dallasites, especially when combined with their continued residence in the city, than on farmers.
Labor and Joint Disease
We compared the data for joint disease to discern whether urbanites and rural farmers differed in terms of work-related stress. Although a common approach is to reconstruct past activity patterns by assessing mechanical loading and repetitive tasks and their effects on different joint complexes (e.g., hip–knee), this line of inquiry is beyond the scope of this article. Instead, we considered the presence of moderate to severe osteoarthritis (OA). Because individuals become more prone to osteoarthritis as they age (Watkins Reference Watkins2012), we also determined the mean ages of those affected. If work-related stress was similar for both groups, we predicted that rural inhabitants would have higher OA frequencies, because they began farming at an early age and they lived longer.
In only the cases with more advanced joint disease (moderate to severe), Providence and Cedar Grove women had double the rate of OA than Dallas women, whereas none of the women interred in Foster and Ridley had advanced joint disease (Figure 8; Supplemental Table 2). Both rural and urban men exhibited moderate to severe OA, with the highest frequency (by a small margin) observed for Freedman's. What is more telling is the mean ages of those affected. Dallas men and women developed moderate to severe joint disease by their mid-forties, compared to rural men and women who were 50+ years old. The results are somewhat unexpected, because sharecroppers began farming as young as age seven (Wilkison Reference Wilkison2008:56). In certain instances, there is an elevated risk of developing OA when work-related stress is high, and it begins early in life (Weiss and Jurmain Reference Weiss and Jurmain2007:444). Thus, farming has been implicated in higher rates of OA, especially of the hips, in comparison to other occupations.

Figure 8. Osteoarthritis by sex, age-at-death, and site. Each circle represents an individual affected with joint disease.
Research on farmers found an elevated risk of hip OA that increased the longer they farmed (Thelin et al. Reference Thelin, Jansson, Jacobsson and Ström1997). Men who began heavy manual labor in their teens also had greater risks of developing OA (Croft et al. Reference Croft, Coggon, Cruddas and Cooper1992:1271; Thelin et al. Reference Thelin, Jansson, Jacobsson and Ström1997). That Dallas adults had similar or higher rates of OA and at younger mean ages points to greater work-related stress. Further, despite the relationship between farming and hip OA, adults interred at Freedman's surpassed Cedar Grove adults in the frequencies of hip and knee OA (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002:255). This rural–urban disparity in joint disease is likely due to the nature of sharecropping, which, although arduous and beginning at an early age, was seasonal, and the work was more self-paced after emancipation (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002:265). In addition, because sharecroppers worked as families, most chores were shared.
Labor, Reproduction, and Black Maternal Health
African Americans’ morbidity and mortality differed by place, age, and also gender. Figure 9 shows that women died at younger ages and at higher numbers than men. For adults who survived childhood, nearly half of the men lived past 40 compared to only 26% of women. Over time, men consistently outlived women in both rural and urban contexts (Figure 10). In this section, we consider how gender and racial oppression led to differential experiences for black women that adversely affected their health and longevity (Zuckerman and Crandall Reference Zuckerman and Crandall2019). More specifically, our focus on black women of reproductive age reveals how childbirth relates to a “larger constellation of problems that put women at risk for high rates of morbidity and mortality” (Stone Reference Stone2016:151).
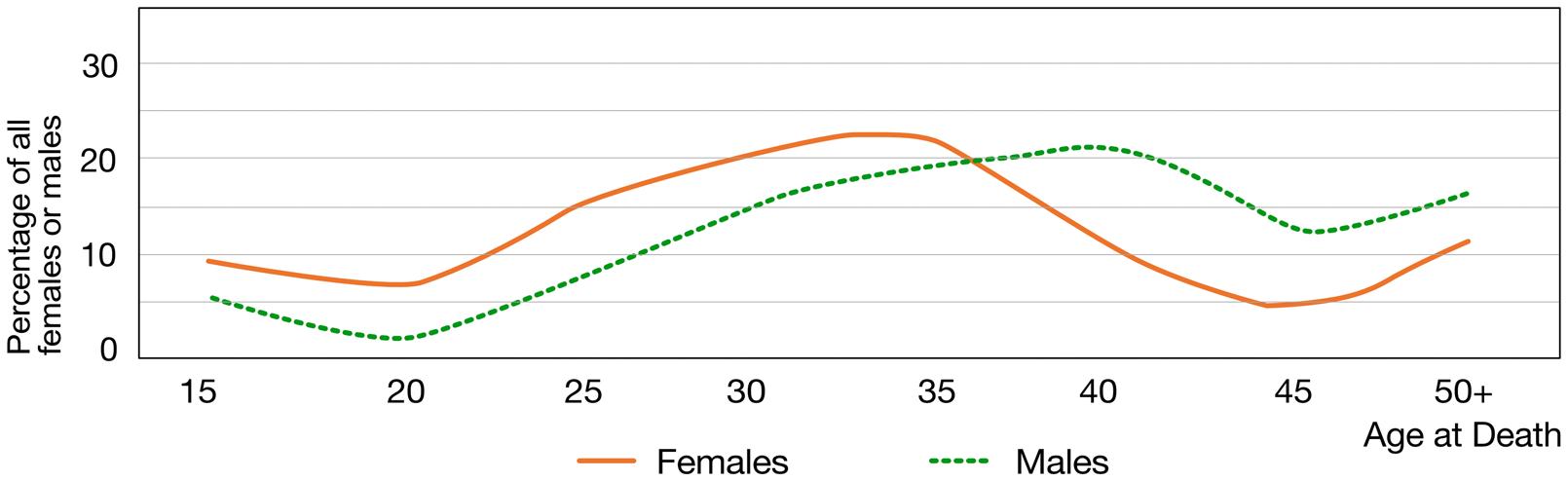
Figure 9. Mortality profiles for adult females versus males. The mortality distribution for females was significantly different from that of males (KS test, D[606] = 0.27, p = 0.0001).

Figure 10. Mean age-at-death for adult males versus females (left), and mortality rates for rural versus urban females (ages 15 to 34 years).
Black Women's Working Lives
Pamela Geller (Reference Geller2017:126) argues that the “heteronormative assumptions” surrounding the sexual division of labor (men produce, women reproduce) are “the philosophical bedrock in many bioarchaeological studies.” We agree with this critique and note that this gender dichotomy of labor did not apply to the majority of enslaved and free black women (Collins Reference Collins2000; Rankin-Hill Reference Rankin-Hill, Zuckerman and Martin2016). Black women farmed (Burton Reference Burton1998), and most urban black women had jobs, either because of their spouse's underemployment or because they headed their own households (Jones Reference Jones2009:103–105). In the urban South, it was common for black women to raise children on their own (Ayers Reference Ayers2007:69). As early as 1880, about 30% of black households in Dallas were headed by women (Teague and Davidson Reference Teague, Davidson and Barnes2011:93).
Urban black women typically worked as laundresses. Of the black women who worked in Dallas and who were listed in the 1909 city directory, 40% were laundresses (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002:260–261). Although the pay was low, this work came with certain advantages (Hunter Reference Hunter1997:57–58; Wilkie Reference Wilkie2003:83–84). Laundresses were largely self-employed, and because they often worked from home, laundresses could wash clothes, do their household chores, and raise their children. Yet laundering led to OA of the shoulder and elbow; exposure to contaminated water and dirty laundry meant that laundresses were prone to contracting diseases (Davidson et al. Reference Davidson, Rose, Gutmann, Haines, Condon, Condon, Steckel and Rose2002:261; Rankin-Hill Reference Rankin-Hill, Zuckerman and Martin2016:144).
Black women's working lives troubled the private–public gender binary. They worked outside of the home and were essential to their household's economy. In rural areas, their productivity (canning, gardening, selling butter and eggs) alleviated the family's dependence on merchant credit (Ayers Reference Ayers2007:204–205). They shopped, cooked, sewed clothes, cleaned, nursed the sick, and raised children. Black women's labor was physically and emotionally demanding, and these “invisible stressors” are implicated in maternal health (Stone Reference Stone2016:167).
Black Maternal Morbidity and Mortality
Black women experienced higher rates of maternal morbidity, stillbirths, and deaths than white women (Carson Reference Carson1994:37; Elman et al. Reference Elman, London and McGuire2015:203). In 1880, about 2.5% of white women versus 4.9% of black women died of “afflictions connected with pregnancy” (U.S. Census Bureau 1881, 11:29), and this disparity continued into the 1930s (Cutright and Shorter Reference Cutright and Shorter1979:196; Elman et al. Reference Elman, London and McGuire2015:194–195; Loudon Reference Loudon1988:188, 213). From 1910 to 1940, black female mortality exceeded that of males; Ewbank (Reference Ewbank1987:109) remarked that this atypical pattern of black mortality was “clearly related to problems with childbearing.” We posit instead that the broader inequalities experienced by black women were the root causes of maternal mortality, not childbearing in and of itself.
Our contextualization of black maternal health within structural oppression is influenced by a recent biocultural study that considers gendered violence as a root cause of maternal deaths. Pamela Stone (Reference Stone2016) asserts that birth is a natural process, yet women's reproductive bodies have become pathologized in the paleoanthropological literature. Stone argues that it is not childbirth but broader inequalities that compromise maternal health. Although she focuses on the related rise of modern obstetrics, reproductive risk management, and maternal mortality, Stone (Reference Stone2016:162) also considers other “general stressors” that put expectant mothers at risk.
It is unknown how many of the women we studied died of complications related to pregnancy and childbirth. Women's reproductive years are between 15 and 44, with advanced maternal age at 35+ years. Twenty-eight percent of rural women died before the age of 35, and well over half (56%) of the women buried at Freedman's never lived to that age (Figure 10). Even though the age-at-death data on their own are not a reliable measure for maternal mortality, the statistics related to black women's fertility suggest that at least a portion of them succumbed to childbirth complications.
Although fertility rates declined over the late nineteenth and early twentieth centuries (Haines and Steckel Reference Haines and Steckel2000; Tolnay Reference Tolnay1981), black women still bore more children than whites. In 1900, their total fertility rate (TFR) was about 5.6 children versus 3.5 for whites (Tolnay Reference Tolnay1987:213–217). Between 1886 and 1892, rural black women had a much higher TFR (9.2) than urban women (5.3), and rural women had a high TFR until the 1940s (Tolnay Reference Tolnay1981:453–454, Reference Tolnay1987; Tolnay and Glynn Reference Tolnay and Glynn1994). Thus, not only was sharecropping a form of debt slavery but it was also implicated in rural black women's reproductive burden. Plantation tenancy encouraged childbearing, because larger families fared better odds in securing labor contracts; yet multiple births elevated the risk of maternal death (Elman et al. Reference Elman, London and McGuire2015:202; Leavitt Reference Leavitt1986:25–26).
While women interred at Freedman's and Cedar Grove, in particular, survived childhood malnutrition and illness, these early life stressors probably elevated their risks for maternal morbidity and mortality. Relatedly, the data for CO for infants one year of age or younger (Supplemental Table 1) point to poor maternal health. Their nursing mothers were very likely malnourished, a condition they passed on to their infants through nutritionally poor breastmilk (Walker et al. Reference Walker, Bathurst, Richman, Gjerdrum and Andrushko2009). A lack of access to medical care and nutritious diets meant that black women were likely to succumb to the primary causes cited for maternal deaths. Until the 1930s, puerperal sepsis (postpartum infection) was the main cause of maternal deaths, followed by hemorrhaging and toxemia (preeclampsia; Loudon Reference Loudon1988:193–195). Black women died of infection and toxemia more often than whites (Carson Reference Carson1994:37; Cutright and Shorter Reference Cutright and Shorter1979:196). Chronic anemia elevates the risk of hemorrhaging (Loudon Reference Loudon1988:197; Stone Reference Stone2016:167). The evidence for PH among Freedman's and Cedar Grove females raises the possibility that they struggled with anemia, a condition that is exacerbated by pregnancy, into their childbearing years. African Americans are at a higher risk than whites of developing rickets, which can lead to pelvic deformities that increase the risk of obstructed labor and death (Cutright and Shorter Reference Cutright and Shorter1979; Stone Reference Stone2016:155).
We presented one plausible explanation for why women had higher rates of midlife mortality than men, and there are undoubtedly others. Pregnancy and childbirth within the context of racism and gendered violence put black women at risk for an early death. In both cities and rural areas, they assumed strenuous workloads, and expectant mothers continued to work out of necessity. These stressors, combined with impoverishment, all but ensured poor maternal health.
Discussion and Conclusion
After 1865, most African Americans in the South followed two trajectories: they stayed as farmers in the rural areas that they were deeply familiar with or struck out for towns and cities seeking a different way of life. In the countryside, anti-black racism and economic subjugation made it extremely difficult to move out of tenancy and sharecropping, whereas in the cities most African Americans continued to work as low-wage laborers with little job security. Within this historical context, our research addressed the heterogeneity of black experiences based on bioarchaeological evidence. Our comparisons of the data by age, place, and gender helped elucidate how and why health and longevity differed between communities and between men and women. We draw four conclusions from our research: (1) for those who survived to adulthood, urbanites had higher midlife mortality and reduced longevity compared to farmers; (2) urban and rural black children experienced poor health and high mortality; (3) relatedly, there were notable health and mortality disparities between the rural communities; and (4) black maternal health was implicated in the gender disparity in midlife mortality. We discuss each of these conclusions next.
African Americans led precarious lives in cities, including Dallas. The increasing frequencies of hypoplastic teeth, CO, and PH over time were undoubtedly due to the city's population growth, which exacerbated problems with crowding, sanitation, and the spread of diseases. Malnourishment, contaminated weaning foods, and diarrheal diseases are also implicated in the high rate of infant deaths (Table 3) and the CO observed in children three years and younger. Based on the data for osteoarthritis, black Dallasites also experienced a more physically demanding working environment than farmers. Importantly, Dallas men and women died at younger ages than their rural counterparts; far fewer lived to age 50 or older. This suggests that childhood chronic stress, biological weathering, and continued residence in the city elevated the risks of illness and mortality in urban adults.
A focus on childhood stress and mortality by site complicated the urban penalty thesis. Before 1900, the comparable urban–rural mortality rates and frequencies of enamel defects for Elko Switch and Freedman's suggest similarly adverse conditions for children in both settings. After 1900, stress markers and child mortality varied significantly across the rural populations. Compared to Freedman's, individuals interred at Foster, Ridley, and Providence had lower rates of enamel defects, porotic hyperostosis, or both. At the same time, however, the rate of child mortality in Cedar Grove and Ridley surpassed that in Freedman's. There was also the issue of poor skeletal preservation at rural sites, with a potential underrepresentation of children for Foster Cemetery. Poor preservation also precluded the possibility of including all of the rural samples in the comparisons of LEH, CO, and PH. Yet, based on the evidence at hand, there was greater complexity in childhood health than the urban penalty suggests. Although the countryside was not altogether healthier for children, for those who survived to adulthood, residence in low-density rural areas led to greater longevity and a less stressful working environment than urban living. Finally, rural and urban child mortality declined over time, and we provided possible avenues for future research to explain this pattern.
Cedar Grove, in particular, challenges the notion that black farming communities were a homogeneous group with unvaried lifeways and environmental conditions. This community had more deaths among children and higher frequencies of hypoplastic teeth, CO, and PH than any other community, including Dallas. We posited that dietary differences and greater exposure to disease and parasites may help explain the health disparities between these rural enclaves. Further, as in Freedman's, poor maternal health, diarrheal diseases, and weaning practices were the likely causes of the cribra orbitalia observed in very young children. Of the rural populations we studied, Cedar Grove was anomalous. However, further bioarchaeological research is likely to reveal an even more diverse spectrum of health and mortality outcomes between African American farmers.
Had we just focused on the evidence for physiological stress, we might have proposed that men's quality of life was lower than or similar to that of women. Yet the gender disparity in mortality rates suggests otherwise. We concluded that women's burden of domestic and extra-domestic labor, coupled with the stress of having and rearing children, played a role in elevating their risk of an early death. Compared to white women, black women had poorer maternal health, nearly double the rate of deaths related to childbirth, and much lower life expectancy. Importantly, an emphasis on black women's life experiences underscored how structural inequalities systematically disadvantaged them (Prather et al. Reference Prather, Fuller, Marshall and Jeffries2016).
Bioarchaeological evidence is remarkably sensitive to the role of gender, racial, and economic inequalities in influencing quality of life (Blakey and Rankin-Hill Reference Blakey, Rankin-Hill, Zuckerman and Martin2016; Buzon Reference Buzon, Walker, Verhagen and Kerr2005; Geller Reference Geller2017; Grauer et al. Reference Grauer, Williams, Bird, Zuckerman and Martin2016; Rankin-Hill Reference Rankin-Hill, Zuckerman and Martin2016; Stone Reference Stone2016). This avenue of research is relevant in today's society, because it resonates with current concerns regarding health disparities. In the United States, black children have historically suffered from poor health and high mortality rates, and current infant mortality rates for African Americans are twice that of non-Hispanic whites (Hamilton et al. Reference Hamilton, Hoyert, Martin, Strobino and Guyer2013:552–555; Prather et al. Reference Prather, Fuller, Marshall and Jeffries2016:666). Chronic diseases, including cancer, stroke, diabetes, and HIV/AIDS, afflict black Americans at higher rates than they do whites (Noonan et al. Reference Noonan, Velasco-Mondragon and Wagner2016). Coronary heart disease (CHD) is the leading cause of death among Americans. Yet, although CHD is less prevalent among blacks than whites, blacks still die more often from it (Leigh et al. Reference Leigh, Alvarez and Rodriguez2016:9). Black women's unequal access to health care means they experience higher incidences of pregnancy-related complications and deaths than women of other races (Prather et al. Reference Prather, Fuller, Marshall and Jeffries2016:664). As of this writing, African Americans suffer disproportionately from COVID-19-related deaths than other racial groups. The continuation of these disparities can be traced back to the communities we studied. Using bioarchaeological data, important work remains to be done in historicizing health and inequality to better address racism and how it “gets under the skin” (Goodman Reference Goodman, Zuckerman and Martin2016).
Acknowledgments
We thank James Davidson for his support and feedback as we worked on this article. Thank you to Nedra Lee, Anna Agbe-Davies, Rachel Watkins, and Lauren Springs for providing helpful comments. We are grateful to Brandon Thompson, Lee Meadow Jantz, and Guy Weaver who responded with collegiality to our requests for data. We acknowledge the researchers who worked on these projects; the quality of their work made ours possible. Enrique Rodríguez-Alegría wrote the Spanish abstract, and we thank him for his assistance. We extend our gratitude to our peer reviewers and editor Lynn Gamble, all of whom were generous in assisting us with improving this manuscript with thoughtful and constructive comments and suggestions.
Data Availability Statement
No original data were presented in this article.
Supplemental Materials
For supplemental material accompanying this article, visit https://doi.org/10.1017/aaq.2020.58.
Supplemental Table 1. Frequencies of Cribra Orbitalis and Porotic Hyperostosis by Age-at-Death Cohort.
Supplemental Table 2. Frequencies of Osteoarthritis by Sex and Mean Age-at-Death.

















