

Introduction
This chapter provides foundational knowledge of the occurrences, events, and disease manifestations during the early stages of the COVID-19 pandemic, including the responses and measures that were undertaken to contain the transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19. The importance of early intervention is discussed throughout this chapter to illustrate the impact that timely action – or, in many cases, inaction – had on the development of the pandemic. This chapter explores the data collection and analysis mechanisms utilized to monitor disease spread in different geographies. The necessity of information that is derived from early disease vigilance and subsequent surveillance programs is stressed. This chronological account is intended to create a roadmap for health and governmental authorities to follow for future undertakings, programs, and decision-making processes at the earliest phases of future pandemics.
Disease Outbreak
The spread of infectious diseases affects both individuals and entire communities. Early detection of a new outbreak is crucial so that containment measures can be implemented quickly enough to minimize the need for large-scale quarantine, especially when resources are limited. When primary care, public health, laboratories, and involved communities collaborate effectively, early identification and mitigation initiatives are achievable. This section outlines the initial detection of the COVID-19 outbreak and the responses of governments, public health officials, and communities. Figure 1.2 is designed to help visualize the significant occurrences during the earliest phases of the COVID-19 pandemic.


Figure 1.2 Pandemic evolution: from early detection to the declaration of the COVID-19 pandemic.
CCDC, Chinese Center for Disease Control and Prevention; CDC, US Centers for Disease Control and Prevention; WHO, World Health Organization.
First Cases
On December 19, 2019, a case of pneumonia of unknown origin was detected in Wuhan, China, a city of 11 million people and the capital of Hubei province in central China. By December 29, 2019, four more cases had been reported to the Chinese Center for Disease Control and Prevention (CCDC).Reference Li, Guan and Wu1 All initially reported cases were related to the Wuhan South China Seafood Market (Huanan Seafood Wholesale Market). These cases had been identified through a surveillance mechanism for “pneumonia of unknown etiology,” a concept designed to allow timely identification of novel infectious organisms introduced following the 2003 SARS-CoV outbreak.Reference Xiang, Havers and Chen2 Due to varying disease severity and clinical manifestations, these cases attracted the attention of local physicians. While little was known about the cause of these infections, there were indications of a possible new emerging virus that diverged from the classical influenza virus.
Roughly 10 days later, the medical administration of the Wuhan Municipal Health Commission (http://wjw.wuhan.gov.cn/) issued and distributed a document announcing the outbreak, reporting 27 new cases of pneumonia, mostly in stallholders at the Wuhan South China Seafood Market. Seven of these patients were in critical condition. Various hospitals in Wuhan held emergency symposia, where they defined a suspected case as a patient who met all four of the following criteria: fever, with or without recorded temperature; radiographic evidence of bilateral pneumonia; low or normal white blood cell count or low lymphocyte count; and no improvement in symptoms after three days of antimicrobial treatment, as per standard clinical guidelines. A patient who met the first three criteria and had an epidemiological link to the Wuhan South China Seafood Market could also be considered a suspected case.3
Local authorities responded by initiating virus-typing studies, implementing population isolation, and closing the market. While most patients were linked to the Wuhan market, it soon became evident that human-to-human transmission had been occurring since mid-December and that the number of cases was doubling every 7.4 days.
Early reports referred to the outbreak as “viral pneumonia,” suggesting that bacterial agents had been ruled out. Although the exact virus that caused the outbreak was unknown, the similarity in symptomatology to the previous SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV) outbreaks led health officials to hypothesize that it was another SARS-CoV outbreak.
Initially, Chinese health officials were free to share information about the newly emerging infectious disease; however, China’s federal authorities quickly began inhibiting global medical and scientific communication. The Chinese government began to censure doctors who, in December 2019, raised the alarm about this pneumonia of unknown origin. For example, at the Central Hospital of Wuhan, a young ophthalmologist expressed his concerns to coworkers about a virus that he felt resembled SARS-CoV, a disease that originated in China and spread to four countries in 2003. The police summoned and admonished him, together with seven other doctors, on January 3, 2020. He was instructed to “stop making false comments” and investigated for “spreading rumors.”3 Tragically, he contracted COVID-19 and, on February 7, 2020, he passed away at the age of 33.Reference Wenliang4
By January 1, 2020, according to the World Health Organization (WHO) Newsroom, “the causal agent had not yet been identified or confirmed.”Reference Huang5 Further requests were made to the Chinese authorities for information that would enable assessment of the risk posed by the virus. On the same day, the Wuhan South China Seafood Market was closed, and the Chinese National Health Commission set daily meetings to monitor potential pneumonia epidemics. While it was clear that humans were infected with pneumonia of unknown etiology, the initial theories seemed to suggest a link to a wholesale fish and live animal market, indicating possible exposure to animals. Up to this point, information about the situation was only reaching local and international communities informally or through news released by the press, and they had received limited information to determine and monitor the potential risks.3, Reference Huang5 The WHO assembled an incident management support team, which recommended continued public health measures and surveillance of influenza and severe acute respiratory infections. These recommendations did not include any specific measures for travelers.
On January 3, 2020, the Chinese government formally notified the director of the US Centers for Disease Control and Prevention (CDC) of the outbreak, revealing that 44 patients with pneumonia of unknown etiology had been reported, 11 of whom were critically ill, with the remaining 33 in stable condition.3, 6 In January 2020, Chinese scientists at the National Institute for Viral Disease Control and Prevention announced the discovery of a new coronavirus.Reference Khan7 This novel coronavirus was the pathogenic cause of the viral pneumonia of unknown etiology, designating the disease as a novel coronavirus-infected pneumonia.
Responding to a surge in pneumonia cases with unknown etiology, on January 7, 2020, the CDC established an “incident management system” and issued watch level 1 travel precautions for Wuhan, China. The CDC recommended that visitors to Wuhan avoid contact with sick people; avoid animals (alive or dead), animal markets, and products that originated from animals (such as undercooked meat); and wash their hands often with soap and water. Additionally, the CDC advised anyone who had traveled to Wuhan and felt sick to isolate at home, except when seeking medical attention. At this stage, the WHO was uncertain of the cause of the 59 pneumonia-like cases, but it began to suspect that a novel coronavirus was to blame. Further research was required to correctly diagnose the individuals infected with the emerging virus.
Viral Pathogen Sequencing
Genomic sequencing is a laboratory technique used to decipher the full genetic composition of an organism (a virus in this case) or cell type. This approach may also be used to detect changes in specific regions of the genome. Viral sequencing was a quickly emerging technology that was critical in the diagnosis of COVID-19 and for understanding the transmission and management of the novel coronavirus.
On January 5, 2020, researchers at Fudan University, Shanghai, at the Shanghai Public Health Clinical Center and at the Fudan University School of Public Health published the sequence of SARS-CoV-2, the virus that causes COVID-19.Reference Zhang8, 9 The sequence was published to GenBank and the Global Initiative on Sharing All Influenza Data, both of which are online databases that are open and accessible to the public.
The genetic information became available to the WHO on January 12, 2020, opening the gateway for laboratories in different countries to produce specific, diagnostic polymerase chain reaction (PCR) tests that could detect the novel infection. The isolation and sequencing of the new virus confirmed it was a coronavirus.Reference Wu, Zhao and Yu10 While the Chinese researchers provided an essential tool for developing diagnostic tests, the Chinese authorities reacted negatively once again, closing the sequencing laboratory and ordering the “rectification” of disclosed statements on the virus, as well as the censorship of “misleading information” on social media.3
Assessment of Infectivity
In early January 2020, the Wuhan Municipal Health Commission stated that there was “no clear evidence of person-to-person transmission and while the possibility of limited person-to-person transmission cannot be ruled out, the risk of sustained person-to-person transmission was low.”11 A retrospective analysis of initial data shows that this was not true, the data highlights the necessity for early assessments of disease infectivity. Assessments of disease infectivity provide vital insight into how easily a disease is transmitted from human to human, which better informs officials on the best mitigation practices. Finally on January 20, 2020, China confirmed person-to-person transmission of the novel coronavirus and infections among medical workers.3
A universal measurement of disease transmission is the reproduction index (R0). The R0 index is defined as the number of susceptible people that one person with the disease can infect. It is a function of the following variables: the period of infectivity after infection, the chance of infection transmission per contact between a susceptible and an infectious individual, and the contact rate.Reference Chang12
Studies found that the initial Wuhan SARS-CoV-2 strain exhibited an estimated R0 value between 1.4 and 2.5. For context, this value is displayed in Table 1.1 in comparison with other coronaviruses and known respiratory viral diseases with potential epidemic spread.Reference Lindstrøma, Engebretsen and Kristoffersen13 It is important to note that the infectivity of SARS-CoV-2 changed with the introduction of new variants.Reference Liu and Rocklöv14–Reference Fan, Li and Zhang16 Each variant presented structural changes to the viral spiral proteins that control binding to epithelial angiotensin converting enzyme 2 (ACE2) receptors and thus affect the infectivity of the virus. For more information on the impact of variant infectivity, see Chapter 9.
Table 1.1 Viral infectivity: basic reproductive number (R0) of various known respiratory viral diseasesReference Chang12–Reference Fan, Li and Zhang16
| Virus | Disease | R0 | Transmission |
|---|---|---|---|
| SARS-CoV-2: original Wuhan strain | COVID-19 | 2.4–2.6 | Respiratory droplets/aerosol |
| SARS-CoV-2 alpha (B.1.1.7) | COVID-19 | 4–5 | Respiratory droplets/aerosol |
| SARS-CoV-2 delta (B.1.617.2) | COVID-19 | 5–8 | Respiratory droplets/aerosol |
| SARS-CoV-2 omicron (B.1.1.529) | COVID-19 | 8.2 | Respiratory droplets/aerosol |
| SARS-CoV | Severe acute respiratory syndrome | 2.2–3.6 | Respiratory droplets |
| MERS-CoV | Middle Eastern respiratory syndrome | 1.7–3.1 | Direct contact or large virus-laden droplets |
| Influenza A | Influenza | 0.9–3.1 | Respiratory droplets |
| Respiratory syncytial virus | Bronchiolitis | 1.2–3.0 | Respiratory droplets/fomites |
| Rhinovirus | Cold-like illness | 2.0–3.0 | Respiratory droplets |
| Measles virus | Measles | 12.0–18.0 | Small particles/aerosol |
| Mumps virus | Mumps | 10.0–12.0 | Respiratory droplets |
| Ebola virus | Ebola virus disease | 1.5–2.5 | Body fluids |
| Adenovirus | Human adenoviruses systemic infection | 2.3 | Respiratory, fecal–oral |
Disease Progression
While the Wuhan Municipal Health Commission was reporting no new infections or deaths, stating that the cumulative number of cases in the city had remained steady at 41, cases were being detected internationally. The first COVID-19 case inside the United States was detected on January 21, 2020, in a passenger returning from Wuhan. The CDC quickly set up a team to investigate the case and began tracing the patient’s contacts. Similarly, cases were identified in the Republic of South Korea, Japan, Thailand, Singapore, France, Germany, Italy, the United Kingdom, and Spain.Reference Worobey, Pekar and Larsen17
On January 22 and 23, 2020, the WHO Director-General convened an emergency committee under the 2005 International Health Regulations (IHR), issuing a comprehensive package of technical guidance on how to detect, test for, and manage potential cases.
On January 23, 2020, the Chinese government placed Wuhan in lockdown. By this time, the virus had spread to other provinces, and nearly 5 million people had left Wuhan to celebrate the Lunar New Year. Approximately one-third of those individuals traveled to locations outside Hubei province. The measures introduced by the Chinese government included strict social distancing, isolation requirements, the use of masks in public places, and the extension of the Lunar New Year holiday until March 10 for Hubei province and February 9 for many other provinces.Reference Chen, Yang, Yang, Wang and Barnighausen18, Reference Cohen19
By the end of January, new epidemiological information revealed increases in the number of confirmed cases, suspected cases, and affected provinces, and in the proportion of deaths among the cases that had been reported to date (~3%; 17 of 557). Fourth-generation cases in Wuhan and second-generation cases outside Wuhan were reported, as well as some clusters outside Hubei province. Figure 1.3 shows the first reported analysis of the COVID-19 epidemic undertaken using the information system of the CCDC. The analysis showed that, over 30 days, the disease had spread from Hubei province to the rest of mainland China. It provided information on patient characteristics, calculations of case fatality and mortality rates, a geo-temporal analysis of viral spread, and an epidemiological curve construction based on location, contacts, disease severity, comorbidity, and geography.

Figure 1.3 Series of graphs illustrating the spread of SARS-CoV-2 within China’s provinces before the declaration of the COVID-19 pandemic.20
The identification of the events that led to the infection of patient zero is crucial in investigating any epidemic outbreak. For SARS-CoV-2, these events were never clearly identified; thus, the possibility that SARS-CoV-2 was already circulating in Wuhan at the time of the outbreak has led to the proposition that the seafood market was a consequence, rather than the source, of the SARS-CoV-2 virus.Reference Cohen19 A study published in 2021 applied a technique known as the “mutational order approach” – which was initially developed to identify the evolutionary history of malignant tumor clones – to reconstruct the ancestral sequence and mutational history of SARS-CoV-2 genomes.Reference Kumar, Tao and Weaver21 The results demonstrated the worldwide presence of SARS-CoV-2 well before the pandemic began, which makes it nearly impossible to identify patient zero.
Unfortunately, when the pandemic began, there was no surveillance system in place that could efficiently reflect the severity of the outbreak, its impact, or the required mitigation measures. Such a surveillance system would have facilitated and improved international coordination, including research efforts for developing medical countermeasures. Additionally, a lack of transparency from the Chinese government negatively affected the investigation of the initial outbreak in Wuhan. While general measures for controlling the crisis were eventually advised in specific countries and geographies, there were no conclusive or specific recommendations of measures to be implemented internationally, including for international travel.
Declaration of Health Emergency
On January 30, 2020, the WHO COVID-19 IHR Emergency Committee reconvened and, on January 31, 2020, the WHO issued recommendations for a global health emergency to be declared. Three days later, the United States declared a public health emergency. Despite this and the progressive spreading of virus infections and indications of intercontinental distributions of the disease, several members of the WHO committee considered it still too early to declare a public health emergency of international concern (PHEIC). With cases continuing to increase and in the face of an evolving epidemiological situation, the WHO’s resistance to declaring a PHEIC was questionable. Issuing an intermediate-level alert could have reflected the severity of the outbreak. In the absence of conclusive recommendations, international travel continued and cases spread globally in alarming numbers.
Research and Development Prioritization
On February 4, 2020, the WHO published the 2019 Novel Coronavirus (2019-nCoV): Strategic Preparedness and Response Plan, which included accelerating research and development (R&D) processes as one of three major strategies. On February 11 and 12, 2020, the WHO held the “Global Research and Innovation Forum: Towards a Research Roadmap for COVID-19.” The fact that a COVID-19 R&D forum was the first meeting convened after the PHEIC declaration testifies to the importance of R&D in response to emerging infectious diseases.Reference Jee22
The prioritization of research allowed for rapid identification of the pathogen behind the SARS-CoV-2 outbreak and successful sequencing of the genome by February 7, 2020. In parallel, international research resulted in the prompt understanding of the physiopathology of viral infection and the disease progression, with the initiation of vaccine research by early March 2020.
Very judiciously, in February 2020, The Jenner Institute of the University of Oxford started developing the Oxford–AstraZeneca vaccine. By April 2020, 115 vaccines were in development, 73 of which were in the exploratory phase; however, only a handful of the vaccine projects succeeded. These R&D achievements were crucial and led to the development of vaccines in just 9 to 10 months, with these vaccines being granted temporary and conditional authorization. In December 2020, a 90-year-old female patient became the first person to receive a SARS-CoV-2 vaccine. Nevertheless, the R&D infrastructure was poorly coordinated overall and was still an inadequate response to a pandemic of this size.
A report prepared by the Independent Panel for Pandemic Preparedness and Response (IPPPR) highlighted the benefit that science and researchers provided during the COVID-19 pandemic.23 The panel stated that the expertise and technology from decades of work – specifically on HIV, Ebola, and cancer vaccine research and immunology – were available and ready to apply to the new virus.
Global Response
One of the first coordinated efforts to curtail transmission occurred on a cruise ship that originated in Japan on January 20, 2020, with stops in Hong Kong, Vietnam, and Taiwan before returning to Japan on February 3, 2020. A passenger on board presented with symptomatology and subsequently tested positive for the novel virus. The ship was thus placed in quarantine. From the information collected, it was clear then that substantial transmission of COVID-19 had been occurring before the implementation of quarantine, that the quarantine intervention was effective in reducing transmission among passengers, and that, among contacts, there were asymptomatic cases requiring at least 14 days of isolation to reduce transmission.24
Data analysis on patient characteristics is critical for calculations of case fatality, mortality rates, a geo-temporal analysis of viral spread, and an epidemiological curve construction based on location, contacts, disease severity, comorbidity, and geography.20, Reference Chen, Zhou and Dong25
By February 2020, Korea had demonstrated remarkable research capacity by conducting high-throughput COVID-19 testing and utilizing innovative drive-through sampling. These measures for early detection and the screening of cases should have been followed by full global efforts to produce research-based evidence by thoroughly analyzing epidemiological, clinical, and immunologic data, which would facilitate the development of vaccines and therapeutics for COVID-19. However, there was no globally directed, concerted effort in place to facilitate the coordination. Korea was a key global partner in COVID-19 research and actively participated in the development of immediate and mid-/long-term priorities, which was jointly led by WHO partners.
Figure 1.4 illustrates the emergence of SARS-CoV-2 in Europe and the United States, mapping the path followed by infected travelers from China.Reference Worobey, Pekar and Larsen17 This identification of the various transmission networks was essential for the later demonstration of the effectiveness of countermeasures for the spread of the disease, including testing, isolation, quarantine, and air traffic control.
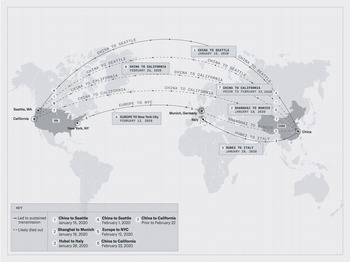
Figure 1.4 SARS-CoV-2 introductions to the United States and Europe.
Several clusters of cases were initially identified in 37 European countries, with variability in the incidence rate (IR) and mortality rate (MR) related to the population age and diverse national approaches to the crisis.Reference Fan, Li and Zhang16, Reference Zach, Hanová and Letkovičová26 From February 28 to May 21, 2020, the most severely impacted countries in terms of the IR and MR were Spain, Belgium, Ireland, Sweden, the United Kingdom, Italy, France, and the Netherlands, which had IRs and MRs higher than the European average. While the IR and MR are determined by multiple factors, the lack of initial unity in the various countries’ responses to the COVID-19 crisis may have led to some diversity in the numbers of cases and deaths. In Europe, the largest and most serious clusters of COVID-19 cases were in the Lombardy region of Italy in early March. The disease in this region was considered particularly severe owing to the unprecedented number of patients, including healthcare workers, and the very high case-fatality rate among elderly people, despite aggressive containment efforts.
The pandemic unfolded in the United States following the recognition of the first cases on the west coast (Santa Clara, CA, and Seattle, WA), and clusters of infection began developing from people traveling back from the Far East who were infected and showing clinical symptoms. This made it very clear that we were dealing with a pandemic of massive proportions. The exponential growth of reported cases in the United States is indicated in Figure 1.5. The cases reported at that time may have represented only a fraction of the total number of actual cases, as testing and contact tracing were not fully implemented at that time.
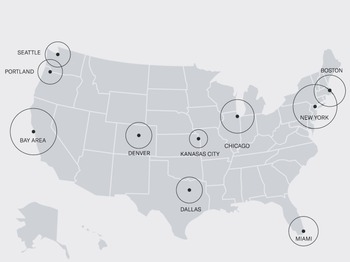
Figure 1.5 Relative infections in the United States as of March 1, 2020.
On March 11, 2020, the WHO declared COVID-19 to be a pandemic, with the Director-General declaring “the alarming levels of spread and severity of the outbreak followed by alarming levels of inaction.”Reference Zach, Hanová and Letkovičová26, Reference Chu, Akl and Duda27 Soon after, on March 15, 2020, the President of the United States declared COVID-19 to be a national emergency, offering billions of dollars in federal funding to combat the disease.
Pandemic Development and Consolidation
From March 2020 onwards, the pandemic spread globally, affecting different continents, countries, and cultures and impacting society at virtually all levels and types of activities. The spread of COVID-19 skyrocketed in the United States, with the fatality rate reaching 100 000, 300 000, and 1 million deaths by, respectively, May 23, 2020, December 12, 2020, and May 14, 2022.
Public health policies needed to be implemented for isolation, quarantine, and the control of human travel. The enacting of a social lockdown (March 21, 2021, in the United States) that restricted circulation, banned large gatherings, and promoted the closing of schools and business activities resulted in an unprecedented situation in which the entire global community underwent a shutdown that lasted for variable amounts of time, up to several months in some countries. Mechanisms to recognize COVID-19 transmission among presymptomatic and asymptomatic cases were of particular significance. Prompt contact tracing, including close and non-close contact from 2 days before clinical symptoms started, was demonstrated as effective in stopping further transmission.
Early experiments showed that SARS-CoV-2 aerosol and fomite transmission was extremely probable, and that social distancing (of 1 meter or more), the use of face masks (preferably N95) as personal protective equipment (PPE), and the use of eye protection were associated with less infection and could be efficient deterrents of virus spread.28 Surprisingly, it took over 6 months for the WHO to announce new guidance for the use of face masks (June 7, 2020).
One of the most basic measures for containing a pandemic is identifying infected people and putting measures in place for contact tracing, finding their contacts, and preventing them from infecting others. A major challenge for the United States was to remedy testing gaps by developing and providing nationwide the rapid diagnostic tests that were needed for an accurate diagnosis. The United States quickly rose to the challenge, with the CDC, Food and Drug Administration (FDA), and National Institutes of Health (NIH) working expeditiously to create and finance the bio-network needed to develop appropriate assay diagnostic systems.
The CDC developed protocols to utilize reverse transcriptase PCR as a highly specific diagnostic test. The NIH, working collaboratively with multiple partners across government, academia, and the private sector, created the Rapid Acceleration of Diagnostics (RADx®) initiative (April 29, 2020). The mission of RADx was to accelerate the development, validation, and commercialization of innovative point-of-care and home-based tests. Chapter 7 describes in detail the entire strategy and process to develop appropriate molecular tests for prompt and specific disease diagnosis. The FDA authorized the CDC’s test via an Emergency Use Authorization at the end of February 2020 under growing pressure to expand testing capacity. During 2020, 2021, and 2022 and potentially into 2023, many individual Emergency Use Authorizations for antigen and molecular diagnostic tests for SARS-CoV-2 were or are expected to be authorized, as described in Chapter 4. More details on the regulatory steps involved in granting Emergency Use Authorizations can be found in Chapter 10.
To analyze the actions taken by individuals, institutions, communities, local and national governments, and international bodies to suppress or stop the spread of disease, the WHO provides longitudinal public health and social measures (PHSM). The composite PHSM Severity Index expresses the average of six indicators, including wearing face masks; closing schools, offices, businesses, institutions, and operations; and restrictions on gatherings. The PHSM Severity Index has been useful to endorse the implementation of effective measures in areas where there was reluctance toward such measures.
Pandemic Preparedness
It became very evident as the pandemic progressed that no country was fully prepared for an epidemic or pandemic, and there was no consensual, comprehensive, global operational preparedness plan in place to respond to COVID-19, despite multiple efforts by many states and leading governmental organizations.29 As a result, countermeasures for controlling and preventing disease spread failed or achieved only partial results. Therefore, the Pandemic Response Accountability Committee was created for overseeing and guiding both national and international organizations and stakeholders on operating and synchronizing activities. Many organizations started working on the advancement of national preparedness at the federal, state, private, and academic levels.
One example is the Public Health Emergency Medical Countermeasures Enterprise, which coordinates and collaborates with partners to ensure that medical countermeasures and associated capabilities are available where needed. Another example is the Global Health Security (GHS) Index, which is intended to assess and improve national and international capabilities to address infectious disease outbreaks. Recent GHS Index reports reveal that, while many countries can develop the capabilities to confront a crisis, the majority remain unprepared to face future epidemics and pandemics. Gaps were detected in the level of financial investment, the fitness of the health systems, and the lack of mechanisms to detect outbreaks. In the United States, only 34% of states showed indicators of readiness for state emergency preparedness. Funding being revoked at the state level is in part responsible for some states’ poor performance.
There are several federal documents addressing various aspects of the governmental and administrative management of the crisis. For instance, the Pandemic Response Accountability Committee provides information on and strategies for how federal government funding for pandemic programs can be allocated, resources/monies can be appropriated, and spending can be tracked. The committee was established to promote transparency and coordinate oversight of the pandemic response.
The White House released the National Strategy for the COVID-19 Response and Pandemic Preparedness, a document produced by the federal government to coordinate the pandemic response across all federal departments and agencies and improve the effectiveness of our fight against COVID-19. This is a comprehensive document covering many aspects of the COVID-19 crisis and defining government participation, but with less emphasis on operational protocols.29
Crisis in the Health-Care System
The abrupt eruption of cases with severe disease placed tremendous pressure on health and hospital systems, as first seen in Italy.Reference Remuzzi and Remuzzi30, Reference Onder, Rezza and Brusaferro31 The medical community had to adapt to the crisis and develop capabilities to assist thousands, if not millions, of patients requiring special management, starting with isolation, transmission containment, monitoring disease severity, and critical care in intensive care units. Chapter 3 meticulously describes the impact of the numbers of patients with COVID-19 on emergency medicine and health-care organization in general in the United States.
The medical supply chain, which provides essential tools, medical supplies, medication, and PPE, was under tremendous strain to comply with increasing demands. The challenge for the network was to quickly develop efficient new production lines of products and services while lacking guidelines on allocation and distribution amidst changing regulations and pricing. Medical and surgical attention for all non-COVID-19 illnesses were limited, which resulted in delays in diagnostic and therapeutic interventions, including cancelations. Waiting lists for non-COVID-19 conditions soon reached millions of patients worldwide, and it is estimated that the waiting list will only be cleared by the end of 2023.
Disease Origin: Zoonotic Transference
With millions of people dead and even more hospitalized due to SARS-CoV-2, the burning question is: Where did this disease come from? All data at the time of writing this book suggest that SARS-CoV-2 originated from a zoonotic source. The WHO defines zoonosis as any disease or infection that is naturally transmissible from vertebrate animals to humans.32 The disease or infection can be passed from an animal to a human through direct contact (saliva, urine, blood, etc.), indirect contact (contact with the animal’s home [e.g. aquarium water or chicken coop]), or vector-borne (e.g. an insect bite), waterborne, or foodborne sources.
Zoonotic transference poses a large public health threat, as there is a close relationship between humans and animals in agriculture, in zoological settings, as domestic pets, and in nature. Scientists have estimated that three out of every four emerging infectious diseases have come from a zoonotic source. To strengthen this theory, and in trying to understand the source of the new virus, a researcher at the Fred Hutchinson Cancer Center investigated the virus’s evolution and identified a dataset containing SARS-CoV-2 sequences from early in the Wuhan epidemic. He was then able to reconstruct partial sequences of early viruses and concluded that they likely contained three mutations relative to the market viruses that made these sequences more similar to the bat coronavirus relatives of SARS-CoV-2.Reference Bloom33
More recently, studies on the distribution within the Wuhan market of animals susceptible to being infected with SARS-CoV-2 and humans infected with SARS-CoV-2 revealed that there was a spatial relative risk, even though it was not possible to establish a direct correlation. Because of the prevalence of cases and the disease distribution among the Wuhan population, it is understood that the Wuhan South China Seafood Market was the early epicenter of the COVID-19 pandemic.Reference Cohen19, Reference Andersen, Rambaut, Lipkin, Homes and Garry34–Reference Worobey, Levy and Serrano36 However, as mentioned earlier, some studies have shown that SARS-CoV-2 was already circulating before December 2019, and so it has also been proposed that the seafood market was a consequence, rather than the source, of the SARS-CoV-2 virus.Reference Kumar, Tao and Weaver21, Reference Worobey, Levy and Serrano36
Recent human coronaviruses, SARS-CoV and MERS-CoV, have been caused by zoonotic transmission. In 2003, SARS-CoV emerged through zoonotic spillover at a live animal market in China’s Guangdong province. Antibodies against SARS-CoV were detected in animals being sold at the market: masked palm civets and raccoon dogs. Further research discovered that the masked palm civets and raccoon dogs were most likely intermediate hosts, with the disease originating from horseshoe bats (Rhinolophus affinis), a species demonstrating a 99.8% nucleotide match with the human isolates. MERS-CoV is another human coronavirus likely originating from bats, as the disease has been detected in 14 distinct bat species. Anti-MERS-CoV antibodies have been isolated in camels in the Middle East, Africa, and Asia. Thus, the likely intermediate host between bats and humans for MERS-CoV has been identified as camels.
SARS-CoV-2 has been detected in several species, but no animal reservoir has been documented. It has been suggested that the most likely source of SARS-CoV-2 is the horseshoe bat species. Studies have found that there is about a 96% nucleotide identity match between the coronaviruses of humans and horseshoe bats (RaTG13 GenBank: MN996532.1). Additionally, phylogenetic analyses of a large subgenomic dataset of bat coronaviruses from China further support the claim that SARS-CoV and SARS‐CoV‐2 both likely originated in horseshoe bats. As humans do not commonly come into close contact with bats, the transmission to humans likely occurred through an intermediate host. This intermediate host would need to be one more commonly handled by humans, such as a domestic animal, livestock, or a domesticated wild animal. At the time of writing, no intermediate host for SARS-CoV-2 has been identified.
Reverse Zoonosis and Secondary Zoonosis
While the search for the zoonotic host continues, it is important to conduct research in parallel into which other animal species are susceptible to SARS-CoV-2 infection. This research will help epidemiologists better prevent secondary zoonotic events (transmission of the infection from animals back to humans) and possible reverse zoonosis (also referred to as zooanthroponosis: the transmission of the infection from humans to animals).Reference Goraichuk, Arefiev, Stegniy and Gerilovych37, Reference Munir, Ashraf and Munir38
There have been several cases of dogs, cats, and zoo animals testing positive for SARS-CoV-2 in countries such as Belgium, France, Spain, Germany, the United States, and Hong Kong.39, Reference Carlson, Albery and Merow40 Clinical manifestations in animals have ranged from asymptomatic to severe respiratory illness. When symptoms are present, they can include coughing, sneezing, respiratory distress, nasal discharge, ocular discharge, vomiting, diarrhea, fever, and lethargy. Although there is no definitive evidence that dogs, cats, or zoo animals can transmit SARS-CoV-2 to humans, it is important to be cautious of how the virus may behave in other animal species. For this reason, increased continuous monitoring and planned targeted surveillance of high-risk animals and their caretakers should be implemented at local and national levels.
There is not enough SARS-CoV-2 testing currently being done for companion and zoo animals. It is important to note that IDEXX Laboratories in the United States has released a diagnostic test, “SARS-CoV-2 (COVID-19) Real PCR Test,” for screening companion animals. Serological assays and nucleic acid-based tests for the diagnosis of SARS-CoV-2 in domestic and zoo animals are also being developed and used by several other private and government veterinary laboratories.
Zoonotic Monitoring
As explained previously, controlling and monitoring zoonosis is critical for responding quickly and effectively to emerging infectious diseases. Several organizations controlling and monitoring zoonosis include the:
CDC National Center for Emerging and Zoonotic Infectious Diseases
CDC Division of High-Consequence Pathogens and Pathology
National Animal Health Laboratory Network
WHO Scientific Advisory Group for the Origins of Novel Pathogens
World Organisation for Animal Health
These organizations collectively constitute a network through which new infectious agents are communicated and possible zoonosis reservoirs are monitored that represent a risk of epidemics and pandemics to humans. Furthermore, the Global Virome Project is an international initiative to map zoonotic viruses around the world through the creation of a database of animal viruses. In many ways, this project parallels the Human Genome Project, which has revolutionized our understanding of human diseases.
Therefore, the next question to ask ourselves is: What should we do in anticipation or even for the prevention of an upcoming pandemic? As the major source of novel infectious agents is zoonosis, comprehensive monitoring of animals for detecting zoonosis at the preemergence stage would be ideal, that is, at the stage when the disease is still in its natural reservoir before being transmitted to humans. However, given the high number of animal species and novel agents continuously emerging, this strategy would be extremely difficult, costly, and practically impossible to carry out to its full extent. Nevertheless, pandemic threat programs are emerging that aim to prevent pandemics at the source before they infect humans. These programs are based on the building of health-care capacity, surveillance and diagnostic programs, and the implementation of predictive disease modeling. Another important tool in zoonotic monitoring is viral molecular sequencing, which can provide useful information about virus dynamics, such as the viral mutation rate and the detection of selective sequences compatible with human receptors that can facilitate infection of human tissues. While these recent advancements are useful for monitoring and controlling the spread of infectious diseases, additional research and resources are needed to fully assess the dangers of zoonotic transmission.
A mathematical model developed to simulate potential hotspots of future viral sharing under climate change and land-use scenarios for 2070 predicted that species will aggregate in new combinations at high elevations, in biodiversity hotspots, and in areas of high human population density in Asia and Africa, driving the novel cross-species transmission of their viruses an estimated 4 000 times.Reference Sachs, Abdool Karim and Aknin41, Reference Kufferschmidt42 The model identified bats as the most likely mammal to share viruses along evolutionary pathways that will facilitate future emergence in humans.
Surveillance
From February 2020 to the present, an extraordinary surge of information has pervaded communications across the medical, scientific, epidemiological, statistical, social, and financial fields. Information provided in different formats – from recognized professional journals to media news – has helped enormously in the understanding, management, and control of the pandemic crisis.Reference Kufferschmidt42 Nevertheless, the analytical processing, interpretation, archiving, and overall evaluation of the current pandemic, as well as of future pandemics, is still under scrutiny and will require profound analysis before being incorporated as prescribed pandemic preparedness protocols.Reference Choi and Pak43
The epidemiological and clinical characteristics of COVID-19 were further clarified by a landmark communication in The Lancet in 2020, with the clinical description of 99 patients with COVID-19, 49 of whom had a history of exposure to the Wuhan South China Seafood Market.Reference Chen, Zhou and Dong25 This revealed the importance of rapid communication and the publication of all types of information related to pandemic evolution.Reference Kufferschmidt42, Reference Choi and Pak43 Around this time, the major publishers and university presses opened their archives with regard to articles related to COVID-19, a fortunate decision that helped tremendously in understanding the 2019 outbreak and in the decision-making process to develop appropriate diagnostic tools and countermeasures.
The implementation and management of effective surveillance systems are essential for early detection and effective responses to emerging infectious diseases.39 Surveillance systems provide officials with an understanding of when, where, and in which demographics an infectious disease is being transmitted. The data from surveillance systems are then used to inform decisions surrounding countermeasures, controls, prevention, and patient management. Inaccurate or incomplete data can drastically impact decision-making and potentially place people at higher risk of severe disease.
Surveillance has been a pillar of public health systems since the first recorded epidemic in Egypt in 3180 BC.Reference Choi and Pak43 Since then, surveillance has evolved with each epidemic and pandemic, including the first public health action as a result of surveillance during the 1348 bubonic plague epidemic, commonly coined the “Black Death,” when public health officials imposed the first quarantine by refusing the entrance of ships with infected passengers. More recently, we have seen both the strong and the weak points of our current surveillance systems through the COVID-19 pandemic.
One of the most vital data points tracked through the surveillance system is the number of cases. This information can be used to determine incidence (the number of new cases in a specific period), prevalence (the number of cases at one specific point in time), hospitalization (the number of cases resulting in the hospitalization of the patient), and deaths (the number of cases resulting in death). Based on WHO guidance, the minimum testing rate should be maintained as 1 person tested per 1 000 population per week to ensure sufficient data collection.
Additionally, the WHO suggests that strong surveillance systems include:
immediate notification of changes in epidemiological patterns
tracking of morbidity and mortality statistics
calculation and monitoring of disease impact on health-care capacity, including hospitalizations, intensive care unit admissions, the financial health-care burden, and the number of health-care workers
monitoring of variants through strategic and geographic genomic surveillance
effective monitoring of potential animal reservoirs
special studies (on the impact on high-risk groups, the characterization of new variants, and long COVID)
monitoring of vaccination doses when available; this should include both primary series and boosters
The delay between data collecting and analysis and the absence of data reporting from at-home testing are two significant challenges facing our current surveillance systems. For the most effective disease predictions and decisions, data must be analyzed in real time. One potential solution is to develop and deploy an electronic case-reporting system that would supply data seamlessly from a health-care provider’s electronic health record to a public health agency. These systems should be implemented both nationally and globally before the next pandemic.
A unique characteristic of the COVID-19 pandemic was the unprecedented number of at-home diagnostic tests being performed. This was a major accomplishment in slowing the spread of COVID-19, but it did impose difficulties in tracking the tests performed and the confirmed cases, as individuals were not required to report their results. Many individuals who tested positive on an at-home test had a confirmatory test done at a health-care facility, and these confirmatory tests were required to be reported. However, those who tested negative at home were not required to report and thus there was the possibility of overinflation of the positivity rate. Most at-home tests do have a reporting component for individuals to report their results, whether it be a mobile application or a website, but this is not often used. Further changes need to be made to address issues surrounding the lack of at-home reporting and the potential subsequent positivity rate inflation.
Scientists in California developed a nanobeads technique that allowed the identification of coronavirus strains circulating in a community up to 14 days earlier. This technique applied PCR to sewage and could become an early warning system to be used in surveillance.Reference Karthikeyan, Levy and De Hoff44, Reference Bonanno Ferraro, Veneri and Mancini45 According to the study published in Nature, the use of the nanobeads technique increases the amount of viral ribonucleic acid (RNA) that can be sequenced from a wastewater sample from 40% to nearly 95%.Reference Karthikeyan, Levy and De Hoff44 In addition, the California team also developed a method that allows the identification of the variants present in each wastewater sample and a determination of their concentrations.
The use of machine learning as a tool to extract concealed information patterns, mine huge raw datasets, and establish high‑quality clinical predictive models has proven to be very helpful. Similarly, digital medicine and artificial intelligence programs supporting data analysis and decision processes of clinical, genomics, and even sociocultural information have been successfully introduced through the COVID-19 pandemic.
Surveillance took several different formats across multiple media during the COVID-19 pandemic. This was largely due to many professional and nonprofessional media and government agencies advocating for the collection of critical information. The CDC is a leading surveillance institution in the United States. The CDC plays a key role in issues related to emerging infections by developing and implementing infectious disease surveillance and laboratory activities and providing an initial rapid response capability. A short example of the different survey programs conducted by different organizations/groups and potential benefits to disease control are listed in Table 1.2.
| Epidemiological parameter | Organization/tool that measures the parameter | Purpose/benefits |
|---|---|---|
| Emergence of new zoonotic and vector-borne diseases |
| Early identification of possible zoonotic emergence and the exact mechanism responsible for its initial transmission |
| Case information |
|
|
| Laboratory diagnostic tools (monitoring test results) |
| Improvement of the accuracy of diagnostics and the introduction of new technologies and diagnostic systems |
| Tracking and monitoring disease |
| Statistic information on basic epidemiological parameters such as prevalence, hospitalization, death rate, and demographic information |
| Novel disease contact tracing |
| Early detection of clinical manifestations, such as fever |
| Social and cultural response, such as willingness to accept a COVID-19 vaccine |
| Essential for pandemic control, disease management, and transmission reduction |
| Immune protection at public and individual levels |
|
|
| Vaccination monitoring |
|
|
Progressing from Response to Pandemic Control
The main strategies to manage the pandemic have evolved since the initial phases of the crisis. Currently, the approach is based on the combination of control measures directed at creating global immunity, primarily through effective vaccination, monitoring the emergence of new variants, and assessing pandemic progression through the appearance of new outbreaks, breakthrough infections, and the impact of long COVID.
Challenges for the global control of COVID-19 remain at the forefront of anti-COVID-19 activities and countermeasures. Testing still plays a major role in pandemic control. However, despite the hundreds of brands of tests available, difficulties with testing remain in many areas, particularly in low- and middle-income countries, due to a lack of infrastructure for countermeasure implementation and global competitive pricing for access to diagnostic kits and supplies.
Studies on the effectiveness of testing have expanded to areas such as diagnostics in clinical practice, screening of populations at an increased risk of acquisition and transmission, and public health in terms of testing travelers, testing in schools, and testing large communities. The impact of home tests and over-the-counter kits has been quite significant in terms of increasing the numbers of asymptomatic individuals taking tests and confirmed cases. Furthermore, comprehensive contact-tracing programs with testing and effective isolation or quarantine have been crucial for successful outbreak control.Reference Peeling, Heymann, Teo and Garcia46
WHO COVID-19 Dashboard
One example of a publicly available surveillance system is the WHO COVID-19 dashboard, which has provided official daily counts of COVID-19 cases, deaths, and vaccine utilization reported by countries, territories, and areas since early 2020. Data interpretation, especially at the early stage of a pandemic, needs to be taken as a partial overview of the developing pandemic, because the data provided by some countries may be incomplete or of variable integrity. While steps are taken to ensure accuracy and reliability, all data are subject to continuous verification and change. Despite some deficits, the WHO dashboard has been very useful for clinical management, monitoring pandemic evolution, and measuring the effectiveness of vaccination programs. At the time of writing of this book, there are 769 774 646 confirmed cases of COVID-19, including 6 955 141 deaths (as of August 25, 2023). A total of 13 498 570 620 vaccine doses have been administered (as of August 25, 2023). Updated global data are available at covid19.who.int.
Surveillance of pandemic parameters conducted at various phases helped to assess the COVID-19 pandemic evolution, decode processes of transmission, and control spreading. Modifications and adaptations of surveillance programs were necessary to respond to evolving needs through the various pandemic phases (i.e. from antibody and PCR testing to adverse events following immunization and the acceptance of vaccination). Surveys of the multiple social, medical/scientific, epidemiological, and environmental components require significant participation of public health systems and cooperation with government and political organizations. While the information gained in the initial phases was very useful, at the same time, informal or poorly structured and conducted surveys provided information of lesser quality. Overall, the major constraints were associated with data collection, analysis, interpretation, and, more importantly, data integration and distribution. The latter remains a major challenge and certainly needs to be strongly considered during future pandemic and epidemic conditions.
What Went Wrong?
Reflections on the events of the COVID-19 pandemic – the largest medical-social global crisis of modern times – provides great insights into the areas that were successful and those that failed. A prime example of such reflection on a global scale can be seen in the IPPPR’s May 2021 report.47 The IPPPR is an independent panel that was established in May 2020 by the WHO Director-General to construct an evidence-based course for the future based on lessons learned from the past and present to ensure that nations and international organizations, specifically the WHO, successfully address health risks.
The IPPPR’s May 2021 report outlined key errors within the COVID-19 pandemic response:
Warning signs from previous pandemics were ignored. These included the SARS-CoV epidemic (2003), the H1N1 influenza pandemic (2009), the Ebola outbreak in West Africa (2014–2016), and the Zika virus and MERS-CoV outbreaks. The SARS-CoV outbreak led to an update of the IHR in 2005. Several recommendations added to the 2005 IHR were never implemented.
Pandemic preparedness was underfunded. A great opportunity exists to improve the capacities and capabilities of underserved populations.
No appropriate system of zoonotic disease surveillance was implemented. The necessity of such a system is heightened, as most new pathogens are zoonotic in origin due to increasing deforestation for land use and food production.
The message from the WHO when declaring the PHEIC fell short of communicating the severity of the COVID-19 threat. As a consequence, the international response was divided: proactive countries were successful and those that denied and delayed were unsuccessful. The declaration of a PHEIC did not lead to an urgent, coordinated, worldwide response. The IPPPR concluded that February 2020 was a lost month of opportunity to contain the outbreak. There was a worldwide shortage of equipment, supplies, diagnostic tests, funds, and workforce, which led to health-care systems and health-care workers not being properly prepared to face a prolonged crisis. The bureaucracy of many governments was too slow, with governments taking actions only when the WHO declared a pandemic. The panel stressed that measures could and should have been taken to eradicate the epidemic and prevent the pandemic.
Successful vaccine development with initial shortages introduced vaccine nationalism, leading to high-income countries purchasing doses to cover 200% of their population, while the program COVAX – launched by the WHO and partners to equitably deliver vaccines – failed to achieve its goal.
Among other recommendations, the IPPPR report highlighted the need for an improved system for surveillance and alerts that works at a speed that can combat viruses such as SARS-CoV-2. The report also recommended that authority be given to the WHO to publish information and dispatch expert missions immediately.47
At the national level, the United States was lacking a national strategic pandemic plan that was subscribed to by major stakeholders, including multiple government agencies; health-care, public health, and professional organizations; industry; and socially relevant entities. Such a national plan should clearly define the capabilities, capacities, and responsibilities of operating groups and the coordination of the various components.
As the COVID-19 pandemic progressed, many new challenges arose. Thus, in addition to an initial national pandemic plan, a committee needs to be established to monitor and synchronize pandemic-related policies.
A lack of strong leadership was revealed at multiple levels, both internationally and at the domestic level, by the delayed response and implementation of countermeasures. The mismanagement of human circulation with poor control of air traffic and trade activities failed to stop the virus from spreading soon after the outbreak. Additionally, leadership was varied in terms of public health communications, with messaging often conflicting.
Finally, pandemic education was lacking in many populations. Pandemic education should provide correct and accurate information on disease countermeasures. This information can be delivered through social media and diverse instruction campaigns at work sites, schools, churches, and community centers. Strong education programs on vaccine benefits are particularly needed to counterbalance negative opinions on vaccinology that have been so detrimental to society. Can COVID-19 vaccination perception change and become a social norm in the same way that society has adopted wearing seatbelts, stopping at red lights, wearing bike helmets, and living in smoke-free environments? In the same way that these behaviors have become social norms, we need society to view COVID-19 vaccination as another such social norm before full global vaccination can be reached. It should also be remembered that smallpox and poliomyelitis were globally controlled and are in the process of eradication thanks to vaccination.
Lessons Learned
Recognizing the failures presented in the previous section, we must now look toward implementing the following lessons learned to prevent these failures in the future:
aim for early recognition of infectious ailments with unique clinical manifestations different from known diseases
monitor symptomatology and gather all clinical information to develop databases
report all suspicious or confirmed infectious diseases immediately to health authorities and international health forums
attempt to identify and isolate the agent microorganism(s)
identify the origin of clusters of cases
assess disease infectivity and human-to-human transmission
promote and implement sanitary measures and recommendations, starting from universal countermeasures
establish surveillance systems of the severity of the outbreak and its impact on health at individual and social levels
provide clear control indications based on the emergent conditions of the disease
upon declaration of a pandemic, consider the spread of disease and transmission to different geographies and continents
develop surveillance programs in different areas related to patient care, disease spread, control countermeasures, diagnostics, therapies, and vaccination programs, and secure appropriate data analysis, integration, interpretation, and broad distribution as required
set up pandemic/endemic oversight committees at the national and international levels to manage information, announcements, and countermeasures for disease control
promote information notification and diffusion among different countries and communities
maintain the fitness of health systems to meet the health needs associated with the crisis
develop robust programs of pandemic control in coordination with national and international health organizations (the WHO, CDC, CCDC, the UK health system, and country health ministries)
demonstrate robust leadership by prominent representatives of the various crisis constituents and elected and nonelected governmental officials through strong commitment and conviction
develop strong policies to tackle inequalities – the COVID-19 pandemic demonstrated how rich countries put their interests ahead of those of low- and middle-income countries, putting “their relationship with the big pharma ahead of ending this pandemic.”Reference Mahase48







