



Introduction
Hepatitis B virus (HBV) infection is a leading cause of morbidity and mortality globally, with most of the disease burden attributable to the late outcomes of chronic infection [1]. Acute infections are often self-limiting, but can also, in rare instances, lead to death. Of the estimated 257 million people living with chronic HBV infection in 2015, around a quarter of the infections were in women of reproductive age who could transmit the virus to their babies [1]. Infections acquired perinatally and in infancy lead to chronic infection in about 95% of cases with a higher risk of developing sequelae in later life than those infected as adults [2]. Since the 1980s, vaccination programmes have been pivotal in decreasing the incidence and seroprevalence of HBV in younger cohorts worldwide [1, 3].
There are an estimated 4.7 million people currently living with chronic HBV infection in the European Union (EU)/European Economic Area (EEA) and United Kingdom, corresponding to an overall seroprevalence of hepatitis B surface antigen (HBsAg) of 0.9% [Reference Hofstraat4]. The situation is, however, heterogeneous with the estimated prevalence in the general population ranging from 0.1% in Ireland and Norway to 4.4% in Romania [Reference Hofstraat4], and much higher among at-risk groups [Reference Falla5, Reference Falla6].
HBsAg seroprevalence among people in prison in the EU/EEA has been reported to be high with estimates suggesting approximately one in four individuals in prisons chronically infected with HBV in some countries [Reference Falla5]. People in prison often have multiple existing risk factors associated with HBV infection. Demographically, prison populations include social groups also known to be disproportionately affected by HBV, especially migrants [Reference Aebi and Tiago7] from endemic countries who are likely to have acquired it earlier in life. People in prison, however, are at further risk of acquiring and transmitting the infection while incarcerated due to factors such as unsafe sexual practices and injecting drug use (IDU) [Reference Moazen8, Reference Mason9].
In line with the Global Health Sector Strategy (GHSS) on viral hepatitis 2016–2021 [10], the Action plan for the health sector response to viral hepatitis in the World Health Organization (WHO) European Region (2017) set regional targets to be met by 2020 as milestones towards the elimination of viral hepatitis as a public health threat by 2030 [3]. This entails advancing universal vaccination programmes with three doses of HBV vaccine alongside birth-dose vaccination; diagnosis of chronic HBV infection; treatment of eligible HBV patients and scaling up of harm reduction services. Yet in most European countries, key interventions have persistently been reported to have limited coverage or be unavailable in prisons settings [3, 11].
The overall aim of our study was to identify actions that are necessary for progress towards elimination of HBV in the region. Here, we describe current data on HBV disease burden and relevant measures in prisons across EU/EEA countries and United Kingdom to provide a better understanding of the current epidemiological situation and the responses in place. This paper builds on our previous analyses pertaining to the healthcare administration, population and hepatitis C virus (HCV) infection in EU/EEA and United Kingdom prisons [Reference Nakitanda12].
Methods
Study design and setting
A retrospective analysis of data submitted to the WHO's Health in Prisons European Database (HIPED) [13] by 30 EU/EEA countries and United Kingdom.
Data and data sources
Data collected through the National questionnaire for the minimum public health dataset for prisons in the WHO European Region in 2016/2017 for EU/EEA countries and United Kingdom were considered and were extracted from the HIPED on 1 March 2020. These data were provided by national focal points from participating Member States and included public health indicators ranging from prison population statistics, the prison healthcare system, prison risk factors, disease screening and treatment of communicable diseases, among others. Seroprevalences were based on HBsAg and antibodies to HBV surface antigen, however, the latter was not included in our analyses.
Supplementary data on HBV epidemiology in prisons were obtained from European Centre for Disease Control's (ECDC) online prevalence database of infectious diseases [14]. The database contains peer reviewed literature on studies reporting on the prevalence of HBV published between 2005 and 2017, collated and appraised through a systematic review [15]. HBV prevalence data were downloaded from the ECDC database on 1 March 2020 in CSV format, and only included measures of HBsAg.
The detailed methodology of these two projects have been published elsewhere [14, 16].
Data analysis
Data management and statistical analyses were performed using Microsoft Excel (2016). Maps were constructed using the ECDC Map Maker, EMMa [17].
Results
The HIPED did not contain data from Austria, Greece, Hungary, Liechtenstein and Luxembourg; while subnational data were available for Germany. In addition, there were no data on HBV treatment or prevention of mother to child transmission (PMTCT) strategies in the HIPED.
Prevalence of HBV
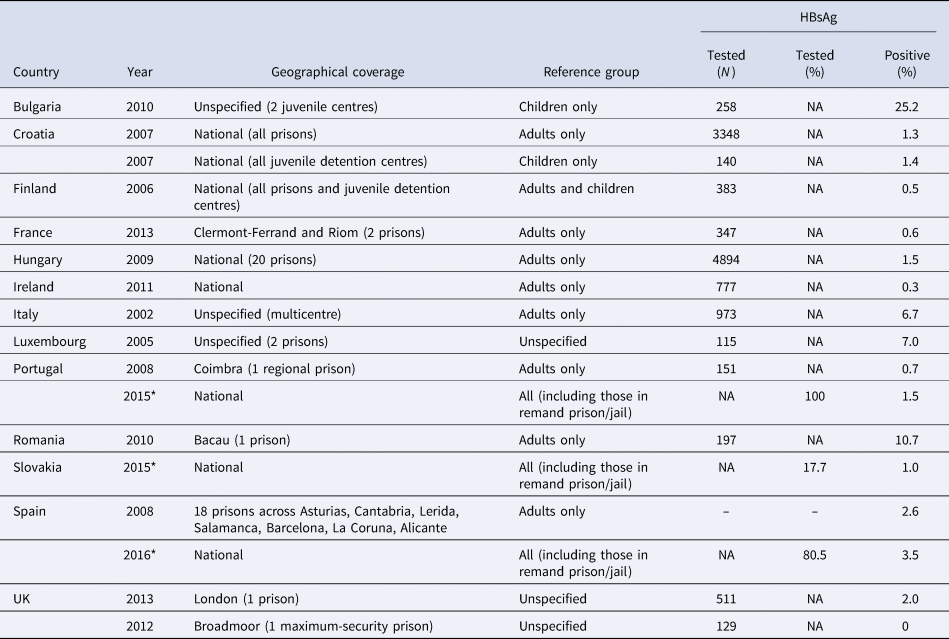
Combined, national and/or subnational data on HBsAg seroprevalence in prisons were available for 13 counties from the HIPED and ECDC databases (Table 1). The HBsAg prevalence ranged from 0% in one maximum-security prison in United Kingdom to 25.2% in two Bulgarian juvenile detention centres.
Table 1. Prevalence of HBsAg in prisons, EU/EEA and United Kingdom (UK)

Sources: ECDC Hepatitis B-prevalence database (year denotes final year of sampling) and HIPED*.
–, no data; NA, not applicable.
HBV screening and vaccination
Twenty-five of the 26 countries reported having HBV screening programmes for people in prison. In 13 countries, screening was reported to be available but not mandatory, while in eight it was routinely offered to all individuals (Opt-out). Risk-based screening was reported in two countries: on clinical suspicion in Lithuania; and for drug users, sex offenders, drug dealers and foreign nationals in Slovakia. In Czech Republic, it was reported as mandatory for all people in prisons (Fig. 1). For Germany, screening was mandatory in Bavaria only, of the 16 federal states. Although it was available but not mandatory in eight states, screening was routinely offered on an opt-out basis in seven states. Cyprus did not report on HBV screening.
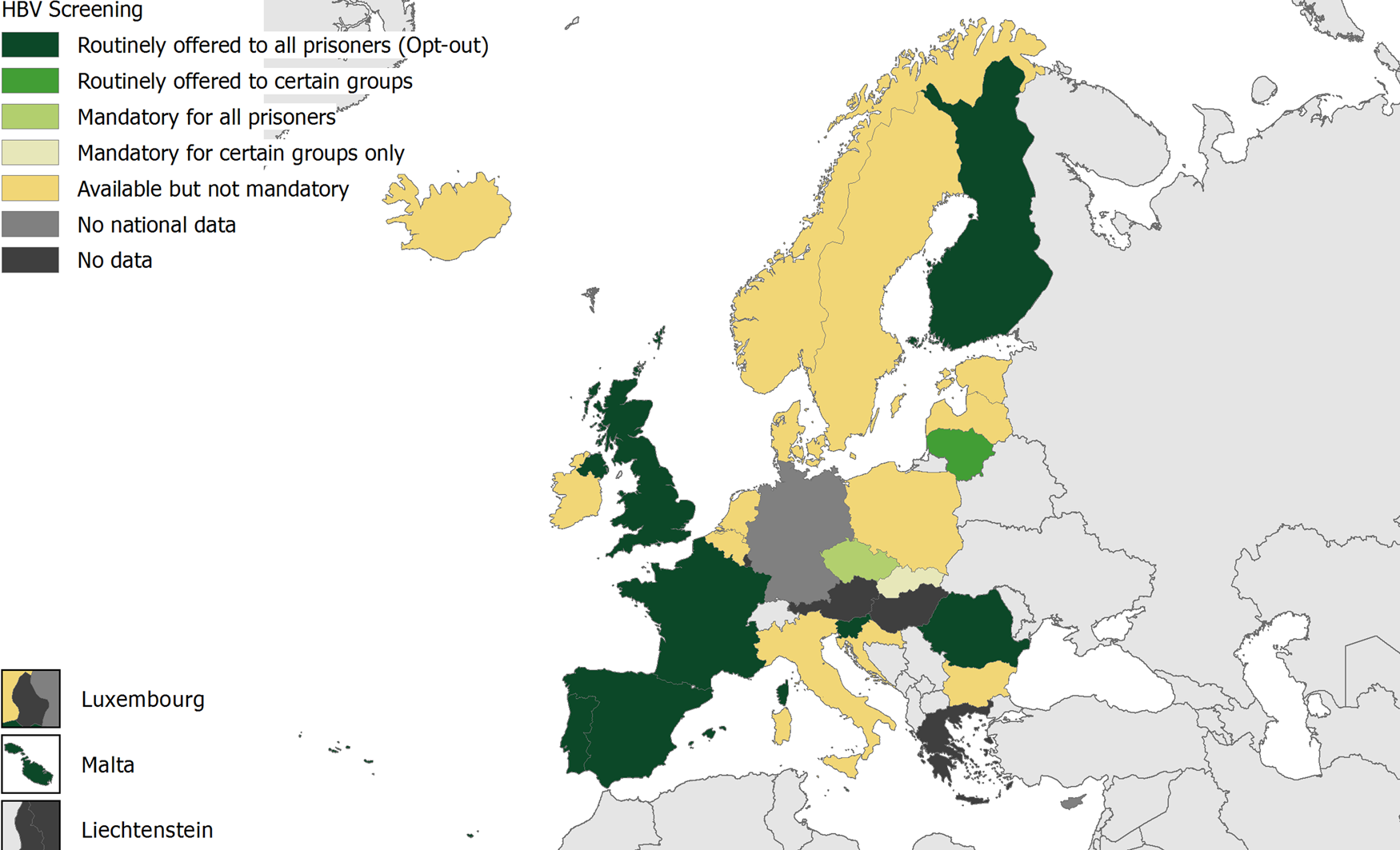
Fig. 1. HBV screening in prisons, EU/EEA, 2016/2017. Source: HIPED.
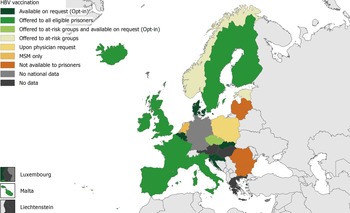
Of the 26 reporting countries, vaccination programmes in prisons were reported as available by 21 countries. In four countries: Bulgaria, Latvia, Lithuania and Romania, HBV vaccination was not available to people in prison. Among the five countries that reported availability on opt-in basis, Czech Republic additionally offered vaccination to at-risk groups. In two countries, it was only offered to at-risk groups. It was additionally offered to at-risk groups in Czech Republic (Fig. 2). In 10 countries, vaccination was offered to all eligible individuals. In the Netherlands, HBV vaccination is available for men who have sex with men only and in Poland, upon request by the physician. Two countries had HBV vaccination coverage data in prisons. In Estonia, 96 people in prisons had received HBV vaccination in 2016, while 66% of all people in Swedish prisons were known to be vaccinated against HBV in 2015. Of the 16 federal states in Germany, nine offered vaccination to all eligible individuals on an opt-out basis; and five offered to high-risk groups. HBV vaccination was available on request (opt-in) in one state, and for medical indications in a further state. There were no data on HBV vaccination for Cyprus.
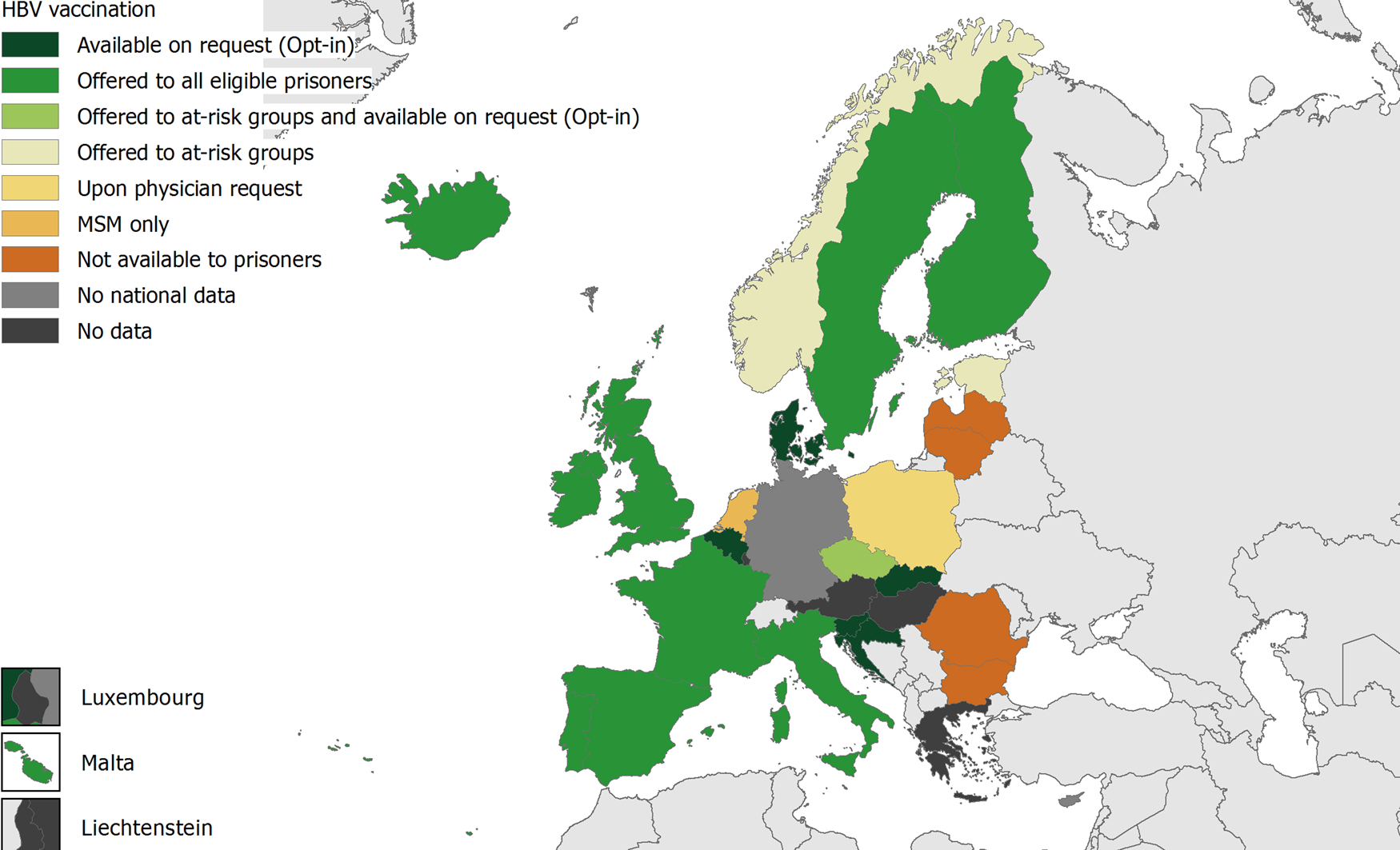
Fig. 2. HBV vaccination in prisons, EU/EEA, 2016/2017. Source: HIPED.
Prevention of sexually transmitted infections and blood-borne viruses (BBVs)
A total of 26 countries provided data on the availability of disinfectants, condoms and lubricants in prisons in the HIPED database.
Disinfectants were reported as being available in all prisons in eight countries (Bulgaria, Denmark, Finland, Italy, Lithuania, Portugal, Spain and United Kingdom – England and Wales) of which six offered it free of charge. In France and Norway, disinfectants are available in more than half of prisons free of charge. Twelve countries reported not providing disinfectants. Cyprus, Estonia, Germany and the Netherlands did not have national-level data. Germany indicated that disinfectants were not available in all prisons in all federal states except for Thuringia.
Condoms were reported to be available in all prisons by 16 countries, of which 12 offered it free of charge. France and Iceland availed condoms in more than half of all prisons in the country free of charge, while Romania and Sweden provided condoms free of charge in less than half of all prisons. Five countries: Cyprus, Ireland, Italy, Latvia and Poland, did not provide condoms in prisons. In 12 German federal states, condoms were available in all prisons free of charge. Condoms were available free of charge in more than half of all prisons in one state; and were reported as unavailable in two. Saarland did not provide state-level data.
Lubricants were unavailable in prisons across 11 countries. Belgium, Bulgaria, Spain and United Kingdom reported availability of lubricants in all prisons free of charge, while lubricants were available in all prisons in Slovakia but not free of charge. They were also available free of charge in less than half of prisons in France, Romania and Sweden. Denmark, Finland, Germany, Lithuania, the Netherlands and Norway did not have national-level data on the availability of lubricants in prisons. For Germany, lubricants were available in all prisons in eight federal states, of which four provided at no cost. One state provided lubricants in less than half of prisons, at no cost. Lubricants were reported as unavailable in four states, while three did not have state-level data.
Twenty-six countries provided data on unsupervised family/partner visits with the possibility for sexual intercourse. These visits were allowed in all prisons in 10 EU/EEA countries, in more than half of prisons in six countries and in less than half of prisons in three countries. Such visits were not possible in six countries: Bulgaria, Cyprus, Ireland, Italy, Slovakia and United Kingdom. Subnational data were available for Germany with four states reporting such visits possible in all prisons; one state reporting possibility in more than half of prisons; and in less than half of prisons in seven states. Partner visits were not possible in two states.
Discussion
People in prison have been known to be disproportionately affected by viral hepatitis in the EU/EEA and are a priority population for interventions for the prevention and control of these infections. To demonstrate progress towards the 2020 targets set in the European action plan specifically for HBV infection, the current study assessed the current epidemiology and response measures targeting HBV in prisons across the EU/EEA and United Kingdom. This assessment aimed to identify gaps in responses to highlight actions necessary to achieve elimination of HBV in the region by 2030 in line with the GHSS for viral hepatitis.
After collating information from two sources: the HIPED and ECDC prevalence database, we still found limited data on HBV seroprevalence in prisons for EU/EEA countries and United Kingdom as only 13 of 31 countries had data available for our analysis. There was also wide variation in the quality and methodologies of these studies, which made the data very heterogeneous. Moreover, there were few recent studies of a robust methodology. At least half of reporting countries only had data covering a sample of all the prisons in the country, and the lack of data for all the countries did not enable any meaningful inter-country comparative analyses of prevalence. Although more recent data were available from the HIPED, only Spain reported on national-level seroprevalence in prisons for 2017, the period in which the survey was conducted. Temporal analyses were also not possible owing to a lack of consistent data over the years. It is likely that the methodological differences between studies account for much of the wide variation in seroprevalence of HBsAg which ranged from 0% in a maximum-security prison in United Kingdom for 2012 to 25.2% in Bulgarian juvenile detention centres for 2010. We also noted that in addition to the seroprevalence of HBsAg in Bulgarian juvenile detention centres being highest among the available data, prevalence in Croatian juvenile detention centres was higher than in adult prisons over the same period of sampling. The limited available data on BBV prevalence among juveniles in prisons restricts the conclusions that can be drawn. However, more attention should be paid to the risks of BBV in juvenile prison population. At the same time, further analysis on risk behaviours and associated harms in adolescent population is needed. These figures also raise concerns of potential gaps in vaccination programmes and increased transmission risk for this particular population [Reference Thompson18], warranting catch-up immunisation programmes and other interventions targeting young offenders during incarceration. The current study invariably suggests that the prevalence of HBV infection among people in prisons across EU/EEA countries and United Kingdom continues to be high compared to previous findings [Reference Falla5] and the general population [Reference Hofstraat4].
Despite the higher prevalence of HBV infection in prison populations, the asymptomatic nature of the disease coupled with suboptimal access to healthcare may hinder diagnosis of HBV. Opt-out testing is a provider initiated service where testing is conducted unless an individual explicitly declines [Reference Rosen19], and there is evidence to show this method has a higher uptake than other modalities for human immunodeficiency virus (HIV) and HCV [Reference Rumble, Pevalin and O'Moore20, Reference Jack and Thomson21]. Recent guidance published by ECDC recommends universal opt-out testing in prisons to ensure timely diagnosis, together with vaccination and/or linkage to appropriate care to prevent the risk of further disease transmission both in and out of the prison setting [11, 22]. Our review found that although most of the EU/EEA countries with available data offered screening for HBV, only eight reported implementing the recommended universal opt-out testing. Moreover, few countries reported data on testing interventions in prisons. Monitoring the uptake of HBV testing underlies all efforts to scale up case detection in prisons to assess progress towards the elimination targets [22–Reference Villar24]. Reducing the undiagnosed fraction of HBV infections is a key priority towards elimination as the GHSS aims to diagnose 90% of viral hepatitis cases by 2030.
Although a promising 21 countries reported availability of HBV vaccination for people in prisons, the full extent of implementation could not be established owing to scarcity of coverage data. In Sweden where vaccination is offered to all eligible individuals, two-thirds of all people in prison were reported to be vaccinated in 2015. This has since been found to be even lower (40.6%, 2017) in Stockholm county prisons [Reference Gahrton25], highlighting potential imbalances or stagnation in the implementation of prisons vaccination programmes. Estonia routinely offers HBV vaccine to at-risk groups, but had issued only 96 vaccines, representing 3.8% of all people in prison [Reference Aebi and Tiago7], in the first half of 2016. Vaccination coverage is unlikely to have reached sufficient levels in European prisons especially among people who inject drugs (PWID), as demonstrated by a recent study in Germany [Reference Haussig26]. A universal prison vaccination programme in Scotland has been found to not only reduce HBV prevalence in prisons, but also led to a reduction in the prevalence of HBsAg among PWID in the communities [Reference Palmateer27]. This highlights the potential for prison-based vaccination to reach hard-to-reach population groups, as many PWID in Europe report at least one incarceration episode in their lifetime [Reference Aebi and Tiago7]. A very rapid scheduling of vaccination may be preferred, considering that release/transfer from/between prisons is a main reason for non-vaccination, and that acceptance may decline with dose [Reference Madeddu28, Reference Stasi29]. At the same time, rolling out global or European vaccination strategies or targets specifically relating to prisons could better inform public health response in this setting.
The global targets for HBV immunisation focus on strengthening of vaccination coverage of infants as this has the greatest impact on the burden of disease and should be the foundation of hepatitis B prevention programmes. In the EU/EEA, most countries have achieved good implementation of childhood immunisation programmes, however, cohorts born before the introduction of universal vaccination can still be vulnerable to HBV infections and thus the European action plan recommends Member States to define country-specific risk groups according to local context and to develop a national policy on targeted vaccination of high-risk individuals against HBV. As the epidemiological evidence presented in this paper indicates, for most countries in Europe, people in prison represent one of these risk groups. In addition, it will be important to adapt and tailor interventions to the needs of specific prison population groups, including among others, women, migrants and juvenile population. In particular, although women constitute a minority proportion (around 5%) of the prison population [Reference Aebi and Tiago7], they present a vulnerable health profile with high rates of IDU and sexually transmitted infections, among other health concerns [Reference Plugge, Yudkin and Douglas30]. Vaccination programmes also need to be scaled up to include prisons staff and in particular, healthcare workers [11, Reference De Schryver31]. The European action plan includes universal HBV vaccination of all children at birth, antenatal screening of mothers, and hepatitis B immunoglobulin (HBIg) (where indicated) to infants of infected mothers, as PMTCT strategies [3]. However, coverage data on antenatal screening and post-exposure prophylaxis in infants born to infected mothers in the prison setting were unavailable. The risk of transmission can also be further reduced by treating infected mothers with antivirals [Reference Brown RS32]. Data on these strategies were also unavailable in the dataset but could be considered for monitoring in the future.
Nosocomial and sexual transmission are the other important transmission routes for HBV infections [33] that have been associated with acute HBV outbreaks, owing to unprotected sex [34] and suboptimal infection control practices in prisons [Reference Hallett35, Reference Hutchinson36]. In the current study, most countries reported the availability of disinfectants, but further details on how these products are used in practice would be useful. The use of bleach or other disinfectants for the purposes of decontaminating injections, body piercing and tattooing equipment in prisons have been found to be not as effective, and the WHO currently recommends disinfectant programmes only as a temporary or second-line strategy to needle and syringe programmes (NSPs) [37]. This could explain why almost half of EU/EEA countries reported not providing disinfectants at all, but also why all countries that reported providing disinfectants (except for Spain) do not have NSPs in their prisons [13]. By 2017, three EU/EEA countries are known to have implemented NSP in their prisons: one female prison in Germany, as well as Spain and Luxembourg across all their prisons [38, Reference Anna Tarján and Stöver39]. At the same time, information on infection control procedures in healthcare services such as the sterilisation of equipment and safety-engineered devices would be useful to improve understanding of practices and progress towards the targets in the European action plan.
With regard to safe sex interventions, condom availability was better than that of lubricants overall, as 21 of 26 reporting countries, compared to only 15 for lubricants, reported availability. This could be an improvement from the situation captured in 2016 by the Dublin monitoring programme for HIV in Europe, when 15 and five EU/EEA countries had effected condom and lubricant distribution in prisons respectively [40]. Sexual transmission is still a major route of HBV infection in Europe [33] and high-risk sexual behaviour, often aggravated by a context of overcrowding, is a recognised risk factor in prison settings [11]. According to the ECDC-European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) guidance on the prevention and treatment of infectious diseases in prison settings, the evidence suggests that provision of condoms and the implementation of behavioural interventions may promote safer sex practices in prison settings [11] and reduce transmission. Our study also revealed the possibility for partner visits and intercourse in majority (>70%) of reporting countries, but other forms of sexual activity including anal intercourse have been reported in the literature [Reference Moazen8, 34]. Condoms promote safer sex [Reference Butler41], and should be recognised as a priority programme for implementation. Importantly, interventions aimed at the prevention and control of HBV infection in prisons have the potential to reach those who may struggle to access services while in the community and to tackle other BBV infections. The prevalence of and co-infection with HIV and HCV, that have overlapping risk factors and modes of transmission [11, 22] as HBV, are also particularly high in prisons [Reference Mason9]. Such interventions may also bring dividends to the overall public health as individuals return to communities upon release from prison. Current European guidance strongly recommends that BBV prevention and control measures be implemented in prisons settings [11].
A major issue of this study related to the data, which we found to be largely out of date and incomplete even after collating the two different sources. This issue was particularly apparent when compared against similar efforts focused on HCV [Reference Nakitanda12]. Although HCV and HBV have been flagged for elimination [10], it appears that availability of epidemiological and monitoring data on HBV in prison settings is lagging behind. We believe this finding calls for careful consideration as it may imply lower interests and efforts in assessing and responding to the burden of HBV among prison populations in Europe.
Data limitations did not allow for additional analyses, such as stratification e.g. by year, age, gender and other potentially confounding parameters, except based on juvenile and adult institutions classification provided in the prevalence data only. On triangulation, we also identified disparities in data reported by EU/EEA countries to HIPED, EMCDDA [38] and other sources [Reference Anna Tarján and Stöver39]. We deduced that such variations could have arisen from differences in reporting periods, reporting authorities and indicators measured due to a lack of a common reporting framework. These data-related issues considerably restricted the possibilities to make temporal, inter-country and data comparisons, as well as our overall interpretation and inferences of the results. In addition to the indicators currently collected by the HIPED, other specific targets and indicators pertaining to HBV treatment, vaccination and other primary interventions directed at PWID and PMTCT, are warranted to allow for a better evaluation of the progress made and gaps hindering the elimination of HBV in the EU/EEA. This could then be aligned with the European-wide monitoring system that has been developed by the ECDC and WHO, whose most recent report also calls for data along the broader HBV continuum of care as most countries are not on track to meet the 50% diagnosis or the 75% treatment target by 2020 [42].
Conclusions
This study upholds existing evidence that HBV prevalence remains high amidst suboptimal coverage of interventions in prisons, as for HCV [Reference Nakitanda12]. Data limitations call for more robust data and a harmonised monitoring system at both national and regional levels [42, Reference Aspinall43] to better understand the current HBV situation in the region within the framework of the European action plan and GHSS. As a key risk-group for viral hepatitis, our findings stress the need for increased public health investments in the prisons setting and inclusion of prisons as a core component of the monitoring efforts as a means to the overall scale up of actions targeting HBV in the region.
Acknowledgements
We thank Carina Ferreira Borges, Programme manager – Alcohol and Illicit Drugs & Prisons and Health Programme at WHO European Office for Prevention and Control of Noncommunicable Diseases; and Emilia Janca (formerly of WHO Regional Office for Europe HIPED team) for data support. We acknowledge members of the HIPED Technical Expert Group (TEG) for their work in supporting the development of the HIPED: Stuart Kinner, Stefan Enggist, Emily Wang, Elmira Gurbanova, Eamonn O'Moore, Jussi Korkeamäki and Seena Fazel.
Author contributions
AON contributed to study conceptualisation, conducted the data management, analyses, interpreted the results and drafted the manuscript. ED conceptualised the study, interpreted the results and provided critical revisions to the manuscript. LT, LM and AM contributed to study conceptualisation, interpreted the results and provided critical revisions to the manuscript. All authors reviewed and approved the final text.
Financial support
None received. Open Access provided by Karolinska Institutet.
Conflict of interest
All authors have nothing to declare. The opinions expressed herein are the authors' own and do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
Ethical standards
Not applicable.
Consent for publication
Not applicable.
Data availability
The datasets analysed during the current study are available in the HIPED, https://apps.who.int/gho/data/node.prisons.All_Countries?lang=en; and the ECDC Hepatitis B prevalence database, https://www.ecdc.europa.eu/en/all-topics-z/hepatitis-b/tools/hepatitis-b-prevalence-database.

 Open access
Open access