



Introduction
Stroke is a major cause of long-term disability. Reference Feigin, Norrving and Mensah1 Cognitive deterioration that results from cerebrovascular disease contributes to a poor functional outcome with reduced quality of life and greater dependence on caregivers and institutionalization. It is estimated that post-stroke cognitive impairment (PSCI) may affect from 20% to 70% of patients in the post-acute stage with great variability between the studies depending of the cognitive evaluation utilized and the post-stroke time evaluated. One year after stroke and even 5 years after stroke, cognitive impairment can still be as high as 22%. Reference Leśniak, Bak, Czepiel, Seniów and Członkowska2–Reference Douiri, Rudd and Wolfe4
All domains may be involved in PSCI, but executive dysfunction appears to be more prevalent. Reference Weinstein, Preis and Beiser5 Ischemic strokes contribute to cognitive deterioration not only through local tissue damage, but neurodegenerative changes can be induced in remote brain regions mediated by a degeneration of neuronal fiber tracts connecting the initial vascular injury with distant gray matter and resulting in focal or widespread loss of white matter and cortical thinning. Reference Dichgans and Leys6
Cognitive changes depend on the time elapsed after the stroke. Some studies suggest that cognitive and psychological dysfunction tends to improve in the first few months after a stroke but then remains stable over the long term. Reference Crichton, Bray, McKevitt, Rudd and Wolfe7,Reference Barker-Collo, Krishnamurthi and Feigin8 A meta-analysis that evaluated the longitudinal course of cognitive function in stroke survivors revealed that cognitive decline seems to become more apparent over a longer follow-up period. The risk factors that have possible association with cognitive decline in stroke survivors are age, sex, stroke location, and medical comorbidities (such as depression). Reference Tang, Amiesimaka and Harrison9 The identification of early predictive factors for PSCI could allow a more differentiated approach to these patients.
The development of acute ischemic stroke treatments provided a great value in the functional outcome of these patients. A secondary analysis of the REVASCAT trial demonstrated the benefit of endovascular treatment (EVT) on executive function. Reference López-Cancio, Jovin and Cobo10 Endovascular intervention has been shown to improve long-term functional independence in patients with acute ischemic stroke (AIS). With this study, we aim to assess cognitive dysfunction in patients, one year after a right anterior circulation ischemic stroke and evaluate the impact of reperfusion time and extent of ischemic injuries in cognitive performance. We postulate that speed treatment in the acute phase of stroke could influence cognitive outcome. We also aimed to evaluate other factors associated with different cognitive outcomes such as age, National Institute of Health Stroke Scale (NIHSS), years of education, modified Rankin scale (mRS), and Age-Related White Matter Changes scale (ARWMC). We aimed for an interval of a minimum of one-year post-stroke to assess cognitive function and evaluate the impact of reperfusion time in cognitive performance, since, according to previous studies, the cognitive impairment caused by stroke would be more stable and apparent. Reference Crichton, Bray, McKevitt, Rudd and Wolfe7,Reference Barker-Collo, Krishnamurthi and Feigin8
Methods
We conducted a retrospective cohort study of patients admitted to the Stroke Service of the Vila Nova de Gaia and Espinho hospital center (CHVNGE), which is certified by the European Stroke Organisation, and where endovascular therapy (EVT) has been performed in the acute treatment of stroke since February 2015. CHVNGE is the reference hospital that covers 15 boroughs in the municipality of Porto, Portugal, representing a population of 306,000 people (2021 Census), of which 21% are older than 65 years and 54% are 25 to 64 years old. It is also a reference center for other cities in the northern and central region of Portugal where local hospitals do not perform mechanical thrombectomy. On average, around 500 stroke patients are admitted to the stroke unit per year and around 200 ischemic stroke patients receive endovascular therapy annually in our stroke unit.
In order to be able to evaluate long-term patients after the stroke but keep the sample as uniform as possible and avoid other confounding factors, we selected only patients 1–3 years after the stroke. The study included all consecutive adult patients with acute ischemic stroke in the right anterior circulation who underwent EVT between January 2018 and August 2020. The aim was to select a relatively homogeneous population regarding areas of cerebral infarction and higher functions affected. Other eligibility criteria were residency within a radius of 40 km from our hospital (as it is easiest to reach by subway or train) and being able to speak Portuguese. Written informed consent was obtained from all participants.
All stroke patients are managed acutely by a stroke physician and every data is recorded in the patient file, as part of the stroke unit protocol, including clinical and neurological exam, National Institute of Health Stroke Scale (NIHSS), vascular risk factors, medication in use, and the time of the symptoms. Other collected data are previous education (defined as the total number of years that participants attended school), mRS, occlusion location, intravenous thrombolysis, and all the times between symptoms and hospital assessment (for example, door-to-needle and door-to-recanalization). Reference Adams, Bendixen and Kappelle11 Thrombectomy technical efficacy was assessed through the degree of revascularization defined at the end of the procedure, using the modified treatment in cerebral infarction (mTICI) scale score of 2b, 2c or 3 – corresponding to reperfusion of at least 50% of the affected vascular territory. Reference Zaidat, Yoo and Khatri12 Given the objective of correlating the cognitive function with the time from the onset of the stroke to the reperfusion, patients with wake-up stroke (WUS) or with unknown last seen well time were excluded from the sample. Left anterior circulation stroke patients were excluded as it has been associated with post-stroke dementia in some studies. Reference Manly, Bell-McGinty, Tang, Schupf, Stern and Mayeux13–Reference Zhao, Biesbroek and Shi15 Additionally, language function is important for performing cognitive tasks, and the selection of right hemisphere strokes reduces the possible confounding effect of language impairment on cognitive performance in this cohort.
Cognitive evaluation was assessed by personal interviews conducted by two members of the team (JN and VB) using the Addenbrooke’s Cognitive Examination-Revised scale (ACE-R), as it is an instrument sensitive to cognitive impairment after stroke, similar to the Montreal Cognitive Assessment Reference Makin, Doubal, Quinn, Bath, Dennis and Wardlaw16–Reference Pendlebury, Mariz, Bull, Mehta and Rothwell18 The ACE-R has 21 questions, covering five different cognitive domains: attention/orientation, memory, language, verbal fluency, and visuospatial skills. A study that assessed the accuracy of the Portuguese version of ACE-R in detecting and differentiating early-stage subcortical vascular dementia from early-stage Alzheimer’s disease revealed that this diagnostic tool is sensitive (100%) and specific (92%) enough to detect vascular cognitive impairments. Reference Gonçalves, Pinho and Cruz19 The total score is 100, and the thresholds used to diagnosis dementia are typically 72/73. Reference Quinn, Richard and Teuschl20 Considering the variability of the value at which dementia is defined, according to age, education, and risk factors, in this work we did not apply standardized thresholds for defining cognitive deterioration and evaluated the absolute value of the ACE-R. This assessment was analyzed by a neuropsychologist (ER).
Brain imaging studies (computed tomography (CT) or magnetic resonance imaging) were performed within 6 months after the stroke and were evaluated by a neuro-radiologist. Age-related white matter changes were recorded, with the ARWMC rating scale. Reference Wahlund, Barkhof and Fazekas21 Statistical analysis was performed using multiple linear regression models with Spearman’s rank correlation to choose variables to be included in the regression analysis. Multiple regression analysis included age, NIHSS, mRS, years of education, time for reperfusion, and ARWMC. The level of significance adopted was 0.05. Analysis was conducted using R 3.6.1 (http://www.r-project.org).
This study was approved by the Ethical Review Board of CHVNGE. Informed consent was obtained from the study participants.
Results
Study Population
Between January 2018 and August 2020, 587 patients with anterior circulation ischemic stroke underwent EVT at our stroke center (Fig. 1). Of these, 261 were excluded because they had a left hemisphere stroke and 167 because they lived further than 40 km from the hospital. From the 159 patients that met the inclusion criteria of the study data, 54 (34.0%) patients were deceased by the time of enquiry; 29 (18.2%) were excluded due to severe comorbidities that conditioned greater dependence and made the transportation too difficult for the family (mRS5); 23 (14.5%) patients refused to participate or could not be located; 9 (5.7%) patients were excluded because of WUS. Forty-four patients were included in the analysis.

Figure 1: Flow chart of patient inclusion and exclusion data. CHVNGE indicates centro hospitalar de vila nova de gaia e espinho and mRS-modified Rankin scale.
The median age of participants was 71.5 (IQR 62.0 – 78.25) years, and 50% (22) were women. The median time after stroke was 28.6 months (IQR 28.6 (18.94 – 31.55). Right-handed patients were 95.5%, and all the patients (despite the predominant hand) had dominant-language localization on the left hemisphere. Demographic, baseline characteristics, and comorbidities of the study population are shown in Table 1.
Table 1: Population characteristics

ACE-R = Addenbrooke’s Cognitive Examination-revised scale; EVT = endovascular treatment, IQR: interquartile range; IVT = intravenous thrombolysis; NIHSS = National Institutes of Health Stroke Scale; mRS = modified Rankin Scale.
Considering the ACE-R thresholds adjusted for the Portuguese population, wherein cognitive impairment is defined as scores falling below 72–73, in our study 70.5% of the population exhibited cognitive impairment.
Twenty-three patients were treated with EVT alone and 21 with intravenous thrombolysis as well as EVT. All patients in our sample had a successful cerebral reperfusion with EVT (mTICI ≥ 2b).
Statistical Analyses
Simple regression linear models were adjusted with the variables that presented significative individual effect with ACE-R. The forward multiple regression analysis was performed to access the relationship between different variables (age, education, time from stroke onset to revascularization, NIHSS at the time of discharge, mRS at three months, and ARWMC rating scale) and the cognitive outcome, measured by the ACE-R. Table 2 illustrates the regression coefficients of the simple and multiple models.
Table 2: Regression coefficients between ACE-R and the different variables
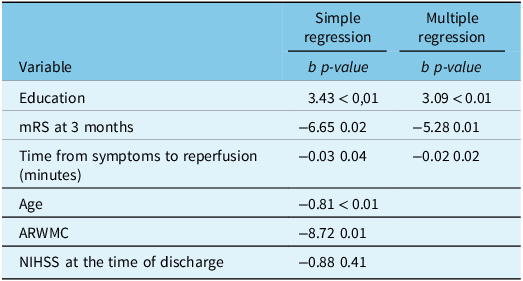
ARWMC = Age-Related White Matter Changes scale; mRS = modified Rankin scale; NIHSS = National Institute of Health Stroke Scale.
Through simple linear regression evaluation, time from stroke onset to revascularization showed a negative influence on the ACE-R (Fig. 2), as well as mRS at three months and ARWMC rating scale. Education showed a positive influence on the ACE-R. The NIHSS at the time of discharge had no statistically significant influence on the ACE-R result (p value 0.409).

Figure 2: ACE-R scores by reperfusion time: crude outcome analysis. ACE-R = Addenbrooke’s cognitive examination-revised scale.
In the forward multiple assessment, keeping all other variables fixed, only time between symptoms and reperfusion, education, and mRS at 3 months revealed a statistically significant influence on ACE-R. Education level presented a strong positive association with ACE-R results (b = 3.0869, p < 0.0001). The mRS at 3 months and the time between symptoms and reperfusion (evaluated in minutes) showed a negative influence on the ACE-R (b = −5.28, p = 0.01; b = −0.02, P = 0.02, respectively). According to these data, for each hour of delay in stroke reperfusion, the ACE score was lower by 1.24 points (60 times the regression coefficient). Collinearity was analyzed with regard to the variables' variance inflation factors. The multiple regression model’s factor standard errors were, at most, 30% of the beta coefficients' value.
Discussion
The main finding of this study was the better cognitive evaluation in patients where reperfusion times were lower, even after a median of 2 years after stroke. Every 48 minutes of delay in endovascular reperfusion corresponded to a decrease of 1 point on the ACE-R. The early recanalization has been associated with favorable clinical response as reduction of lesion volume Reference Albers, Thijs and Wechsler22 and healthy life-years (measured as disability-adjusted life-years). Reference Almekhlafi, Goyal and Dippel23 A possible explanation for that finding is that the early reperfusion of the infarcted area saves the penumbra area from infarction Reference Kumar, Goyal, Sahota and Jain24 reducing the stroke size and consequently the stroke severity which is an important predictor of outcome. Reference Rost, Bottle and Lee25 However, the NIHSS at the discharge was significant only in the univariate analysis. One explanation for that could be the low values of the NIHSS at the discharge and low values at 3 months (not included in the analyses).
The three months functional outcome after the stroke (represented by mRS) was also related to long-term ACE-R. Each additional point on the mRS scale at 3 months was associated, on average, with a score 5.28 points lower on the ACE-R scale. Patients with higher mRS at 3 months have not only motor incapacity but also cognitive impairment that could lead to a higher level of dependency and to a lower quality of life. Delay in thrombectomy times is associated with significant reductions in healthy life-years after stroke. Reference Almekhlafi, Goyal and Dippel23
The most important factor that affected cognition after stroke, however, was the level of education. For each year of education, patients scored on average 3.09 points more in the ACE-R in the multivariate analysis. Lower decline in cognitive function after stroke was associated with higher level of education. Reference Levine, Wadley and Langa26 These results also reinforce the concept that the interpretation of cognitive tests should always be adapted to the patients' education.
The patient’s age and the burden of vascular lesions (analyzed by ARWMC scale) were significant only in univariate analyses, but, after adjusting for other variables, did not show a significant impact on cognition.
The main limitation of our study was the small sample size. We were unable to analyze domain-specific cognitive dysfunction because of that. However, to conduct a personal interview for the cognitive assessment, patient collaboration was necessary. So, first patients with major motor limitations or other severe comorbidities ended up being excluded because they were unable to attend. Second, the interviews took place during the COVID-19 pandemic, and several patients refused to attend for fear of exposing themselves to infection. Third, cognitive assessment is more difficult with a language disorder (aphasia for example), and we selected only patients with right anterior circulation stroke, limiting our sample size. But as left anterior circulation strokes have been more related to global cognitive impairment after stroke in some studies, our study did not add left-sided strokes or patients who had non-dominant language localization to not confound aphasia from language disorder after left-stroke and aphasia caused by cognitive impairment. Reference Makin, Doubal, Quinn, Bath, Dennis and Wardlaw16–Reference Pendlebury, Mariz, Bull, Mehta and Rothwell18 Fourth, given that we are a reference stroke center in our country, many patients come from hospitals that are far, making collaboration for assessment after the stroke more difficult. Fifth, we did not measure the stroke volume, but as the median NIHSS at 3 months was 0 (IQR 0.00–2.00), we assume that the volume lesion was not different between the patients.
In light of the relatively modest sample size within this study, it is important to acknowledge a range of limitations and opportunities for future investigations. Our analysis did not encompass the potential effect of combining EVT and thrombolysis versus EVT alone in predicting cognitive outcomes. Additionally, this study did not explore potential nonlinear relationships between time to reperfusion and cognitive function. Moreover, effect modification by factors such as age, education level, or vascular risk factors was not evaluated. Future research could delve into these potential modifiers and enhance the depth and applicability of our findings in the context of acute stroke management.
The strength of the current study included the uniformity of the analyzed sample, given that the entire population evaluated in this study had a successful recanalization after EVT. The mean age, mortality rate, and time between symptoms and recanalization in our sample were similar to those presented in a recent meta-analysis that evaluated long-term outcomes of mechanical thrombectomy. Reference McCarthy, Diaz and Sheinberg27 Thus, although small, this sample was representative of patients with ischemic stroke undergoing EVT.
Our study used ACE-R as a tool for post-stroke cognitive evaluation as other studies did, Reference Pendlebury, Mariz, Bull, Mehta and Rothwell18–Reference Quinn, Richard and Teuschl20,Reference Mchutchison, Cvoro, Makin, Chappell, Shuler and Wardlaw28 but among patients undergoing thrombectomy, to our knowledge, there are no comparative studies that assessed post-stroke cognitive outcomes according to the time of reperfusion.
Conclusion
Since stroke survival has improved, clinicians are more likely to address the issues of long-term stroke complications, such as cognitive impairment. Cognitive outcome following a stroke is dependent on sociodemographic factors, but the effectiveness of acute-phase stroke treatment has an important role on long-term cognitive outcome. Evaluating post-stroke cognition allows for short- and for long-term preventive measures that diminishes the stroke burden. Interventions that target recognition of stroke symptoms by the general population, as well as a hospital’s fast service for acute stroke treatment, can result in economic and societal gains. Governmental measures all over the world should be taken to ensure education.
Acknowledgments
None.
Statement of authorship
Concieved and designed the analysis: JCN,VB.
Collected data: JCN, ER, VB.
Contributed data or analysis tools: PB, MV, HC, LP, TG, AC, ER, FC, MR, PCP.
Performed the analysis: GCV.
Wrote the paper: JCN, VB.
Revising the manuscript critically for important intellectual content: JCN, VB.
Funding
This research received no specific grant from any funding agency.
Competing interests
None.




