


BACKGROUND
Emergency and trauma care providers face many challenges when caring for injured patients in Canada. Inclement weather, long transport distances, and limited access to resources are some of the potential challenges to trauma management and transport encountered outside tertiary trauma centres. In Ontario, although non-trauma centres receive more than one-half of severely injured patients, there is a dearth of free educational resources addressing community trauma management and transport.Reference Gomez, Berube and Xiong1
Whiteboard videos package concise information with real-time illustration and an accompanying narration. Since the release of the first popular whiteboard video “23.5 Hours” by Dr. Mike Evans, highlighting the health benefits of physical activity for the general public, similar videos have been developed on other health topics.2,3 Although research into the effectiveness of whiteboard videos is limited, initial studies show promising results. A study evaluating information retention and viewer engagement on complex physics topics found whiteboard videos outperformed other formats.Reference Türkay4 Further, when used in healthcare, whiteboard videos improved the process of patient consent and understanding of concepts related to specific medical interventions.Reference Mednick, Irrcher, Hopman and Sharma5,Reference Li, Lee and Vaseghi-Shanjani6 As such, we applied this medium to create a free open-access medical education resource for trauma providers.
PURPOSE
Based on a needs assessment of general emergency departments (EDs) and an expert advisory group through the University of Toronto Trauma program, community pediatric and adult trauma were identified as areas of perceived and unperceived learning need.Reference Li, Lee and Vaseghi-Shanjani6 The primary purpose of this project was to create an educational resource using a whiteboard video to facilitate learning about community adult and pediatric trauma management and transport. Given the broad scope of the subject matter, we focused our content primarily toward physicians.
A secondary objective of our project was to evaluate trauma providers’ perception of the video's effectiveness. This was done through dissemination of an online survey to the study sample using SurveyMonkey® (SurveyMonkey Inc, San Mateo, California, USA). The survey captured participant demographics and perceived video effectiveness and allowed for open-ended feedback.
Description of the innovation
We started the development of this project through the creation of a video working group, consisting of an adult trauma team leader, a pediatric trauma team leader, and an emergency medicine resident. From here, we formed a design committee including both internal and external stakeholders. Internal members within the University of Toronto Trauma program were trauma team leads from adult and pediatric tertiary care centres. The external stakeholders were a group of interprofessional trauma providers (e.g., nurses, paramedics, and physicians) from across Canada. The design committee was involved in content/script development, video design, and dissemination. Eleven key concepts were developed to be covered in the video (Table 1).
Table 1. Eleven key concepts addressed in whiteboard video
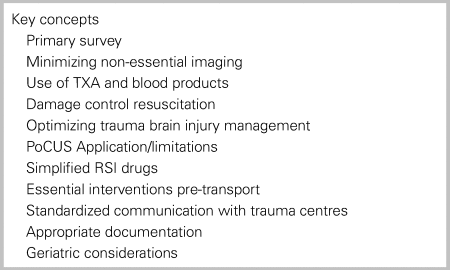
PoCUS = point-of-care ultrasound; RSI = rapid sequence intubation; TXA = tranexamic acid.
The working group merged the finalized script with preliminary storyboard concepts. We partnered with Reframe HealthTM, a third-party production company, to collaborate on storyboards and video animation and record the voice-over narration (Figure 1).

Figure 1. Screenshot of whiteboard video for community trauma management and transport.
We aimed to share the video widely through various communication channels. The video was previewed at the annual Trauma Association of Canada Conference in 2018 and was also disseminated through stakeholders’ professional email listservs and various social media platforms (e.g., Twitter, Facebook, and YouTube). Several professional associations such as Trauma Association of Canada, the Canadian Association of Emergency Physicians (CAEP) newsletter, and free open-access blogs (e.g., Emergency Medicine Cases) posted the video to their site or provided a link to view the video. As of May 15, 2020, the video had garnered over 22,000 views (video link: https://youtu.be/ZZsi_krui-8).
The study's secondary objective was to survey emergency and trauma providers regarding their perceived effectiveness of the whiteboard videos. We obtained 179 survey responses from primarily residents (24.7%) and staff physicians (63.5%) at both tertiary (70%) and community sites (41.7%). Among respondents, 83.2% felt the video improved their understanding of community trauma management (mild improvement 76/179, 42.5%; moderate 61/179, 34.1%; and significant 12/179, 6.7%), and 30% felt it offered practice-changing content. After watching the video, 91% of respondents were motivated to learn more about trauma/transport care, and 86% would watch further whiteboard videos on trauma/transport care. Open-ended feedback provided by survey respondents highlighted two major themes: 1) content specific requests; and 2) more in-depth information on all topics covered in the whiteboard.
DISCUSSION
We created an open-access educational resource for trauma management through collaborative efforts with interprofessional trauma care providers. The video can be shared widely, as the content maintains a balance of general high-yield information for diverse practice environments across Canada.
There are several features contributing to the utility of whiteboard videos as an educational tool. On-demand viewing, paired with sharing across multiple social media platforms, enhances dissemination and learners’ access to the material. The short and concise information, typically less than 10 minutes, specifically addresses the limits of viewers’ attention span.Reference Scott, Albrecht and Given7,Reference Huggett and Jeffries8 The animator's hand displays the image being created, acting as a cueing mechanism to focus the viewer's attention. Additionally, incorporating principles of multimedia learning simplified animations overlaid on a white background and limited text reduce distraction.Reference Mayer9 However, the cost of producing whiteboard videos limits their expanded use as an educational resource. Production companies will typically charge based on video length that can constrain the video's length to fit within budgetary limits.
Our sampled audience perceived the video to be an effective educational resource. To our knowledge, this is the first whiteboard video aimed at physicians to undergo evaluation. A limitation of the study is it is unknown if providers’ knowledge of key concepts improved. The next steps in evaluating the video's educational impact would be assessing knowledge acquisition and retention using pre/post testing. Based on our survey's open-ended feedback, an educational opportunity may exist to build resources for those providers seeking a more nuanced approach to trauma.
SUMMARY
We created a novel whiteboard video to address community trauma management and transport. The video creation process was a collaborative effort with input from a diverse group of community and tertiary trauma care providers. Whiteboard videos are perceived to be an effective tool in medical education that warrant further study. A continued focus should be placed on developing educational resources to improve the delivery of high-quality trauma care in diverse environments.
Acknowledgements
The authors would like to thank Dr. Mark Mensour, Dr. Avery Nathens, Dr. Sandro Rizoli, Dr. Joel Lockwood, Amanda McFarlan, Dr. Joe Nemeth, Dr. Doug Chisholm, Dr. Matt DiStefano, Jasmine Errett, Sherry Armstrong, Dr. Andrew Petrosoniak, and Mike Heinrich for their help in content and script development. We would also like to thank Dr. Sagar Rohailla for help editing the manuscript.
Competing interests
None declared.


